
Abstract
A range of service providers support mothers and children who are experiencing domestic violence (DV). However, research tends to focus on the role of service providers in child protection services and DV services. This potentially excludes valuable insights from a wider range of nongovernment service providers on the systemic issues that mothers experiencing DV and child separation may experience. This research explored the perspectives of 16 different nongovernment service providers about working with women who have had their children removed while experiencing DV. The study used an intersectional feminist approach that highlighted intersecting gendered and racialized power relations in service responses functioning to reinforce multiple dimensions of disadvantage. The study found that mother blame was a pervasive issue both within and outside of child protection services. Service providers described the challenges of navigating a system that revictimizes women, with particular impacts for Aboriginal and culturally diverse mothers. The findings reinforced the importance of preventing mother blame, holding perpetrators of DV more accountable, and improving collaboration across services and for more flexible responses to women living with violence.
There is an increasing recognition that domestic violence (DV) and child abuse often co-occur and should be addressed together (Broady & Gray, 2018; Westwood, 2015). Existing research in DV and child protection tends to focus on women, mothers, and the mother–child relationship (Buchanan et al., 2013, 2014, 2015; Douglas & Walsh, 2010; Klease, 2008; K. L. Nixon et al., 2013; Stanley & Humphreys, 2014; Stanley et al., 2012). There are also studies that present the perspectives of specialist service providers in child protection and/or DV services (Johnson & Sullivan, 2008; Mennicke et al., 2019; O’Leary et al., 2018; Zannettino & McLaren, 2014). Yet, what we know is that there are many different types of nonspecialist and generalist service providers who support families experiencing DV and child removal, whose perspectives are missing from the literature. In this study, we advance previous research by adding insights from service providers working within and beyond the sectors typically examined. This study used an intersectional feminist approach to investigate the perspectives of service providers from a wide range of urban and rural services in South Australia, including child-focused, women-focused, and family-focused services, about working with mothers who have had their children removed. Our main finding is that blame is pervasive within service provision and that ethnocentric and patriarchal systemic responses continue to revictimize women, unequally affecting Aboriginal and culturally diverse mothers.
Child Protection and DV: Everyone’s Responsibility
Previous research into service provider perspectives on working with mothers who experience DV has tended to focus on the responses of DV and/or child protection services. A content analysis of 13 publications from the United States, Australia, and the UK (from 1880s to 2010) has traced commonalities in how DV is constructed and responded to by child protection workers, which includes ignoring perpetrators, judging mothers, and advocating for child removal as the solution (Humphreys & Absler, 2011). Previous qualitative studies in Queensland, Australia, have included the perspectives of child protection, DV, criminal justice, and welfare and generic workers about risk, accountability, leadership, and jurisdictional issues in child protection (CP) and DV service collaboration (O’Leary et al., 2018), reinforcing the need for child protection workers to better understand the dynamic of DV (Douglas & Walsh, 2010). A common theme in social work research on child protection and/or DV relates to service collaboration barriers, highlighting different organizational mandates (Zannettino & McLaren, 2014) and how women as mothers are rendered invisible in these collaborative efforts (Davies & Krane, 2006).
What is known or researched about service provider experiences is predominantly in the context of statutory child protection and DV services. The national Australian child protection and DV policies, Protecting Children is Everyone’s Business, National Framework for Protecting Australia’s Children 2009–2020, and the National Plan to Reduce Violence against Women and their Children 2010–2022, posit that it is everyone’s responsibility to end violence against women and children and to protect children. Therefore, this research has a larger remit beyond DV and children’s services to include the experiences and perspectives of wider group of service providers who have worked with women as mothers, who have experienced both DV and child removal.
The Australian Context
The increasing concern about responding to the social, emotional, psychological, and physical risks posed to children living in DV has overwhelmed child protection systems, with few resources beyond being able to provide a crisis response (Stanley & Humphreys, 2014). DV can be broadly defined as any violent or abusive behavior, including physical, emotional, verbal, sexual, financial, or psychological abuse, that is used to control or dominate another person with whom the perpetrator has or has had a relationship (Humphreys & Absler, 2011). One in six Australian women since the age of 15 have experienced physical and/or sexual violence by a current or previous cohabiting partner (Australian Institute of Health and Welfare [AIHW], 2019b). More than two thirds (68%) of the women who had children in their care when they experienced violence from their previous partner said that their children had seen or heard the violence (AIHW, 2019b). Children may witness violence such as hearing or seeing a parent being subjected to physical, sexual, psychological abuse, and damage to property, and they may also be directly involved such as being forced to watch or participate in assaults or intervene to stop the violence occurring (Campo, 2015).
In Australia, the child protection legislative response is state-based. Definitions of child abuse are contested in the legislation. Only four states of eight mention DV and/or family violence in mandatory reporting requirements, or as psychological and emotional abuse in the harm of children, including the Northern Territory, New South Wales, Tasmania, and South Australia. However, previous research indicates that workers may not always consider the experiences of mothers in the context of legislative requirements that focus on children (Davies & Krane, 2006; Humphreys, 2008). In fact, it has been argued that mandatory reporting has the potential to inflict more harm on mothers because assisting mothers is not the main focus of either DV or child protection services (Davies & Krane, 2006).
The impacts of colonization and institutional racism is all-pervading in the lives of Aboriginal Australians and can include systematic child removal, intergenerational trauma, the destruction of traditional culture, and systemic disadvantage (Willis, 2011). In the Australian context, it is well-documented that Aboriginal Australian women experience high rates of DV and child removal (AIHW, 2019a; K. Nixon & Cripps, 2013). Of the 31,800 children in long-term care for 2 years or longer, two in five were Aboriginal Australians according to data collected as of June 30, 2018 (AIHW, 2019a). Aboriginal children are 7 times as likely as non-Indigenous children to have received child protection services (AIHW, 2019a). Aboriginal women are 2–5 times more likely to experience DV compared to non-Aboriginal women. They are also 32 times more likely to be hospitalized for family violence compared to non-Indigenous adults (AIHW, 2019b).
Research in cultural diversity and DV has emphasized that service systems are ethnocentric and westernized and that service providers do not adequately recognize or respond to cultural differences (Murray et al., 2019; K. L. Nixon & Cripps, 2013; Spangaro et al., 2019; Vaughan et al., 2016). As well, women from refugee and immigrant backgrounds experience being held responsible for men’s violence, pressured to not take action, and often face community ostracism if they do report violence, including the threat of deportation without their children (Murray et al., 2019; Vaughan et al., 2016). They report experiencing barriers in accessing income support and health services and find that systems are underresourced to deal with their specific cultural and linguistic needs and that service providers lack knowledge about dowry and other intrafamiliar relations (Vaughan et al., 2016).
This study examined the wider perspectives of service providers working in urban and rural areas, in child-focused, women-focused, and family-focused nongovernment services, including when providers are working with Aboriginal and culturally and linguistically diverse (CALD) women. As the minority and colonized groups in Australia, CALD and Aboriginal women are systemically disadvantaged and structurally marginalized. Unequal and intersecting classed, gendered, and racialized power relations pervade society and service systems. This study makes visible social and systemic inequalities affecting mothers in DV, including Aboriginal Australian mothers, who are more likely to experience DV and child removal.
Methodology
This was a qualitative, exploratory study of service providers’ experiences of working with women whose children have been removed while experiencing DV. The researchers used a social constructionist lens underpinned by the ontological position that service provider realities are culturally and historically specific (Burr, 2015). The intersectional feminist approach was combined with social constructionism. This enabled the researchers to acknowledge systemic racialized and gendered power relations as well as service provider constructions of mothers and fathers in domestically violent relationships (Locher & Prugl, 2001; Lykke, 2010). The intersectional approach was crucial to exploring unequal power relations within service systems, in service provider accounts of women as mothers, and in the client–worker relationship.
Method
The researchers used purposive and snowball sampling to identify interested research participants (Walter, 2013). Purposive sampling is an appropriate method when the researcher has a specific purpose in mind, and snowball sampling is useful to access participants who are interconnected through a web of service linkages (Neuman, 2000). Sixteen service providers were purposively sampled from nongovernmental organizations (NGOs) who responded to children, women, and/or families who had experienced child removal and DV. It must be noted that the organizations were not statutory child protection services and did not have the mandate to remove children. However, three service providers had previously worked in child protection agencies and tended to draw on their statutory experience, rather than the mission or mandate of their current employment. The employing organizations of the sample group were mostly generic, responding to families more broadly, followed by women and children’s services.
Research participants were recruited from NGOs via telephone calls and emails to the managers, who then distributed research information. Interested staff members contacted the first-named researcher directly to discuss the study or ask any questions. This research was approved by the University of South Australia Human Research Ethics Committee. A Participation Information Sheet, consent form, and an interview guide were used and distributed to potential participants prior to their decision to participate. Individual and group interviews were conducted, audio-recorded, and transcribed verbatim by the first author. Permission to record the interviews was requested upon commencement of the data collection. In the transcribing process, each participant was allocated a pseudonym.
The data were collected through two focus groups of four participants and one group interview of two rural service providers. The focus groups were held within three different nongovernment services including a drug and alcohol, a DV and homelessness, and a child and family service. As well, six individual semistructured interviews were held in private and confidential locations such as rooms on the university campus. Focus groups were requested by managers, as being more efficient for organizations, which enabled access to more participants, with varying perspectives. Focus groups and group interviews allowed for more discussion to occur within the group, while individual interviews enabled more in-depth discussions with the researcher (Neuman, 2000).
Individual and group discussions lasted between 1 and 2 hours. Both the individual interviews and focus groups were asked the same four questions, commencing with a broad question: Can you tell me about your experience of working with mothers whose children have been removed while experiencing DV? This was followed by exploring their dilemmas and challenges, their relationships with the mothers, and suggestions for future practice. The researcher provided significant flexibility for service providers to speak (Walter, 2013). There were thematic similarities using both methods. Emerging topics such as maternal protectiveness and institutionalized systemic racism were explored in further depth by using probes and asking for clarification or explanation.
Sample
As outlined in Table 1, participant’s educational qualifications ranged from nonformal qualifications to postgraduate degrees in social work and psychology. Five of the 16 participants were trained social workers. Two males and 14 females participated, which reflects the gendered nature of frontline human service work. The practitioners interviewed were highly experienced, ranging from 4 to 40 years of experience in human services. Eight of the 16 participants identified as “Australian.” Four participants were from CALD backgrounds and two from an Aboriginal and Torres Strait Islander (ATSI) background.
Sample Demographics.
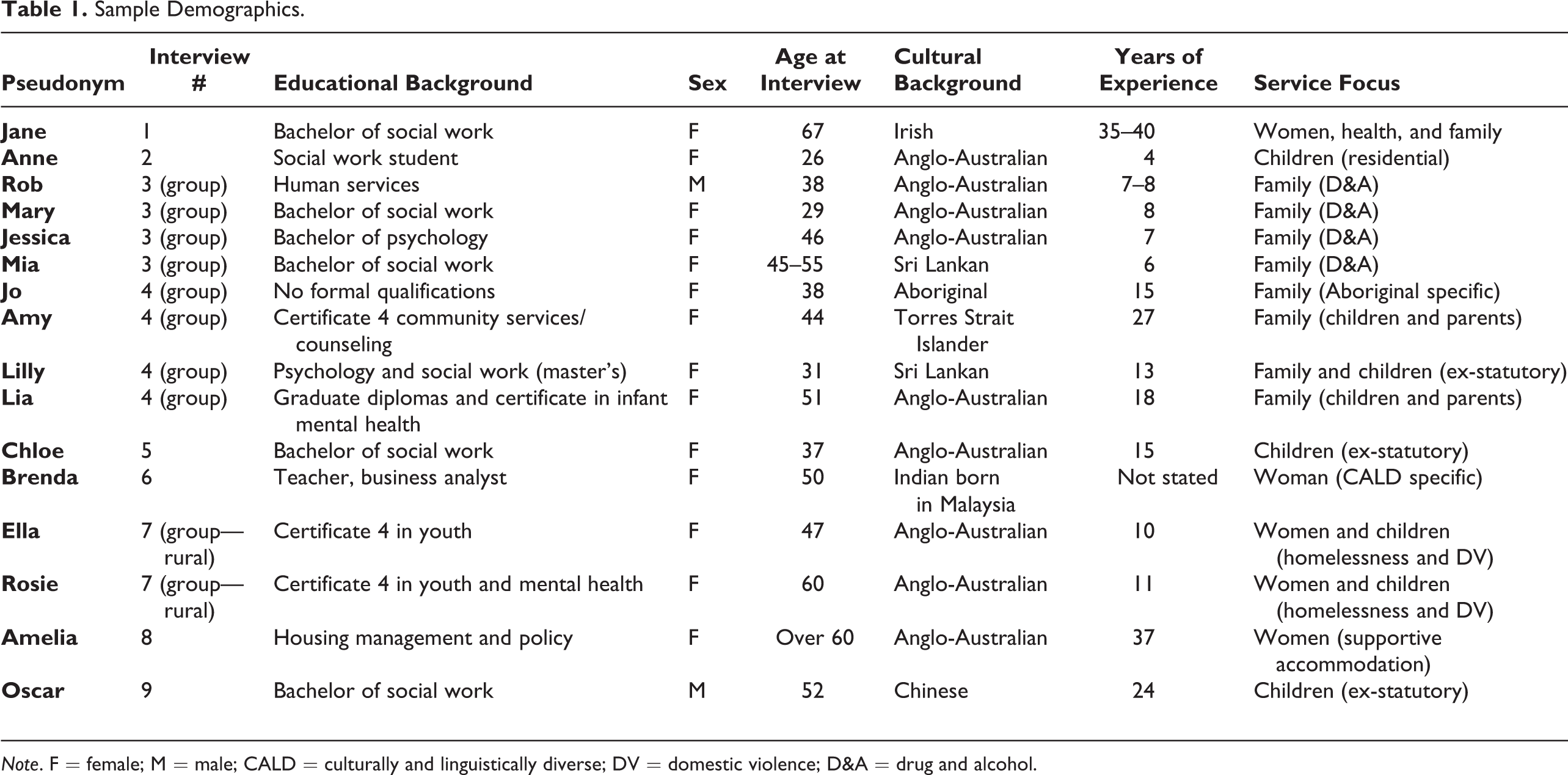
Note. F = female; M = male; CALD = culturally and linguistically diverse; DV = domestic violence; D&A = drug and alcohol.
Analysis
The researchers used thematic analysis to examine the common assumptions that informed participants’ responses. To identify themes and subthemes and the relationships between them, we coded the data using a systematic process of familiarization with the data, generating initial codes, followed by more selective and relational codes (Braun & Clarke, 2006). The two authors analyzed the data separately and then discussed the themes together, paying attention to the similarities and differences in their interpretations of the data. When the themes were discussed, the two researchers were largely in agreement about gendered themes such as mother blame and associated subthemes. One researcher particularly observed racialized differences in how women were revictimized by the system, which was also incorporated in the findings.
Findings and Discussion
Our findings showed that participants echoed similar concerns to previous feminist research with service providers about mother blame in the child protection system. The mother blame theme interrelated with constructions of bad and inadequate mothers, the lack of maternal protectiveness, self-blame, and invisible/frightening fathers. We found that mother blame is not exclusive to child protection services because blame is pervasive within service systems. In the second half of the analysis, we discuss how wider systemic complexities manifested for the NGO workers. They described the service system being “a tough system to navigate” for both mothers who were revictimized and for service providers. They advocated for all service systems to be culturally responsive to the complex circumstances affecting Aboriginal and CALD women.
Mother Blame
All of the participants discussed “blame” in some form, particularly mother blame. Two ex-statutory child-focused social workers noted that the responsibility to protect children is placed on the mother, “whether it’s right or whether it’s wrong, the mother is always viewed to have to be the protective one, isn’t she?” (Chloe). We argue that when mothers are blamed, this renders the perpetrators and their responsibility invisible.
Bad mothers
Service providers reflected on how mothers were blamed by society, by the service system, and even by their own children. The service providers recognized that women were blamed and constructed as being “bad mothers” in multiple ways: for speaking up about DV, for mothering when in DV, for failing to leave a DV situation, and because she has left. As Jane, who had worked in both women- and family-focused services said, women are positioned as a “bad wife” and “bad mother” for speaking up about violence: “You should give him another go, you know the stuff that you do is not nice, you’re not good wife, not good mother.” Yet, when women are mothering in DV and trying to “create a family,” that too is judged as unacceptable. As Mia, from a family-centered agency said, “they’re trying to create family but…its obviously being judged as not acceptable. That’s tough.” As well, after the child has been removed, mothers are positioned as “not caring” and failing “to protect” her children (Jane). The idea that parents are inadequate was perceived to be in the culture of child-focused services: “There’s this big culture…the parents are inadequate…there is so much more to it than that…it’s not her fault” (Anne). Furthermore, participants reported that mothers are blamed by their own children for not leaving the relationship or for leaving them in care. As Jane said, “I’ve certainly worked with children who have grown up thinking: mum just couldn’t be bothered, she never bothered, bloody abandoned us.” Jane’s observation resonates with findings in research from the perspectives of adult children who grew up in DV, that they experienced feelings of betrayal and an unresolved relationship with their mother (Buchanan et al., 2015; Lapierre, 2008, 2009, 2010; Moulding et al., 2015; Wendt et al., 2015).
Paradoxically, a few service providers also blamed mothers themselves in the interviews. We argue that mother blame is organizationally embedded, pointing to the “structural and cultural change required by organisations to support workers to shift their practice” (Humphreys et al., 2020, p. 195). The few service providers who indirectly blamed the women reflected on the age and naivety of the young mothers and the powerful statutory role of child protection workers. Two older service providers from a rural homelessness and DV service said: …saying about the domestic violence, these young girls, within a week, two weeks, with children, they’ve got a stranger living in their house. That’s an issue that I have…bringing him into your house with your children! (Rosie) …these mothers, is not easy to work with them because there’s a lot of blame in our involvement with them…we still try to ensure that we do this in the best interest of their children…. they basically try to avoid facing the reality that the issue that they have…blaming is a big thing…they blame you…just what you’re gonna get with a statutory agency…there’s a huge power imbalance. (Oscar)
Maternal protectiveness
Our findings demonstrated the power dynamics between clients and service providers associated with “educating” mothers to “protect” their children. These power dynamics render invisible the maternal protectiveness strategies that mothers living with DV often use (Buchanan et al., 2013, 2015; Haight et al., 2007; Lapierre, 2009, 2010; Peled & Gil, 2011; Wendt et al., 2015). For example, two ex-statutory child-focused service providers discussed women’s lack of ability to protect their children in DV and highlighted ineffective tactics women adopted to protect their children. Oscar, for instance, noted that women’s protectiveness did not always contribute to enhancing children’s safety: Sometimes, because with domestic violence…they actually so much under control of the perpetrator, so it is really become very powerless for them to be able to protect their children…being in that position herself [in DV] means that quite often she’s not able to…be protective of the child. There are little things that lots of women do to protect their children, but ultimately at the end of the day, unless you leave that situation, it doesn’t matter what you do, it’s going to be to the detriment of that child. Women often felt their action to protect was never understood, named, acknowledged…the many ways in which they were to protect their children…how they were navigating danger was never taken into account…their attachment to their children and with their children is often treated as barely existent in the face of the label ‘failure to protect’ [by statutory child protection agencies]. (Jane) …and what about protection skills, you know, learning protection for their children, the protective skills that is needed for the kids to grow…they need to know how to protect themselves and all that self-esteem…but they also need to learn how to protect their children…not just themselves, their children.
Service providers in this study were aware of maternal protectiveness and some strategies that mothers use to protect their children from the effects of DV. For example, Amy made visible some of the mother’s protective strategies, which included allowing the children to go to the shops late at night or constantly breastfeeding. She recounts her conversations with mothers: [The mother says] “so, I tell the kids to go to the shops at 8 o’clock at night, cause they are a lot safer there than they are at home at the moment”…. [As well] Mum’s breastfeeding too much, the babies on the breast a lot. [The mother says] “cause he’s not gonna hit me with a baby on the boob” [breast].
Mother’s self-blaming
Mother blame is often internalized as self-blame because of the women’s feelings of shame and guilt for “failing to protect” their children (Lapierre, 2009, 2010; Moulding et al., 2015). As Jessica said, “they carry that guilt and burden around with them.” The service providers from the drug and alcohol family-centered service focus group particularly highlighted the mother’s sense of self-blame when their children were removed in the context of experiencing both DV and drug or alcohol abuse: They [mothers] feel like a failure, that they haven’t managed to build that happy family or keep a good marriage or whatever that is. It’s impossible…they give themselves the impossible, but they still feel bad about it, they blame themselves. (Mia) They do a lot of self-blame and then blame on exes or whatever, if he hadn’t have done that…or he’s a wonderful father, he never hurts them, he just keeps hurting me. The stories that they keep telling them self to make it, I don’t know…. (Jessica)
Brenda, a service provider from a woman-centered service perceived women whose children were removed as being “broken.” She said, “they feel they are so small, insignificant, they have lost their place, because they have lost that role that they had…depressed, sad.” Jane also noticed that a woman she worked with denied having children because of feelings of shame, “…and somebody goes…have you got children? “Nuh I don’t have children,” there’s too much shame attached, cause how do you explain that one?” This denial about having children highlights how the stigma and shame associated with DV and child removal impact on women’s sense of being nonexistent, failed mothers.
Participants also discussed the aftermath of mothers being separated from their child/ren. As Jessica observed, when women do leave a DV relationship and children are removed, the mother is then further isolated from system supports: “Nobody around, nobody. Completely isolated.” Jessica’s observations are consistent with literature on post removal issues. Postremoval is characterized by increased stigma, social isolation, low self-esteem, feelings of powerlessness, limited access to resources, and feelings of shame and guilt (Schofield et al., 2011). Importantly, postremoval issues exacerbate the circumstances that lead to the removal in the first place, including substance abuse. As Brenda, who worked in a women’s service said: They’re women who have also had drug problems themselves, who’ve had their kid removed…what makes it really hard for them, is that separation and that isolation, makes it even harder to get back clean…. Their sense of self is degraded.
Amy also vividly articulated the personal effects of DV on women’s sense of self, which was exacerbated by the punitive responses of the service system: It’s a feeling of low self-worth…you got yourself into this situation, it’s shaming, it’s embarrassing, it takes away your dignity, it takes away your choice…there’s all this power and control and it’s almost like the system comes and puts the same power and control back onto them [the women].
Overall, the majority of service providers discussed the effects of violence, including self-blame, and, in doing so, demonstrated their understanding of power and control within a violent relationship and what leaving a relationship entails. At the same time, however, a minority of service providers from both voluntary and statutory organizations continued to blame women to some extent for not addressing their personal issues and their naivety about relationships. These findings about the pervasiveness of blame extend beyond previous studies focusing primarily on mother blame in child protection services.
Next, we consider how service providers understood responses to perpetrators of violence. We found that all service providers deemed that it was pertinent to hold perpetrators more accountable for their violence. This included shifting the responsibility away from the mother back onto the male perpetrator responsible for the violence, especially in the responses of statutory child protection services and court systems.
The hidden power of perpetrators: Invisible and “scary” fathers
Child protection services tend to focus on the mother’s responsibility to protect children, rendering the perpetrators invisible (Bourassa et al., 2008; Broadhurst & Mason, 2013; Douglas & Walsh, 2010; Humphreys & Absler, 2011; Klease, 2008; Lapierre, 2010). The “invisible man syndrome” (Burke, 1999) imbues child protection responses. This was also recounted by participants in this study. As Jane explained: …the child protection service protects from the abuser in domestic violence…daddy’s the abuser…the child protection service does not work with dads to reduce their violence…to acknowledge the violence, the story that emerges is mum didn’t do anything to help.
Mothers are living with the effects of DV and may experience other issues including mental health and drug and alcohol abuse. However, when the blame and responsibility to protect children are placed on them, service systems unwittingly favor the rights of the perpetrator (McInnes, 2014). For example, family-centered service providers like Amy provided accounts of children being removed from the mother by the court system and placed with the perpetrator: …we find that a hell of a lot, that actually they are removed because of the DV, then the mum starts becoming unstable because she’s becoming unhinged, and then they’re looking for somewhere to place the kids, and because the father is now settled and got a house and everything’s looking really well…often in the family court…. He’ll get custody of the children. …they are saying “we know he is dangerous; we know he does drugs,” and the court is saying “for his mental health, the child should also stay with him every fortnight”…while she is still being punished.
Service providers, from DV, drug and alcohol, and health and reunification services, all spoke of the lack of accountability that is placed on the perpetrator within the violent relationship. They expressed their frustration at the system’s response in further punishing mothers and children as expressed by Jane and Jessica: Nobody’s talking to him. Nobody’s talking to the person who’s the perpetrator of the violence against these children…. The perpetrator is not addressed. The violence with the person who’s perpetrating the violence is not considered problematic. (Jane) The mother is considered problematic…Why isn’t he being removed, not the children, do you know what I mean, like why aren’t we removing him? (Jessica) People don’t want to home visit if they know there’s violence in the house, people don’t want to offer flexible options…. people are very fearful of talking about it [DV] in case they have to do something about it…. In case that mum actually turns around and says “actually yeah, can I leave, or what are my options, or how can I do that?”
The contradiction was highlighted between the focus on risk and safety for child protection workers and the expectation on mothers to “control” their violent partners, despite increased risks of post separation violence. For example, Jane, who was working outside the child protection system, observed: The child protection [workers] were like: “we’re not going out there, it’s too dangerous, much to dangerous, because he’s quite violent.” And I’m going “and you want her to manage him, to stop the violence?…you won’t even go near there. She’s living in it. And you want her to somehow control his violence?” Because when she leaves, it doesn’t change…the violence was continuing…[alluding to post separation violence]. …going into that house, he was scary…so even if there was a big issue, I was never going to take him on, on my own, in his house…so if I felt like that, what did she feel like?
Service Systems: “It’s a Tough System to Navigate”
The service providers in our study also discussed how service systems were “tough to navigate” for both mothers and workers, including legal, court, housing, child protection, and support systems. They were tough to navigate because of being crisis driven, the government and nongovernment service interface, and the competing values between women- and child-focused agencies. As one worker stated: “Yeah, it’s a tough system to navigate…it’s not a great system its tough!” (Anne). As another group of workers said: “It’s hard, it’s hard for us workers to navigate. As case coordinators, to coordinate some of those services, it’s hard for us” (Amy, family-centered agency). They discussed how the system was a “blunt hammer” and crisis driven: It’s a blunt response isn’t it? by virtue of it being crisis driven, the system forces us to, all of us, clients and workers alike, what it forces us to do is create a crisis and respond to it with a blunt hammer [referring to mandatory notifications in particular]…although we are good with dealing with the crisis, we are not good with dealing with the preventatives. (Lilly) It’s about the law, its legislation, its what’s written in black and white and we know when we work in this space, it’s not black and white. It’s complex…that’s where the dilemma comes from…that is some of the challenges…sitting behind the legislation…it is powerful. She’s lost her housing…lost her support system because most of them were family or child oriented…she’s now living with her mum in the spare room. No baby, no children, no hope…has been very difficult to work with in a positive sense…. It’s like she’s doing all these things she needs to and there’s still brick walls. (Jessica) The conversations are very one sided…. We don’t get a lot of information, but we are expected to give a certain amount of information…it makes it very hard for us because we don’t always have a complete picture…why they are making decisions. The woman needs to have someone, that’s what I’m saying, like there needs to be strong services advocating for that woman. 100%. But it’s never going to align with the child protection role, it’s just not!
Women being revictimized by the system
Service providers also highlighted that the system revictimized the women in multiple ways. Women were revictimized when service providers lacked information about the effects of DV, feared perpetrators and blamed women, withdrew service supports once children were removed, did not recognize the trauma of child removal, and ignored the cultural contexts of women’s lives.
Participants such as Amelia and Amy argued that power inequalities in DV are replicated by service systems. As Amy said, “you leave an abusive situation with a partner and then you get abused again by a system…that’s almost perpetrating abuse, cause the power balance.” Amelia further explained: People…don’t necessarily understand the power imbalances between the perpetrator and the victim…they don’t understand that the whole issue of power and control…. The trauma of having children removed is not recognized…the trauma for the children is not recognized ether…. I’m just really conscious that the system revictimizes all the time…the trauma is just exacerbated by the system.
Participants in this study explained that service systems continue to revictimize, punish, and blame women affected by DV by not adequately supporting them but still holding them responsible to protect their children. For example, Amelia, a service provider from a women’s supportive accommodation agency, expressed her frustration about systemic issues affecting Aboriginal women living with DV, which she called systemic “victimization.” For example, she pointed to the repeated child removals that do not recognize maternal protectiveness and the steps Aboriginal women have taken to rebuild their lives: …they are victimized by the system and they have their children removed almost by rote…they have experienced such bad, bad work…. She’s not given even an opportunity to try…it’s not recognised that she may have turned her life around.
A culturally responsive system
To approach the unique challenges facing Aboriginal women living with domestic and family violence, it is important to center the perspectives and community knowledge of Aboriginal and Torres Strait Islander (ATSI) service providers about what are considered culturally appropriate responses. Amy, a Torres Strait Islander worker, spoke about more responsive interactions with the perpetrators of violence. In stark contrast to more fearful responses discussed earlier, she described using “growling” with perpetrators, community networks and elders, “aunties” and “uncles,” and not focusing on “qualifications”: …having the right people in there…I growled him, I’m like “what’s she doing with that black eye and what are you doing -not good enough!”…he took the growl…that gives that kind of space to open those conversations…to do that you’ve gotta have the right people…not always the people with the qualifications…their aunties, and there is some uncles, out in the community that we need to tap into a little bit more resources. They’ve got family credit…. And this is where we go wrong in the work we do; we look for a western qualification and it’s not always about the western qualification.
Amy’s response can be contrasted with the experience of a new social work graduate who was a young, white Australian worker. She reflected on her experience entering a rural Aboriginal community to address the protection of children in DV. She cited the cultural unsuitability of this: It was like sending a lamb to slaughter…I look back now, and I think, I just did what I was told!…do you know what I mean? I think, God that never should have happened (Chloe).
While women of diverse cultural backgrounds have reported positive experiences with women’s service providers, they have found it difficult accessing these services, especially if they do not want to leave their violent relationship (Murray et al., 2019; Vaughan et al., 2016). The unrealistic expectation that women leave the relationship was discussed by Lilly, a service provider from a Sri Lankan background, when working with CALD and refugee women: There are a lot of pressures on culturally and linguistically diverse women to remain in that relationship because of the very real social and cultural pressures…[they] get demonized and ostracized in the community. …we need a bit more sophistication in our DV services that allow for families to work together on responding to the violence, if they want to stay together…you’re kind of given an ultimatum, you have to choose between the life you know…now your kids being removed. (Lilly)
Participants also emphasized racism and how new arrival and refugee communities are often in the “spotlight” and homogenized, making it harder for women to speak up. This is explained by Brenda, who was from an Indian Malaysian cultural background and worked in a women’s service: …as soon as something happens in an ethnic community, it gets blown up. “Oh, you know the Sudanese boys are doing this or the Pakistani’s are this or the Indians are this or the Chinese are this.” So, I think that makes it really hard for the people in the community to come out and say, “yes there is violence in our community,” because they will be in the spotlight if they did that.
Implications for Feminist Social Work
Feminist social work research and practice is informed by many different feminisms but fundamentally intends to highlight gender and power inequalities and to empower people most disadvantaged in society (Hyde, 2013). In the context of DV, women and their children are the most disadvantaged. This study used an intersectional feminist approach to interrogate how gender and race intersect to create multiple dimensions of systemic disadvantage (Crenshaw, 1991), including for Aboriginal Australian and CALD women affected by DV and child removal. The study found that a range of systemic and institutionalized practices continue to stigmatize and blame mothers whose children have been removed in DV. In the absence of effective interventions, perpetrators are both invisible and feared by service providers.
While the responses of feminist-informed DV services potentially differ to child-focused or family-focused organizations, this study found that mother blame pervades social discourse and service systems. This study shows that social workers must continue to make visible and reshape systemic practices and policy responses that further victimize and blame mothers for “failing to protect” their children when living in DV. It also emphasizes the importance of holding perpetrators accountable for their violence, including by further engaging with them. This study is supported by social work ethics and values that intend to challenge institutionalized sexism and racism and uphold social justice and human rights, for diverse groups of women and children living with the effects of gendered violence and child removal (AASW, 2010; International Federation of Social Workers, 2018).
The service providers in this study advocated for educative and preventative responses and more flexible options within the service delivery system. They supported women’s choices and made visible their maternal protectiveness in DV. All participants, except for the two rural service providers, spoke of the lack of collaboration between statutory government services and nongovernment agencies. Consistent with previous literature about improving collaborations across the service interface of DV and child protection (Laing et al., 2018; Mennicke et al., 2019; O’Leary et al., 2018), the participants suggested that women-focused and child-focused services have competing interests because one service is voluntary and the other is statutory. They highlighted that legislative requirements and crisis responses made it difficult for social workers to work in the best interests of women and their children, often distributing power back into the hands of the male perpetrator of violence.
However, social work models have emerged such as David Mandel’s Safe & Together Model that assists organizations and practitioners to offer comprehensive multidisciplinary, multiagency collaboration across the service system. This model recognizes that children are safe when together with the nonoffending parent, usually the mother, ensures service providers are working in partnership with mothers, and checks that perpetrators are being engaged with and held accountable (Safe & Together Institute, 2018).
Study Limitations
The findings of this study cannot be generalized beyond the experiences and perspectives of the 16 service providers interviewed, of whom five were trained social workers. The participants were recruited from diverse service sectors. However, there were commonalities in how they perceived that mothers who had their children removed were blamed and systems were failing them. Two social work participants who had previously worked within a government statutory child-centered agency (Oscar and Chloe) presented some differing perspectives to those who had not worked in this area. Future research with statutory service providers can expand the analysis of system complexities within the statutory role. As well, two participants were from a rural location. In future studies, it may be beneficial to gather the perspectives of service providers from a wider range of rural locations and services. Other potential avenues for further research include (1) making visible the voices of those directly impacted by service system gaps and failures and (2) interviewing more service providers from Aboriginal and culturally diverse backgrounds to further explore culturally sensitive practice and service system responses.
Conclusion
The findings of this study resonate with feminist social work literature that has a long history of interrogating how service systems condemn women and blame mothers when they are positioned outside Western middle-class ideals (Abramovitz, 1997/2013; see also Zufferey & Buchanan, 2020). Mothers who have survived DV and children removal continue to be socially constructed as being deficit, blameworthy, and failed mothers, while perpetrators continue to be invisible or emboldened by a system that is complicit with their violence. This study found that a mother’s ability to rebuild her life and reunify with her child/ren is challenged because of mother blame, combined with failures to acknowledge maternal protectiveness and women’s revictimization by the system. A more responsive service system would prevent disciplining women as mothers, by acknowledging the disempowering intersecting effects of gender and race inequalities and institutionalized sexism and racism, on mothers affected by DV (Zufferey & Buchanan, 2020). As social workers, we are working with cultural differences not within our own realm of experience, which requires us to facilitate collaborative dialogues and practice self-reflexivity, consistent with an intersectional feminist social work approach (Murphy et al., 2009). Service providers can join with mothers to challenge unfair systemic practices that disadvantage them, whether they are living in a violent relationship, surviving the aftermath of the violence, or when their children have been removed.
Multidimensional systemic inequalities are reinforced by unequal power relations within service systems. The service providers in this study acknowledged the power imbalances between victim and perpetrator as well as between service providers and mothers, particularly for statutory child protection workers, who hold a great deal of legislative power over women and their children. They advocated for this power to be used responsibly from a supportive value base, that is, nonjudgmental and culturally competent. This study has included a wide array of service provider perspectives beyond statutory child protection and DV services. We argue that intersecting gendered, racialized, and classed power relations in service systems perpetuate mother blame and reinforce male violence, which is a concern for all service providers.
Footnotes
Acknowledgments
We would like to thank all the services and service providers that agreed to participate in this study. As well, we would like to thank the Zonta Club of Adelaide for providing funding for this project and The Ian Cox Memorial Social Work Honours Scholarship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We would like to thank the Zonta Club of Adelaide for providing funding for this project and The Ian Cox Memorial Social Work Honours Scholarship.