
Abstract
Reactive Attachment Disorder (RAD), is characterized by failure to seek and accept comfort in maltreated children. This lack of activation of the attachment system has profound developmental disadvantages yet, in early childhood, usually resolves quickly after placement in nurturing care. Persistence of RAD into middle childhood has been demonstrated in children reared in Romanian Institutions but, in family-reared children older children, there is controversy regarding whether RAD-like behaviors are genuinely attachment-related and stable from early childhood or are, in fact, related to PTSD. We conducted two pieces of research to investigate this: 1. a systematic review to examine persistence/resolution of RAD and 2. a case series of three boys whose RAD symptoms persisted despite living in placements judged by both social and child health services to be of good quality. Our systematic review revealed a paucity of longitudinal data. Except in atypical institutionalized samples, RAD had not been evidenced beyond pre-school. All three boys in the case series met DSM 5 criteria for RAD in late childhood/early adolescence and had stable RAD symptoms since before age 5. Qualitative interviews with their families revealed common themes of family strain, frustration and resentment at the lack of support from services. This paper provides the first opportunity to generate testable hypotheses about environmental circumstances and coexisting symptomatology that may influence RAD trajectories. Persistence of RAD has profoundly negative implications for children and their families. Recognition of RAD symptoms is challenging but crucial in order to improve care of these children and their families.
Introduction
The diagnostic criteria for Reactive Attachment Disorder (RAD) have been adapted various times since it was first defined in 1980, and “failure to seek and accept comfort” are now considered to be its core symptoms (American Psychiatric Association, 2013). RAD was previously categorized as one of two “Attachment Disorders” with two subtypes: Inhibited Reactive Attachment Disorder (I-RAD) and Disinhibited Reactive Attachment Disorder (D-RAD). These are now considered to be two distinct disorders. RAD, previously I-RAD, is still considered a disorder of attachment since failure to seek/accept comfort is essentially a shutting down of the attachment system (Groh et al., 2017; Yarger et al., 2016). Disinhibited Social Engagement Disorder (formerly D-RAD) is characterized by indiscriminate friendliness—a behavior not directly related to the primary attachment relationship—so DSED is no longer considered a disorder of attachment (Bruce et al., 2019). In this paper, we do not consider DSED, but focus solely on the DSM 5 definition of RAD.
RAD is characterized by significant difficulties with social relatedness in most contexts, appearing before the age of five (American Psychiatric Association, 2013). The behaviors are thought to develop as the result of persistent caregiver neglect, abuse and a lack of opportunity to develop consistent attachments. This disorder of attachment means a child does not initiate appropriate social interactions, especially in stressful situations and, if approached, may respond in an inappropriate manner e.g. withdrawal, high levels of fear or unpredictable reunion responses with caregivers (Humphreys et al., 2017).
RAD is associated with social, emotional, physical and developmental disadvantage (Helen Minnis et al., 2013; Humphreys et al., 2017; Kay & Green, 2013; Prior & Glaser, 2006). The few studies of RAD in older children or adolescents have found an association with psychiatric disorders including attention deficit hyperactivity disorder (ADHD), post-traumatic stress disorder (PTSD), anxiety, conduct disorders (Moran et al., 2017) and emerging personality disorder (Giltaij et al., 2017). These studies, of family-reared older children, do not include data on these same young people in the pre-school years, so it is impossible to be certain that their symptoms occurred before the age of five or that the symptoms seen in adolescence are, in fact, RAD. Assessment of RAD in older children is challenging and controversial, since attachment-related symptoms differ greatly in the teenage years (Lehmann, Monette, et al., 2020).
Longitudinal studies of RAD are very limited. We were aware that the persistence of RAD behaviors into middle childhood had been demonstrated in a randomized controlled trial of an institutionalized population, in children who had been given a diagnosis of RAD in the pre-school years. RAD behaviors persisted, to some extent, even in those randomized from the institution into nurturing foster families—but all participants had been exposed, in early life, to the uniquely severe emotional neglect that characterized Romanian orphanages under Ceausescu (Zeanah et al., 2017). A recent narrative review from the same group expressed doubt that, even in this institutionalized sample, “any of these children reached the diagnostic threshold” (Scott et al., 2018).
The natural history of RAD is therefore in doubt. Firstly, although adolescents have been described with RAD-like symptoms, including failure to seek and accept comfort, there is controversy as to whether this is, in fact, RAD or might have another non-attachment-related etiology e.g. PTSD (Lehmann et al., 2020). Secondly, older children and adolescents with RAD behaviors have either experienced very extreme early adversity (Zeanah et al., 2017) or have never experienced stable, nurturing care (e.g. Kay & Green, 2013; Moran et al., 2017).
The paper’s senior author leads a clinical and research team focusing on children and young people who have experienced abuse and neglect. In line with the experiences of other research and clinical colleagues, our impression is that RAD in infancy and the pre-school years often resolves quickly when the child is placed in nurturing substitute care and is rarely seen clinically in older children living in nurturing families. However, we have noticed that when RAD does present clinically in older children, failure to seek or accept comfort has rarely been previously commented upon (e.g. in social work or child mental health notes) and the child usually only presents once associated behavioral problems have become extreme or relationship problems have become unmanageable. It is not uncommon, in our clinical practice, to see RAD-like behaviors in older children who have experienced inadequate care throughout their lives, but it is usually impossible to be certain that these behaviors have persisted since early childhood and are truly indicating attachment-related symptoms, not simply related to PTSD (Lehmann et al., 2020).
Two research questions arise from this: Can the longitudinal course of RAD be traced from early childhood into middle childhood and adolescence—beyond institutionalized samples? Can RAD, in older children and adolescents, persist despite stable nurturing care?
These are crucial questions for several reasons: firstly, RAD usually resolves quickly when noticed in early childhood; secondly, its core symptoms of failure to seek and accept comfort seem to be usually missed in older children; thirdly, older children and adolescents with RAD symptoms seem to rarely present to services unless challenging behaviors are also present. Lastly, and most importantly, RAD behaviors in older children tend to be associated with co-occurring psychiatric diagnoses and significant functional impairment that often includes breakdown of care placements and youth justice involvement (Kay & Green, 2013; Moran et al., 2017).
To address these research questions, we first conducted a systematic review to find out whether any previous studies had examined persistence/resolution of RAD in family-reared children, and to examine factors associated with RAD behaviors across childhood and adolescence. Secondly, we conducted a case series, following CARE guidelines (Gagnier et al., 2013), focusing on the handful of cases of persistent RAD seen in our clinic over the years where RAD symptoms had clearly been present, despite nurturing care, from infancy through to later childhood. For rare disorders like RAD, traditional epidemiological studies are not possible so case series can provide the most robust methodology available (Gagnier et al., 2013).
Systematic literature review
Review methodology
Following PRISMA guidelines (Liberati et al., 2009), an electronic search of the following databases was conducted: MEDLINE, Psychinfo, PsychARTICLES, Web of Science, British Library Ethos, PubMed, Google Scholar and Embase.
Inclusion criteria
Articles that directly explored factors associated with inhibited attachment disorder Articles that are written in or have been translated into English Articles published between 2004–2019 including unpublished studies
Exclusion criteria
Previous reviews, book chapters, and case studies Qualitative research
34 papers were included and scored using Crowes Critical Appraisal Tool (CCAT v1.4), which scores design, sampling, results etc, with higher scores indicating a higher assessment of quality overall. In line with the tool’s guidelines a score of <20 is considered low quality, a score of 20–29 moderate quality and a score of 30–40 high quality. 20% of articles were rated independently by RN and GC, with good agreement. Rating discrepancies or challenges were agreed in consultation with a third, more experienced, reviewer (HM).
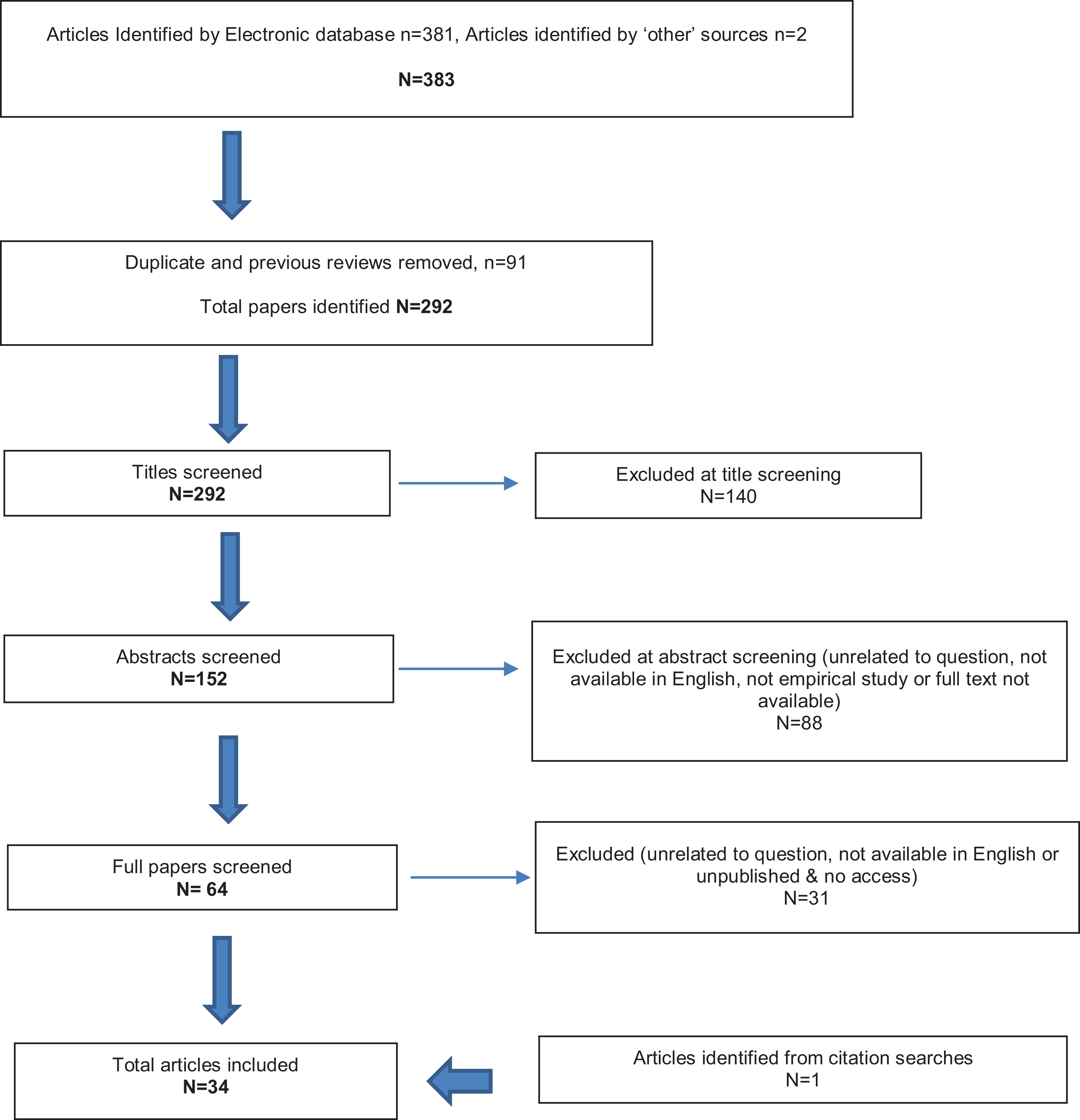
Flowchart showing inclusion and exclusion of articles during literature review, total articles included (n = 34).
Review findings
The 34 reviewed studies are summarized in Appendix. The literature was of moderate to high quality. The commonest methodological problems were small and/or poorly representative samples (Table A1).
Both individual and contextual factors were associated with RAD. Contextual factors included institutionalization (Humphreys et al., 2017; C. H. Zeanah, A. T. Smyke, S. F. Koga, & E. Carlson, 2005); quality of caregiving in the institution (Corval et al., 2017; Gleason et al., 2011; McGoron et al., 2012; C. H. Zeanah et al., 2005; P. Zimmermann & Iwanski, 2019); placement moves (Upadhyaya et al., 2018); harsh parenting, parental negativity (H. Minnis et al., 2007); parental mental health problems (Lehmann et al., 2016; Zeanah et al., 2004); maternal smoking; single motherhood (Upadhyaya et al., 2018); paternal age (Upadhyaya et al., 2018) and longer exposure to the maltreating pre-care environment (Jonkman et al., 2014). Individual factors included male gender (Lehmann et al., 2016); reduced gray matter volume (Fujisawa et al., 2018; Shimada et al., 2015; Smyke et al., 2012); lower cognitive ability (Hong et al., 2018; Takiguchi et al., 2015); dopaminergic dysfunction (Gleason et al., 2011; Tomoda, 2016); and genetic factors, particularly for males (Zeanah et al., 2004). RAD was associated with depressive symptoms (Gleason et al., 2011); social and emotional difficulties (Gleason et al., 2011; Hong et al., 2018; Humphreys et al., 2017; Mayes et al., 2017; Moran et al., 2017; Spangler et al., 2019); functional impairment (Gleason et al., 2011; Hong et al., 2018; Lehmann et al., 2016; McGoron et al., 2012); behavioral and conduct problems (Elovainio et al., 2015; Hong et al., 2018; Lehmann et al., 2016; Mayes et al., 2017; Moran et al., 2017; Spilt et al., 2016); hyperactivity (Elovainio et al., 2015; Humphreys et al., 2017; H. Minnis et al., 2007); internalizing symptoms (Elovainio et al., 2015; McGoron et al., 2012; Scheper et al., 2016; Shimada et al., 2015; P. Zimmermann & Iwanski, 2019); externalizing symptoms (Elovainio et al., 2015; Hong et al., 2018; Scheper et al., 2016); stereotypies (McGoron et al., 2012); help seeking from services (Lehmann et al., 2016); callous-unemotional traits (Mayes et al., 2017); emerging personality disorder (Mirza et al., 2016); higher levels of comorbidity (Hong et al., 2018; Mayes et al., 2017) and symptoms of Disinhibited Social Engagement Disorder (DSED) (Gleason et al., 2011; Lehmann et al., 2016; Mayes et al., 2017; McGoron et al., 2012).
The prevalence of RAD varied greatly across studies (Mayes et al., 2017). Of the eight studies that included participants above the age of 12, only four reported on prevalence. Two papers included small sample sizes (n = 29 and n = 10) and noted rates of 10% in young people with both criminal and psychiatric histories and 60% in young people with symptoms of Borderline Personality Disorder (Mirza et al., 2016; Moran et al., 2017). A larger study (n = 200) recorded a prevalence of 9% in home reared children clinically referred for emotional and behavioral problems and 27% in a foster care sample with an age range of 2–7.9 years (Scheper et al., 2016).
Despite variations in sample size, age and type of participants, and measures utilized, the findings regarding factors associated with RAD were largely consistent across studies. However, some studies found an association with RAD and externalizing problems, while two did not (Elovainio et al., 2015; Hong et al., 2018; Jonkman et al., 2014; Lehmann et al., 2016; Mayes et al., 2017; McGoron et al., 2012; Moran et al., 2017; Scheper et al., 2016; Spilt et al., 2016; P. Zimmermann & Iwanski, 2019). Despite a recent surge in the number of papers investigating RAD and associated factors, few follow children from early childhood through to adolescence and those that do are exclusively focused on institutionalized samples. Although there have been no population studies able to give robust prevalence figures for RAD, the literature still considers RAD to be a very rare disorder beyond infancy. The question about persistence/resolution of RAD in family care was not a focus of any of the papers in our review and we found no evidence for or against RAD persisting in children reared in families that are providing nurturing care.
Case study: Presentation, diagnosis and outcome
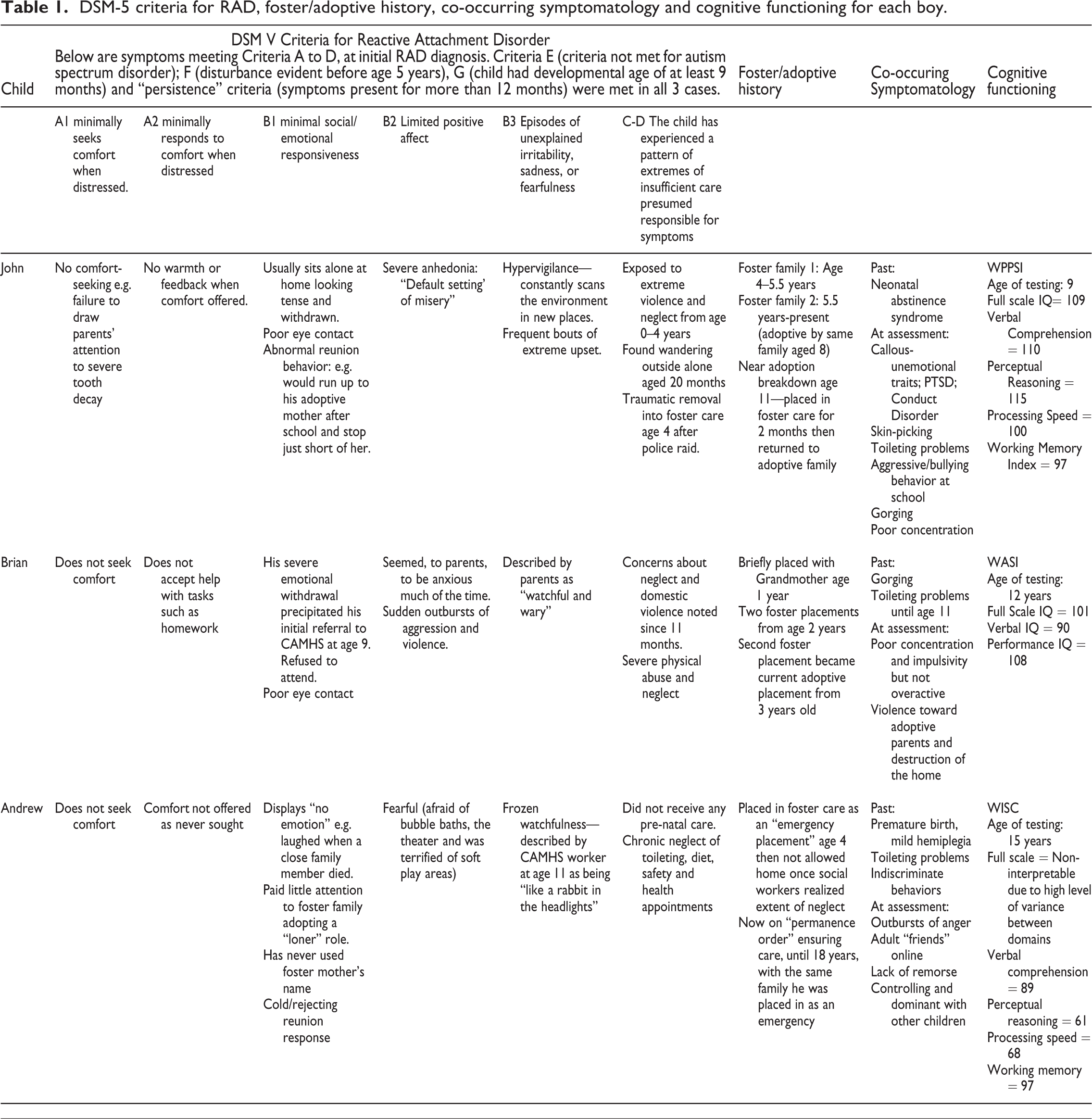
The three boys we describe here are the only children seen, in the team’s > 15 years of clinical experience, with RAD symptoms persisting from early childhood in families objectively judged to be providing nurturing care. All had experienced severe maltreatment in early life and were placed, between age three and five, with adoptive or foster parents who had undergone stringent background checks and had ongoing support. All boys and their families gave informed consent to the inclusion of their case reports. Names have been changed to protect identities. Diagnoses of RAD were made via multi-disciplinary assessment using a standardized observation protocol (McLaughlin et al., 2010) including a semi-structured interview for RAD (Helen Minnis et al., 2013; Lehmann, Meillet, et al., 2018) and face to face clinical assessment (see Table 1). Additional standardized measures examined co-occurring psychiatric disorders (Goodman et al., 2000) and cognition (Wechsler, 2014). Table 1 provides an overview of the DSM-5 criteria for RAD, cognitive functioning, co-occurring symptomatology and foster/adoptive history.
DSM-5 criteria for RAD, foster/adoptive history, co-occurring symptomatology and cognitive functioning for each boy.
Case 1, John
When assessed at age 9, RAD symptoms had been noted by adoptive parents since age 4. In addition, John was diagnosed with PTSD, Conduct Disorder and ADHD. He had intensive relationship-focused psychotherapeutic treatment with his adoptive mother, but symptoms persisted.
Case 2, Brian
When first assessed at age 12, RAD symptoms had been noted by adoptive parents since age 3. At age 13, Brian was moved to a small residential unit where he continued to have problems seeking and accepting comfort from his keyworkers and his parents, who continued to visit. At age 15 he continued to demonstrate RAD symptoms and difficult behavior and was moved into a singleton residential placement, receiving intensive one to one care from a small team of staff. Involvement with his parents increased. By age 16, when last assessed, Brian was no longer violent, no longer met criteria for RAD and was being investigated for possible ADHD.
Case 3, Andrew
When assessed at age 14, RAD symptoms had been noted by the foster carer since age 4 and the foster placement was in jeopardy. Ongoing health concerns relating to his premature birth included mild left-sided hemiplegia, talipes and partial sightedness. At first assessment, his foster carer had never considered whether or how Andrew had sought comfort as a young child, but described how he would stand silently while physical care was provided to other foster children, all of whom had severe or profound physical and learning disabilities.
After two sessions of psychotherapy in which the therapist encouraged Andrew and his foster mother to notice and respond to each other’s signals, symptoms improved markedly. However, significant difficulties still remained that continued to put the security of the placement in jeopardy.
Social communication
In all of the boys, social communication was typical (apart from failure to seek/accept comfort and emotional withdrawal) and none had repetitive or stereotyped interests. None of the boys had symptoms of Autism Spectrum Disorder.
Family perspective
Parents took part in qualitative interviews to explore the impact of RAD symptoms on the family. RN and GC read each transcript independently, then agreed on the main themes (Braun & Clarke, 2014): Three common themes were extracted across all three families
Family strain: High levels of stress characterized all aspects of family life. Burdensome child behaviors included lack of understanding of social cues, violence and eliciting negative attention. There was emotional separation between the child and the rest of the family, described by John’s mother as living “parallel lives; one life with my husband, biological son and dog, and the other with John.”
Frustration: A key frustration for families was lack of understanding of the child’s emotions and the child’s emotional unresponsiveness and abnormal interactions. Another frustration was the significant delay in identification of the problem and the associated lack of support, resulting in years of isolated suffering.
Resentment: Feelings of resentment were evident in all three families due to the significant strain that RAD had put on their family relationships. Both adoptive couples had experienced marital difficulties ascribed to the burden of their child’s problems.
Discussion
Our systematic review showed that our research questions had not been answered by the previous literature. Our case series, however, answered both questions: The longitudinal course of RAD could be traced, in these three family-reared boys, from early childhood into middle childhood/adolescence. The diagnosis of RAD, in these older children and adolescents, persisted despite care that had been objectively judged to be stable and nurturing.
The literature confirms that RAD commonly coexists alongside other psychiatric disorders. Early life maltreatment, institutionalization, and poor-quality caregiving, as well as length of exposure to maltreatment and number of placement moves, were found to be associated with symptoms of RAD in older children and adolescents, even when in nurturing adoptive placements. The literature, however, provided no evidence regarding persistence/resolution of RAD within nurturing families, except in previously institutionalized samples (Elovainio et al., 2015).
There was general agreement across the literature regarding factors associated with RAD but discrepancy regarding the presence of externalizing difficulties (Jonkman et al., 2014; McGoron et al., 2012). The two studies finding no association between RAD and externalizing symptoms recruited very young participants (22–89 months) compared to older samples recruited in other studies (4–17 years) (Hong et al., 2018; Lehmann et al., 2016; Mayes et al., 2017; Moran et al., 2017). This suggests a likely change in the way RAD presents, and the co-occurring disorders that manifest, as the individual develops.
The significant variance regarding prevalence estimates across the identified papers is likely a result of variations in study methodology. Despite this variance, the systematic review confirms that RAD is rare and of low prevalence even in high risk samples.
The Case Series showed that RAD has a profound social and emotional impact on both the children and those caring for them. All cases had associated developmental/neurodevelopmental problems and extremely problematic relationship functioning, as found by previous studies (Helen Minnis et al., 2013; Kay & Green, 2013; Kocovska et al., 2012; Moran et al., 2017). All placements had been threatened with breakdown. This evidence provides a new insight: that persistent RAD, while rare, threatens family life.
Future research will be challenging because of the rarity of RAD. The use of methodologies developed specifically for rare disorders, such as surveillance, will be essential since the negative outcomes of persistent RAD seem to be so profound. Hypotheses raised by our study, for future testing, include: that children with neurodevelopmental disorders who also experience abuse and neglect might be at higher risk of persistent RAD; that persistent RAD symptomatology might lead to extreme family strain and risk of placement breakdown, even in otherwise well-functioning families.
To conclude, in rare cases, RAD can persist despite years of nurturing care, even in children who did not experience early institutionalization. Symptoms are easy to miss, but the families of all three of these boys were experiencing severe family stress. Clinicians should always consider RAD—including careful observation for lack of comfort-seeking—when assessing children with a maltreatment history.
Footnotes
Acknowledgments
Mari Porter, NHS Lothian Librarian, assisted with updating the literature review.
Professor Chris Gillberg reviewed and revised the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix
Details of the reviewed studies.

| Study | Quality Rating | Design | Sample Characteristics | RAD Measures | Results | Strengths and Limitations | |
|---|---|---|---|---|---|---|---|
| Prevalence | Associated Factors | ||||||
| High Quality Studies | |||||||
| 1. Shimada et al. (2015) | High | Cross-sectional, case control study | N = 43 living in Japan RAD group: n = 21 living in care facility; Mean age 12.76 (10–17) years; 62%F / 38%M n = 22 typically developing matched on age and gender; mean age = 12.95 years, 55% F / 45% M |
Clinical judgment by Psychiatrists using DSM-5 | n/a | RAD group had reduced visual cortex Gray Matter Volume (GMV) RAD and GMV associated with SDQ internalizing problems RAD group had sig lower FSIQ, higher levels of psychiatric symptom scores |
Strengths
Control group Fairly large number exhibiting RAD Limitations Small sample size IQ differences between groups No RAD observation data |
| 2. C. Zeanah et al. (2005) | High | RCT—cross-sectional baseline data | N = 145 children in Romania (Bucharest Early Intervention Project; BEIP) n = 95 institutionalized; Mean age 23.8 months (12–31) 45% F/ 55% M n = 50 never institutionalized, living with parents; Mean age 22.25 (12–31) months 50% F/ 50% M |
Disturbances of Attachment Interview (DAI) |
Institutionalized children had higher levels of RAD compared to never institutionalized children. |
Continuous measure of attachment moderately correlated with caregiver ratings of RAD. Quality of institutionalized caregiving was related to RAD No association between length of institutionalization and RAD Regardless of rearing environment, categorical organized attachment was not significantly related to caregiver ratings of RAD |
Strengths
RCT Limitations Coders not completely blind to group status No observational measure of RAD No detailed historical information |
| 3. Gleason et al. (2011) | High | RCT Cohort Study | N = 136 children (BEIP) n = 68 care as usual (institution). n = 68 placed in foster care following institution Mean age at baseline 22 (6–30) months; 50%M / 50% F |
DAI The Preschool Age Psychiatric Assessment (PAPA) |
RAD at baseline (6/130; 4.6%); 30 months (4/123; 3.3%); 42 months (2/125; 1.6%) and 54 months (5/122; 4.1%) Nonsignificant pattern of decline |
RAD and DSED correlated at baseline, 30m, 42m, and 54m. No association between categorical diagnoses No associations between exposure to institutional care and RAD at baseline RAD associated with caregiving quality at baseline, 30m, 42m and attachment security at 42m & depressive symptoms, emotional difficulties and functional impairment at all time points. Contributed to variance on ITSEA competence at baseline, 30m, and 42m but not at 54m. RAD predicted functional impairment at 54m in children in institutions. RAD associated with impairment at baseline, 30m, and 42m. |
Strengths
RCT Various follow ups Observational measures (but not specific to RAD) Limitations As above and low rates of RAD limited statistical analyses |
| 4. Smyke et al. (2012) | High | RCT Cohort Study | N = 208 children (BEIP) Age at baseline 6–30 months, no mean reported. Follow up at ages 30, 42, 54m & 8 yrs n = 68 care as usual (institution): 51%F / 49% M, n = 68 placed in foster care following institution: 50% F/ 50% M, 62% n = 72 never institutionalized: 57% F/ 43% M, |
DAI |
Categorical prevalence not specified. RAD decreased differentially for usual care and foster care groups Differences between foster care group and never-institutionalized group found at baseline, 30m and 8 years. RAD in children placed in foster care <24m did not differ from children placed > 24m of age |
Institution group only, more signs of RAD found in those with lower baseline cognitive abilities across intervention period. |
Strengths
RCT Fairly large sample size Follow ups Limitations As above |
| 5. McGoron et al. (2012) | High | RCT Cohort Study | Total n = 136 children (BEIP) Mean age 22.0 (6–30) months. Follow up at ages 30, 42 and 54 months |
DAI | n/a | Associations between symptoms of RAD at 54 m and 30m caregiving quality, 42m attachment security, 54m DSED, 54m stereotypies, 54m internalizing disorders and 54m functional impairment found Association between 30m caregiving quality and symptoms of RAD at 54m RAD not associated with ethnicity or 54m externalizing disorders |
Strengths
RCT Follow ups Limitations As above and magnitude of associations fairly small |
| 6. Moran et al. (2017) | High | Cross-sectional Study | n = 29 youth justice participants in Scotland Mean age 16.2 years (range 12–17 years) 34% F / 66% M |
Relationship Problems Questionnaire (RPQ) Adapted Child and Adolescent Psychiatric Assessment, Reactive Attachment Disorder (Adapted CAPA-RAD) Adapted Observational Schedule for RAD |
10% had RAD, 21% DSED, 10% mixed RAD/DSED & 10% borderline attachment disorder | RAD associated with SDQ total difficulty scores, hyperactivity, prosocial behavior and conduct problem items RAD not associated with emotional symptoms or peer problems |
Strengths
Power calculation included Observational data Limitations Small sample size Exclusions may limit validity Limited historic information no control group or follow up |
| 7. Zimmerman and Iwanski (2019) | High | Cross-sectional study | N = 62 German children, RAD risk group (N = 32, 66% F) Control group (N = 32) Mean age 7.86 years (5–10) |
RPQ DAI Coding of Attachment Disorder Behaviour in Children (CADBC) |
Significantly higher RAD symptoms in RAD risk group as reported by caregivers compared to nonclinical control group |
RAD risk group reported more observed signs of Internal Working Model and more negative self-concept compared to control group Children with higher RAD symptoms showed increased difficulties with: emotional, conduct and peer problems, hyperactivity and lower levels of prosocial behavior |
Strengths
Multiple RAD measurements Observational data Limitations 1 unvalidated tool |
| 8. Giltaij et al. (2017) | High | Cross-sectional Study | N = 55 children previously screened using DAI & ASD symptoms from previous study Mean age range 10.7 years (5–11), 75% M |
DAI Structured observation: Clinical Observation of Attachment (COA) Clinical diagnosis of RAD made by psychologists based on above measures Case files read for extremes of insufficient care |
Based on DAI—9 children positive for RAD Based on diagnostic information 7 children were diagnosed with RAD, 2 children were diagnosed with DSM-5 RAD only |
High convergence between indicators of disordered attachment |
Strengths
Multiple RAD measures Multiple information sources Limitations Relatively small sample size Drop-out rate relatively high DAI used was developed for children under 5 and not the older, adapted version No control group |
| 9. Fujisawa et al. (2018) | High | Cross-sectional Study | N = 21 children with clinical diagnosis of RAD Mean age 12.8 years (10–17), 13 F 22 control group children (mean age 12.95 years, 12 F) |
None | n/a | GMV significantly reduced (20.6%) in left primary visual cortex of RAD group compared to controls Sensitive period 5–7 years Number of types of maltreatment and neglect had a sig effect |
Strengths
Control group Limitations Small sample size Limitation in RAD diagnosis |
| 10. Split et al. (2016) | High | Cohort Study | N = 85 children with mild to severe symptoms of RAD (age range 6.22–10.39 years) | RPQ Sensitivity and Positive climate of the Classroom Assessment Scoring System (CLASS) |
n/a | Sociobehavioral development with inhibited RAD symptoms is associated with sensitivity of teachers Inhibited symptoms of RAD were associated with more overt aggression and less prosocial behavior |
Strengths
Longitudinal data Limitations Limited information on presence of RAD diagnosis |
| 11. Hong et al. (2018) | High | Routine data diagnostic prevalence study | Nationwide Insurance Data, <10 years old, at least one claim for either RAD or DSED (not diagnosed in past year) | None | Across 2010-2012 newly diagnoses with RAD was the highest for 3-year olds (23.8%), 4-year olds (17.8% and 2-year olds (16.2%) Annual diagnosis of RAD per 1000,000 population was 5.25 (5.39 in 2010, 4.9 in 2011, 5.45 in 2012) |
Comorbid diagnoses: 0–3 years—developmental disorders of speech, language and ASD 4–6 years—mental retardation, behavioral and emotional disorders 7–9 years—conduct disorder, adjustment, severe stress and tic disorder |
Strengths
Nationwide large sample size Limitations No information regarding measures used to diagnose RAD/DSED Only includes hospital claims and not families treated out with a hospital |
| 12. Mayes et al. (2017) | High | Case control, cross-sectional study | Three samples: 20 RAD/DSED, 933 ASD & 895 ADHD (age 4–17 years) |
Unspecified semi-structured diagnostic interview with clinician Unspecified parent/teacher questionnaires Paediatric Behaviour Scale (PBS) ASD Checklist |
5 of the 20 RAD/DSED sample had DSED only, 15 had RAD and DSED, none had RAD only | All children with RAD/DSED had callous-unemotional traits, none without RAD/DSED had these traits 73% had conduct disorder High comorbidity with other psychiatric disorders |
Strengths
Control group Multiple RAD measures Limitations RAD/DSED sample is very small |
| 13. Upadhyaya et al. (2018) | High | Routine data case-control study | N = 614 children diagnosed with RAD from Finnish Care Register Each case matched with 4 controls Mean age of diagnosis was 7.36 years old, 61% M |
None | Incidence of RAD between 1996–2012: 6.38/10,000 births, (7.38 M & 4.92F) |
Significantly increased chance of child having RAD when both parents were diagnosed with a psychiatric disorder Association with smoking during pregnancy, single motherhood and advanced paternal age |
Strengths
Large sample size Control group Limitations Limited information on RAD symptoms |
| 14. Humphreys et al. (2017) | High | Cohort Study | N = 161 children, (mean age 12.79 years) 111 follow up participants from BEIP 50 control group |
DAI | n/a | Ever institutionalized group had higher scores than control group, boys had highest levels Number of placement disruptions significantly positively correlated with inhibited behavior |
Strengths
Moderate sample size Control group Limitations Single measure of RAD DAI not validated in early adolescent sample |
| 15. Spangler et al. (2019) | High | Cross-sectional Study | N = 55 children (Mean 35.87 months (12–82) |
Rating for Instant-Stranger Engagement (RISE) DAI Stranger at the Door (StrD) Reactive Attachment Disorder Questionnaire |
n/a | Measures indicate non-normative attachment toward caregivers, inhibited impairments and presence of non-discriminate behavior DAI & RAD Questionnaire show moderate connection |
Strengths
Multiple RAD measures Limitations Small sample size |
| 16. Lehmann et al. (2016) | High | Cross-sectional Study | N = 223 children, age range between 6–12 years old Living in a current foster home in Norway |
Development and Wellbeing Assessment (DAWBA) RAD/DSED scale Strengths and Difficulties Questionnaire (SDQ) Child Protection Questionnaire |
n/a | Conduct problem factor in SDQ had higher trait correlation with RAD factor than DSED factor Significantly higher mean score for DSED compared with RAD |
Strengths
Multiple RAD measures Limitation Missing data may have decrease generalizability of the findings Lack of observational data |
| 17. Lehmann et al. (2018) | High | Cross-sectional study | N = 320 children aged between 11–17 years, 56.9% M | Reactive Attachment Disorder and Disinhibited Social Engagement Disorder Assessment (RADA) Developed from CAPA-RAD & PAPA-RAD, DSM-5 criteria |
n/a | RAD items: inability to seek comfort (mean 0.6) or accept comfort (mean 0.54) Higher age was associated scores of RAD |
Strengths
Large sample size across various countries Multiple RAD measures Limitations No observational measure |
| 18. Scheper et al (2016) | High | Cross-sectional study | N = 200 children—141 referred home reared children, 59 referred foster care children (age range 2–7.9 years old, 71% M) |
DAI Maltreatment Classification System Child Behaviour Checklist Parenting Stress Index |
Inhibited attachment behavior in home reared children was 9%, and 27% in foster child sample Combination of inhibited behaviors and maltreatment suggesting possible RAD diagnosis found in 6% (n = 9) of home reared group |
Disinhibited behaviors were present for 42% of home reared group and 51% for foster child sample 25% of home reared sample & 51% of foster child sample not exposed to maltreatment More inhibited behavior associated with internalizing and externalizing problem behavior |
Strengths
Multi-informant information i.e. use of patient records Limitations Single informant information without observation measure is insufficient for diagnosis Relatively small sample size |
| 19. Guyon-Harris et al. (2019) | High | Case control, Cross- sectional study | BEIP follow up sample age 12 (mean age 12.8 years) N = 55 children from care as usual/foster care group, 50 control) |
DAI (Early adolescent version) |
n/a | RAD/DSED strongly associated with poorer general social functioning/social competence & higher scores on “caregiver views as a victim” |
Strengths
Control group Limitations No diagnosis |
| 20. Bruce et al. (2019) | High | Cross-sectional Study Prospective longitudinal study |
N = 100 children, age range 12–62 months |
Rating of Inhibited Attachment Behaviour Scale (RInAB) DAI SDQ Wechsler Pre-school and Primary Scale of Intelligence (WPPSI) Clinical Diagnosis |
Median score reduced on RInAb & DAI and reduction in caregiver reported symptoms at 1 year follow up At baseline, diagnosed RAD = 5%, 1 year follow up—borderline RAD = 3.9% & diagnosed RAD = 2.6% |
Low overall severity of RAD Significant association between observed RAD symptoms at follow up and FSIQ Carer reported RAD symptoms were significantly associated with SDQ total difficulties score |
Strengths
Multiple RAD measures Observational measures Follow up Limitations High dropout rate Modest sample size Raters not always blinded Procedure to elicit attachment behaviors not fully standardized |
| Moderate Quality Papers | |||||||
| 21. Jonkman et al. (2014) | Moderate | Case control, Cross-sectional study | N = 126 children living in the Netherlands in kinship and non-kinship foster families from two data pools gathered for two previous studies Mean age = 60.28 (22–89) months; 50% F / 50% M n = 65 in treatment foster care, n = 61 in regular foster care |
DAI | 3% in regular foster care group had RAD and 14% in treatment foster care group |
Children with RAD symptoms had older care entry, shorter time in foster care & less time with current foster family RAD more likely than DSED to improve following improved care conditions RAD not associated with types of abuse parents/teachers report of internalizing or externalizing symptoms, number of placements; gender |
Strengths
Control group Limitations Limited measures No observational data Selection not clearly described Small numbers exhibiting RAD |
| 22. Giltaij et al. (2013) | Moderate | Cross-sectional Study | n = 102 children with borderline/mild LD referred for psychiatric consultation in the Netherlands. Mean age 8.8 (5–11) years; 29% F / 71% M |
DAI |
15.7% (n = 16) had clear symptoms of RAD; 11 showed symptoms of RAD and DSED | No associations between RAD and gender, ethnic background, IQ, age, or PDD |
Strengths
Fairly large number exhibiting RAD Limitations No control group No observational measure |
| 23. Zeanah et al. (2004) | Moderate | Cross-sectional Study | Clinicians treating toddlers in foster care in the USA, n = 94. Mean age 27.7 (10–47) months 56%F/ 44%M |
DAI “interview probes” around DSM/ICD-10 criteria |
RAD found in 35% | RAD associated with mothers’ psychiatric history Mothers’ education, teenage parent, partner violence, criminal history, depressed mood, child maltreatment, and history of substance abuse found not to be associated with RAD. No relationships between RAD and gender, ethnicity, or length of time in care were found. |
Strengths
High levels of RAD may increase statistical validity Limitations No control group No observational data Researchers aware of maltreatment history when conducting interviews Low level of variance predicted |
| 24. Elovainio et al. (2015) | Moderate | Cross-sectional Study | n = 853 internationally adopted children in Finland Mean age 8.5 (6–15) years; 54% F/ 46% M |
The attachment-related symptoms measure |
RAD occurred in 18% (n = 137) Symptoms of both RAD and DSED co-occurred in 25% (n = 214) |
RAD associated with emotional &, behavioral problems, ADHD (hyperactive symptoms, not attention problems). RAD children found to have higher internalizing, externalizing, and total CBCL problem scores |
Strengths
Large sample size Limitations No control group or follow up No observational data |
| 25. Sheaffer (2010) | Moderate |
Cross-sectional Study | n = 34 children receiving treatment in USA for RAD, in mixed care settings. Mean age 10.6 (6–19) years 44%F/ 56% M |
RPQ | n/a | RAD symptoms correlated with number of placements No associations between RAD and age, age removed from home, years in care, or years in therapy Association between RAD and attribution bias for recognition of happy in other facial expressions |
Strengths
Recruitment procedures well described Exploration of RAD in older children Limitations No control group or follow up Small sample size No observational data Missing historical information Purposeful sampling strategies and small referral base |
| 26. Lehmann et al. (2016) | Moderate | Cross-sectional Study | n = 122 foster children living in foster care in Norway Mean age 8.0 years (ranging from 6–10 years) 57% F/ 43% M |
The DAWBA RAD |
Not reported but authors note mean RAD scores were sig lower than DSED scores (p < .001) | Male gender, parental mental disorders, conduct problems, hyperactivity and DSED associated with RAD. RAD associated with functional impairment and help seeking from services. RAD did not predict contact with school psychology services, nor associated with parents substance abuse, violence exposure, number of placements, years in current foster home, age placed in current foster home, age at first placement or age |
Strengths
Reasonable sample size Limitations Size of sample reduces the power of some statistical analyses Relatively low scores on the RAD scale No observational data |
| 27. Minnis et al. (2007) | Moderate | Cross-sectional twin study |
n = 6,736 twin pairs Mean age = 7.9 years 51.3% F/ 48.7%M Report of minor differences in ethnicity and maternal educational attainment were found. |
RPQ | n/a | Factor analysis suggested RAD is distinguishable from other child psychiatric symptoms. RAD associated with harsh parenting, parental negativity, and parental positivity (negatively). Association between RAD symptoms and monozygotic pairs in both males and females and dizygotic pairs: males (r = 0.571) females (r = 0.713) For males, majority of variance in RAD due to additive genetic effects. Majority of the variance in RAD for females due to shared environmental effects |
Strengths
Large sample size Limitations Nonclinical and unrepresentative sample Response rate <50% No observational data |
| 28. Zimmerman (Unpublished thesis 2015) | Moderate | Cohort Study | n = 55 foster children in Germany. Mean age 33.4 (S.D = 18.7) months. 49% F/ 51% M |
DAI Reactive Attachment Disorder Questionnaire |
5.5% (n = 3) at T1, 1.8%(n = 1) at T2. Reduction of RAD during the first year of placement, namely in first 6 months. No significant change over time when using RAD Questionnaire. Emergency foster parents described significantly more RAD symptoms than long term foster carers (p = .006) |
RAD associated with parental mental illness RAD not associated with early adversity at T1 or T2, mental illness of parents at T1, number of placements at T1 or T2, and visitation with parents at T1 or T2 Age at placement and severity of early adverse care predicted RAD symptoms at baseline. RAD at 12m was predicted by mental health problems of biological parents and age at placement, pre-placement characteristics no longer predictive. |
Strengths
Multiple RAD measures Follow up Use of observational measures (not specific to RAD) Limitations Singular cases of RAD limits statistical analysis No observational measure At baseline foster parents might not know the children well enough for reliable rating Proportion of variance accounted for fairly low |
| 29. Mayes et al. (2017) | Moderate |
Cross-sectional Study | N = 486 children with autism and no RAD/DSED (4–17 years old, 85% M, 20 children with RAD/DSED (4–17 years old, 50% M) |
PBS Multi-informant Diagnosis of RAD/DSED |
In the 20 children, 75% met RAD and DSED criteria, none met RAD only criteria None of the 486 sample met RAD criteria |
18 of the children had previously been evaluated (17 had RAD diagnosis & 1 possible) 16 had comorbid diagnoses 13 children with RAD/DSED met criteria for autism |
Strengths
Large sample size Limitations Sample not representative of all maltreated children Unclear diagnostic procedure of RAD/DSED |
| 30. Spangler et al. (2019) | Moderate | Cross-sectional study | Georgian Sample of children raised in an institution (16 children, mean age 27.4 months) Foster children (27 children, mean age of children 63.4 months) German longitudinal sample of foster children (55 children, mean age 45.8 months) |
DAI RInAB |
RInAB and DAI scores highest in the institutional sample from Georgia and lowest in German foster sample | Significant negative correlation between RInAB total scale and externalizing behavior problems in Georgian foster sample, positive correlation with internalizing behavior in German foster sample |
Strengths
Multiple RAD measures Comparison groups used Limitations Analysis combined data from different studies and therefore data assessments are not identical Differences in sample characteristics Small sample size |
| 31. Mirza et al. (2016) | Moderate | Cross-sectional study | N = 12 Mean age 18.3 years (15–24) | Observation Schedule for RAD (OSR) RPQ CAPA-RAD Maltreatment Checklist Borderline Personality Questionnaire (BPQ) Structured Clinical Interview for the DSM-IV (SCID-II) |
10 met criteria for RAD or DSED RAD, n = 6 (Inc. 2 suspected) Both RAD and DSED, n = 3 |
9 met criteria for Emerging Borderline Personality Disorder 6 confirmed & 2 suspected ADD diagnosis All participants experienced at least one form of abuse |
Strengths
Multiple RAD measures Limitations Small sample size Substantial consent withdrawal |
| 32. Spilt et al. (2016) | Moderate | Cross-sectional study | N = 166 children (6.6–10.8 years old) | RPQ DAI |
22 (13.3%) met criterion cut off for RAD | 84.8% one or more psychiatric diagnosis 40.9% diagnosed with ASD 33.3% diagnosed with ADHD Children with inhibited RAD scored significantly lower on trust in teachers and observed emotional security with teachers |
Strengths
Multiple RAD measures Limitations No observational data Small sample size |
| 33. Bruce (2019) | Moderate | Cohort study, baseline data | N = 55 children (age 12–60 months) |
DAI RInAB |
RAD diagnosis 7.3% at baseline with 4.3% meeting borderline criteria at 1 year follow up Observed RAD symptoms decreased significantly at T2 but carer reported symptoms did not |
Children with RAD symptoms were significantly older and showed less prosocial behavior RAD associated with some mental health and cognitive difficulties Lower verbal IQ and prosocial behavior were predictive |
Strengths
Multiple RAD measures Limitations Small sample size Observational measure is not fully validated |
| 34. Eruyar (2018) | Moderate | RCT Cohort Study | 75 children screened N = 30 children (age between 8–14 years old, mean 12.45) met clinical cut off criteria for RAD |
RPQ | 40% in screened sample met cutoff score criteria | Significant number rated as above cutoff for RAD had RPQ scores in normal range PTSD and Peer related symptoms significantly decreased after intervention |
Strengths
Control group Limitations Significant non-attendance and dropout rate |