
Abstract
Foster care offers children a safe family environment and is effective in buffering the negative effects of early adversity. Specifically, foster care has been found to facilitate secure attachment to foster parents. However, there are limited data on attachment development in children entering foster care after the first year of life. In this study, we examined attachment behaviour and representations as well as symptoms of reactive attachment disorder (RAD) and disinhibited social engagement disorder (DSED) in 3–6 year-old foster children. We studied two subgroups of foster children with different preplacement experiences (Group 1: children entering foster care after living in institutions; Group 2: children entering foster care after living with their biological families) and compared them with a community sample. The results revealed that children in both foster care groups showed significantly lower attachment security at the behavioural level, higher hyperactivation and disorganization at the representational level, and significantly more symptoms of RAD and DSED than the children in the control group. Analyses did not indicate significant differences between the foster care groups. Moreover, no significant associations were found between attachment-related variables and preplacement experiences. This may be an indication that in long-term foster care, the quality of foster care becomes the major factor affecting a child’s attachment development. Thus, foster parents need supportive services and interventions with a focus on attachment development.
Keywords
Introduction
The consequences of early adversity for child development
Adverse rearing environments, whether abuse and/or neglect in biological families or deprivation of care in institutions, put children at risk for developing a variety of social, psychological, and behavioural problems (Berens & Nelson, 2015; Bick et al., 2018; Pears & Fisher, 2005; Tarullo et al., 2011; Vasileva & Petermann, 2018) and can lead to lifelong difficulties (Norman et al., 2012).
In particular, inadequate care in early life can be detrimental to the formation of attachment relationships (Dobrova-Krol et al., 2010; Dozier et al., 2012). In a meta-analysis, Cyr et al. (2010) found elevated rates of both disorganized and insecure attachment in children with history of maltreatment in their biological families compared to normative low-risk samples. Moreover, maltreated children were less securely attached and showed more disorganized attachment than other children at risk (e.g., children living with a single parent or a parent with substance abuse).
Orphanage care (typically the condition with the most extreme privation, often described as structural neglect) is particularly detrimental to attachment development. Caregivers in institutions typically have to care for numerous children, and thus, dyadic interactions are rare. Turnover rates among caregivers tend to be high, and many children in institutions change groups (and caregivers) regularly. For example, The St. Petersburg - USA Orphanage Research Team (2008) reported that in Russian orphanages, children had contact with up to 100 caregivers before they turned 2 years of age. Lionetti et al. (2015) investigated attachment in institutionalized children and found that only 18% of institutionalized children were securely attached to their primary caregivers, and 54% of the children showed disorganized attachment. Similarly, a study from Ukraine showed high rates of attachment disorganization in children living in institutions as well as poorly developed attachment patterns in nearly three-quarter of the sample (Dobrova-Krol et al., 2010). However, there is also evidence that not all children may be equally vulnerable to extremely adverse rearing experiences (Bakermans-Kranenburg et al., 2012).
In addition to insecure or disorganized attachment, which represent normal variability in attachment, two psychiatric disorders [reactive attachment disorder (RAD) and disinhibited social engagement disorder (DSED)] have been described in association with experiences of neglect, abuse, and deprivation (Zeanah & Gleason, 2015). DSED and RAD are considered psychiatric disorders and show weak to moderate associations with attachment insecurity and disorganization (Gleason et al., 2011; Zeanah et al., 2005; Zephyr, Cyr, Monette, Archambault, et al., 2021). Despite having a common aetiology, the diagnostic features and developmental courses of the two disorders differ. Symptoms of RAD include inhibited, emotionally withdrawn behaviour and social and emotional disturbance and symptoms seem to decrease significantly when the conditions of care improve (Nelson et al., 2020; Smyke et al., 2012). In contrast, symptoms of DSED involve socially disinhibited behaviour towards unfamiliar adults that tends to persist even when the child is moved to a family home with sensitive and stable caregivers (Gleason et al., 2014; Guyon-Harris et al., 2018; Humphreys et al., 2017; Lawler et al., 2016; Román et al., 2022; Rutter et al., 2007).
The prevalence of clinically relevant RAD and DSED symptoms in children exposed to pathogenic care is heterogeneous, with rates ranging between 1.9 and 27% for RAD and between 4 and 51% for DSED, with a tendency towards higher rates in institutionalized children (M. Bruce et al., 2019; Gleason et al., 2011; Jonkman et al., 2014; Scheper et al., 2016; Zimmermann, 2015).
Foster care as an intervention
Foster care is an alternative form of care for children who lack the care of their birth parents
Recent research investigating symptoms of RAD and DSED in children moved to foster care after being exposed to early adversity has revealed two trajectories. Children with DSED symptoms continued to display such behaviours even after they were placed in foster care (Gleason et al., 2014; Guyon-Harris et al., 2018; Humphreys et al., 2017), whereas symptoms of RAD tended to decrease significantly after moving to a sensitive foster home (Smyke et al., 2012), although such symptoms may persist in a small group of children (Nelson et al., 2020).
Recent research had addressed many important aspects of attachment development after pathogenic care, although several questions remain unanswered. First, as recent studies mostly addressed children placed in foster care during their first year of life, knowledge about the development of attachment as well as RAD and DSED in children who move to foster homes after their first year of life is limited. The lack of research on such children is particularly worrisome, as these children may have more difficulties trusting caregivers and may thereby show specific patterns of deficits in attachment security and organization, as indicated by Carrera et al. (2021) and Garcia Quiroga et al. (2017). Both studies found significantly higher rates of attachment disorganization as well as lower attachment security in foster children compared to control groups (see also Garcia Quiroga & Hamilton-Giachritsis, 2016 for a review with similar conclusions). Similarly, the Bucharest Early Intervention Project (BEIP) found that children moved from institutions to foster care after the age of 24 months showed more signs of DSED than children moved before the age of 24 months (Smyke et al., 2012). However, the BEIP sample included only postinstitutionalized children, so that it remains unclear whether this result can be replicated in samples of foster children without experiences of institutionalization.
Second, although all aversive experiences are negative in nature, different types such as physical or emotional abuse, deprivation, or neglect may have different effects on a developing child and may correspondingly facilitate or hinder the development of secure and organized attachment bonds after moving to foster care. In most cases, it is impossible to disentangle those experiences, as they often coocure (e.g., Stronach et al., 2011). Nevertheless, a small number of studies (Fresno et al., 2018; Han, 2020; Stronach et al., 2011) has looked closer at differential effects of early adversity, i.e. whether particular types of abuse and neglect are related to specific patterns of attachment. Fresno et al. (2018) reported that abuse in general was related to higher incidence rates of both insecure and disorganized attachment representations. However, no specific patterns of associations between particular types of abuse and the quality of attachment narratives were found. Similarly, Stronach et al. (2011) investigated attachment behaviour and representations of preschool aged children and did not detect any differences in attachment related to subtype, chronicity, severity, or frequency of maltreatment. Contrary to these findings, a Korean study by Han (2020) found that children who experienced complex trauma, i.e. children who were exposed to more than one type of abuse or neglect, exhibited higher rates of insecure attachment than children who were exposed to only a single type of emotional abuse or neglect. Moreover, the more chronic and severe the abuse and neglect were, the more adversely they affected children’s attachment representations.
While there have been several studies exploring child development in foster care, to our knowledge, none have investigated attachment security and disorganization as well as symptoms of RAD and DSED by comparing foster children from different preplacement settings.
Therefore, in the current study, we intended to extend existing knowledge on the effects of preplacement experiences on both the formation of secure and organized attachment relationships and disorders of attachment and sociability. The impetus for the study was child welfare reform in Georgia, a country that was forcibly annexed by the Soviet Union in the 1920s until its secession from the Soviet Union in 1991
The goal of our study was to assess attachment behaviour and representations as well as symptoms of RAD and DSED in preschool-aged foster children. More specifically, the three objectives of our study were as follows: (i) to compare attachment behaviour, attachment representations, RAD, and DSED symptoms in foster children with and without experience of institutional care with a community sample. We expected children with experiences of institutional care to be most affected, i.e., to show lower attachment security, higher hyperactivation, greater disorganization, and more RAD and DSED symptoms. Second, we aimed (ii) to explore the relationships among attachment behaviour, attachment representations, and symptoms of RAD and DSED in these subsamples. Furthermore, we aimed (iii) to analyse the effects of different preplacement characteristics (number of placements, duration of institutionalization, age at placement in foster care, age at placement in current care) on attachment variables.
Methods
Participants
Preplacement Characteristics of Foster Children.
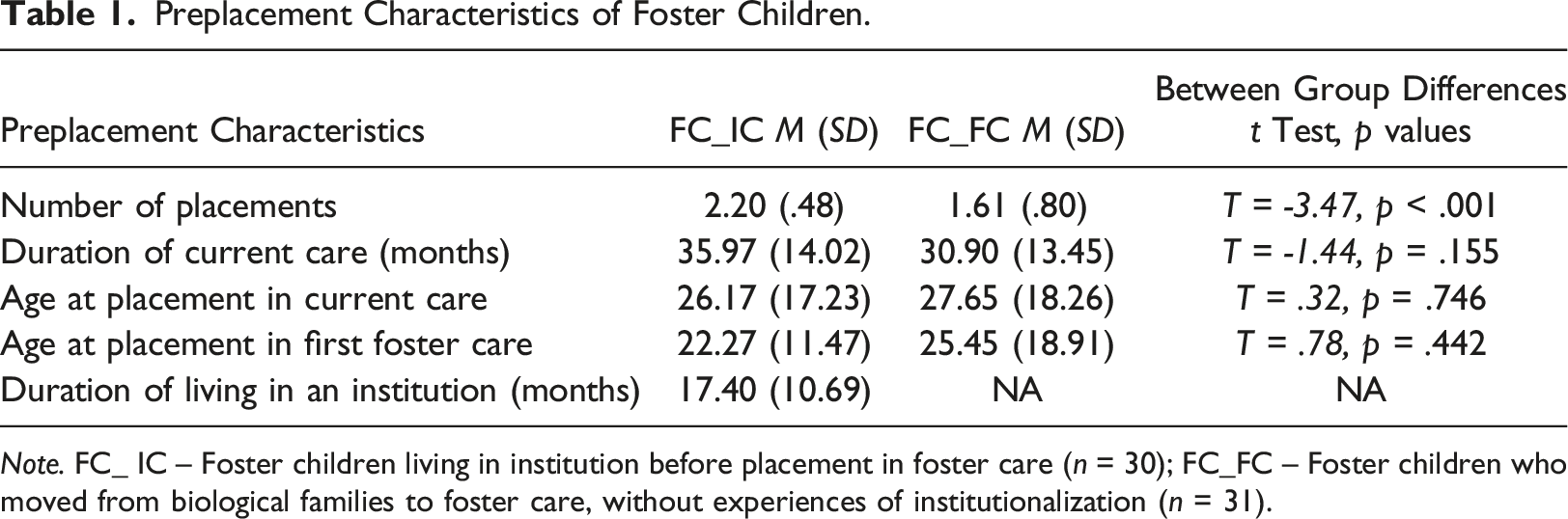
Note. FC_ IC – Foster children living in institution before placement in foster care (n = 30); FC_FC – Foster children who moved from biological families to foster care, without experiences of institutionalization (n = 31).
The comparison group consisted of children living with their biological families who had never been institutionalized or lived in foster care. The majority of foster families lived in either disadvantaged neighbourhoods of the capital city or rural areas. To ensure that the comparison group did not differ significantly from the foster care groups in terms of socioeconomic status, all participants were recruited from public day-care centres located in the same suburbs where the foster families were living.
The study sample consisted of children aged between 3 and 6 years. To ensure that the foster children had sufficient opportunity to develop attachment to their current caregiver, we included only foster children who had previously spent at least 6 months in current care. Exclusion criteria for the foster groups were kinship care and the diagnosis of mental or physical disabilities. For the comparison group, exclusion criteria were a history of out-of-home care, the experience of maltreatment and/or neglect and the presence of mental or physical disabilities. The parents were asked whether children had experienced any kind of abuse or trauma or whether social services had been previously involved. One child from the comparison group was excluded from the analysis due to experiences of emotional and physical abuse.
Procedures
All data were collected from September 2015 to August 2016 in Georgia. The study was conducted in accordance with the WMA’s Declaration of Helsinki. Ethical approval of the study protocol was obtained from the Ministry of Labor, Health and Social Affairs, Georgia (#04/27773). First, information about the study was disseminated by social workers among foster families. The families who were interested in taking part in the study informed the social workers and gave consent to be contacted by the research team. Consent to take part in the study on behalf of the foster children was given by the social worker from the Social Service Agency who represented the legal guardian of the child. Furthermore, foster parents also provided written informed consent. To recruit children for the comparison group, information regarding the study was disseminated at 20 day-care centres, and interested families contacted the researchers. All parents provided written informed consent to participate. Participating (foster) families were asked to determine the child’s main caregiver who was asked to take part the study. In all cases, the (foster) mother was designated as the main caregiver.
Data were collected during two home visits conducted by two researchers. During the first home visit of approximately 3 hours, the (foster) mother filled out several questionnaires, and a developmental screening procedure was administered to the child. The (foster) mother was asked to play with their child in two different situations. At first, in a 25-minute free-play situation, the (foster) mother was asked to play with the child with a box containing age-appropriate toys (e.g., balls, cars, dolls, cubes). Next, a 20-minute semistructured mother-child play assessment adapted from the “three boxes” task of the NICHD protocol (NICHD Early Child Care Research Network, 2003) was conducted. The assessment consisted of three different age-appropriate tasks for the child (puzzle, drawing kit, construction toy), and the (foster) mother and child were instructed to perform the tasks for the next 20 minutes. Alongside predefined play situations, the home visit also included observations of the daily activities of the (foster) mother and the child without instructions from observers. Directly after the first home visit, the Attachment Q-Sort was sorted by a trained observer.
During the second home visit (1 hour), the Attachment Story Stem Completion task was conducted with the child, while a second researcher administered the Disturbances of Attachment Interview with the (foster) mother. Additionally, both home visits were videotaped for later analyses, and the interview with the (foster) mother was audio-recorded.
Measures
Attachment Q-Sort (AQS)
Attachment security at the behavioural level was measured with the Attachment Q-Sort (Waters & Deane, 1985), which has been used and validated in a large number of studies (Posada et al., 2013, 2016). A recent meta-analysis including 245 studies showed that the AQS is a valid measure of attachment security (Cadman et al., 2018). The instrument consists of 90 items describing the child’s attachment and exploratory behaviour. After completing the observation during the home visit, items were sorted according to a predefined rectangular distribution into nine piles from not characteristic to very characteristic for the observed child. The resulting Q-sort profile of each child was correlated with an expert criteria sort of a prototypically secure child (Waters & Deane, 1985), yielding a security score between −1.0 (very insecure) and +1.0 (very secure). In the present study, the observer received training before conducting the home visits. The training included performing ratings of 30 cases (from both live and video observations). After the training, interrater reliability was calculated based on 19 cases. The intraclass correlation between the study observer and a second experienced observer was .89. Coding was conducted directly after the first home visit; hence, the observer was aware of the child’s group membership but was blind to other characteristics of the child.
Attachment Story Completion Task (ASCT)
Attachment representations were assessed using the attachment story completion task (Bretherton et al., 1990), which consists of six story stems, each designed to activate a child’s attachment representations and feelings. The interviewer presented each story beginning with a set of small human figures, initially introduced as a family (mother, father, two children) and a babysitter. Afterwards, the child was asked to show and tell what happens next. The coding of the stories was conducted with a translated version of the Q-sort procedure developed by Miljkovitch et al. (2004). After reviewing each tape, a trained coder sorted the 65 Q-sort items according to a normal distribution into seven piles from least characteristic to most characteristic for the child. The resulting Q-sort profile was correlated with criterion sorts describing four different representational attachment strategies (security, deactivation, hyperactivation, and disorganization), yielding scores between −1.0 and +1.0 for each attachment strategy. Due to extremely high negative correlations between the scales of security and deactivation (r = .98), the deactivation scale was omitted in the current study. High-security scores represent a child who is collaborative and open when confronted with attachment-related themes. The child can display a wide range of positive and negative affective states, enact parental guidance, and invent stories in which the parental figures are supportive and give comfort. High scores in hyperactivation correspond with a child being interested in the task but at the same time being overaroused and anxious, leading to a limited capacity to enact constructive completions of the story stems. Children receiving a high score in disorganization exhibit aggression, destruction, or loss of control with incoherent, chaotic, and bizarre narratives. Parental control is expressed extremely or violently. In some cases, role reversal can be observed.
The Attachment Story Completion Task was videotaped, translated into German, and subtitled. Videos were coded by a trained German psychologist who was blinded to other data or child characteristics.
Disturbances of Attachment Interview (DAI).
The DAI is a semistructured interview administered to the child’s primary caregiver that comprises eight items assessing different symptoms of disordered attachment (Smyke & Zeanah, 1999). Each item is coded as 0 (rarely or minimally), 1 (sometimes or somewhat), or 2 (clearly), according to the severity and frequency of behaviour described by the caregiver. Five out of eight items are indicative of behaviours relevant to reactive attachment disorder (RAD), resulting in a score between 0 and 10. The remaining three items assess symptoms of disinhibited social engagement disorder (DSED), resulting in a sum score between 0 and 6. Previous studies have found high internal consistency for both subscales with Cronbach’s α values of .80 and .83, respectively (Smyke et al., 2002). Additionally, Gleason et al. (2011) demonstrated the criterion validity of the DAI. In the present study, interrater agreement between two raters was calculated for 20% of interviews and was very good for items from both subscales (r = .95 for RAD symptoms and r = .89 for DSED symptoms). The raters were blinded to other data on the child’s experiences and characteristics.
In addition to the sum scores for RAD and DSED symptoms, we used the criteria proposed by Gleason and colleagues to create a categorical score for both RAD and DSED symptoms, i.e. at least three out of five items assessing RAD symptoms and at least two out of three items assessing DSED symptoms with a score >0 (1 – child sometimes or somewhat demonstrates the behaviour; 2 – child clearly demonstrates the behaviour).
Sociodemographic Information.
Sociodemographic data and information on foster children’s experiences before moving to the current foster family were collected from different sources. (Foster) parents completed a questionnaire about their years of education, family income, and other sociodemographic data. Furthermore, social workers provided information about the foster child’s sociodemographic data, placement history, and reasons for out-of-home care.
Statistical Analyses
Statistical analyses were performed using IBM SPSS 28. Differences in mean scores were calculated using t-tests and univariate and multivariate ANOVAs. Associations among continuous variables were calculated using bivariate (Pearson and point-biserial correlations) and partial correlations. Correlations with current age and gender were examined to control for age or gender effects. All tests were two-tailed, and an alpha level of p < .05 was used. The results with a p value <.10 are reported as trends. Both AQS security scores and ASCT scores for security, hyperactivation, and disorganization (r) were transformed into Fisher Z scores because the metric of r becomes nonlinear at its extreme values, and Fisher Z transformation represents a solution to this skewness (Mullen, 1989; Rosenthal, 1991).
Results
Preliminary Analyses: Effects of Current Age and Gender
The three study groups did not differ in the distributions of age or gender. No significant associations with age or gender were found for the AQS security score or both DAI subscales. However, age and gender were associated with attachment representations. The following statistically significant differences were found for all subgroups as well as for the total sample (except for results of the hyperactivity score – see below). With increasing age, children showed significantly higher security, r(84) = .43, p = .000, less hyperactivation, r (84) = −.25, p = .02, and less disorganization, r(84) = −.42, p = .000. Regarding gender differences, the results revealed that boys (M = −.19, SD = .34) showed significantly lower attachment security than girls (M = .04, SD = .45), t (81.88) = −2.66, p = .005. Finally, boys (M = .09, SD = .12) in both foster care groups showed significantly higher hyperactivation than girls (M = .01, SD = .17) (t foster children (54) = 2.18, p = .034). Therefore, age and gender were included as covariates in relevant analyses.
Attachment and Symptoms of Reactive Attachment Disorder and Disinhibited Social Engagement Disorder Across Study Groups
Descriptive Data on Attachment Behaviour, Attachment Representations, and RAD and DSED Symptoms for the Two Foster Care Groups and the Control Group.
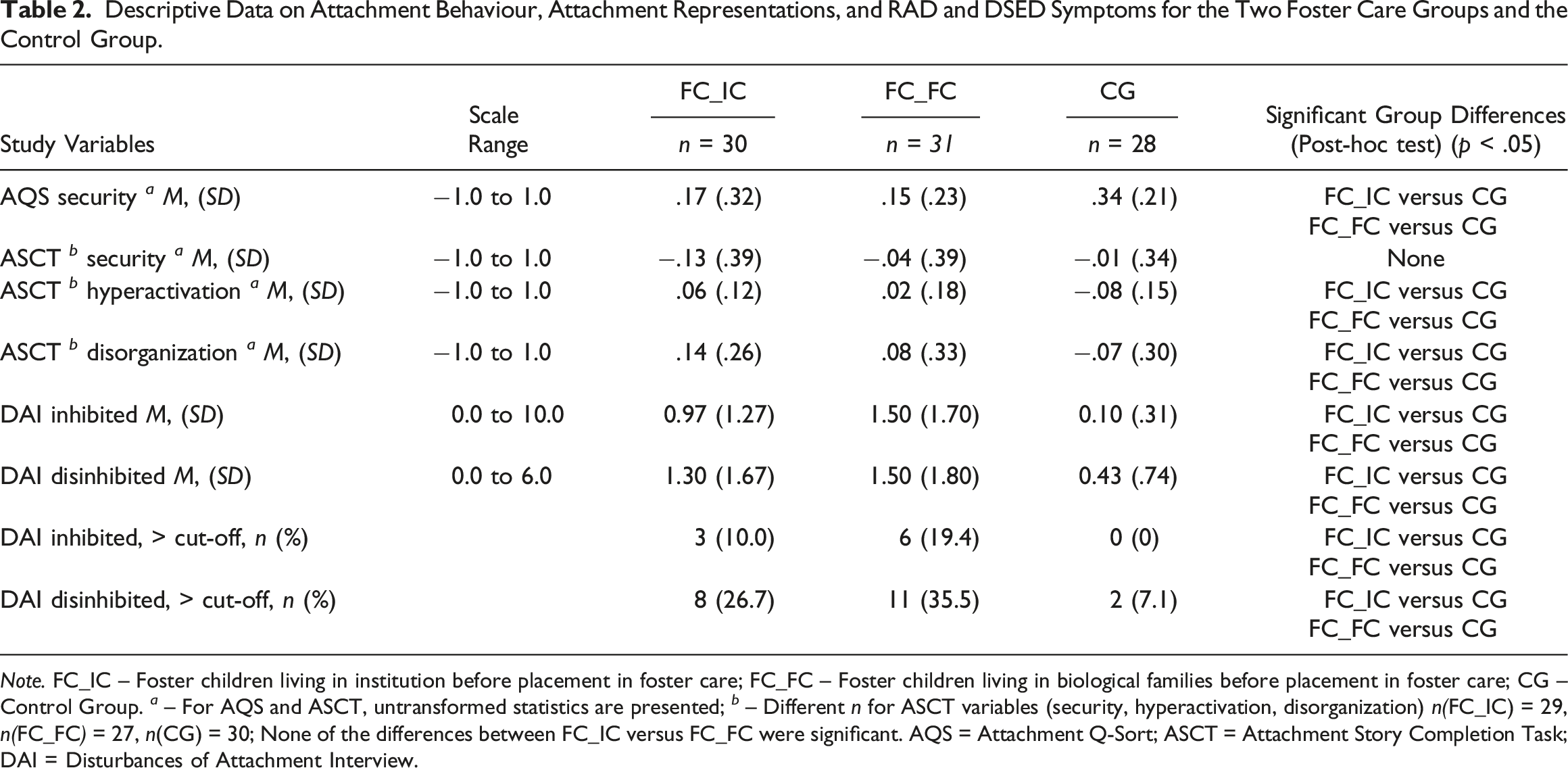
Note. FC
Attachment Behaviour (Attachment Q-Sort).
One-way ANOVA was performed to compare attachment security among the three study groups. As the assumption of homogeneity of variance was violated, Welch’s ANOVA was used, which resulted in a statistically significant difference between the groups, Welch’s F(2, 56.39) = 6.35, p = .003, η
Attachment Representation (Story Stem Completion task)
First, a multivariate analysis of covariance was performed with ASCT security, hyperactivation, and disorganization scores as dependent variables and group as a between-subject factor, while age and gender were included as covariates. After controlling for covariates, 1 a significant main effect of group was found, V = .18, F(6, 154) = 2.51 p = .024, η 2 = .09, indicating that study groups differed in ASCT variables. Separate analyses for the three dimensions revealed significant differences among the three study groups for only hyperactivation, F(2, 78) = 7.08, p = .002, η 2 = .154, and disorganization, F(2, 78) = 5.06, p = .009, η 2 = .12. Means and standard deviations for all three groups on three dimensions of the ASCT can be found in Table 2. Follow-up univariate analyses of covariance revealed a statistically significant difference in hyperactivation between the FC_FC group and the comparison group, p = .004, as well as between the FC_IC group and the comparison group, p = .000. For ASCT disorganization, there was a statistically significant difference between the FC_FC group and the comparison group, p = .015, and the FC_IC group and the comparison group, p = .000. Thus, foster children of both study groups showed significantly higher hyperactivation and disorganization than the control group.
Symptoms of Reactive Attachment Disorder and Disinhibited Social Engagement Disorder
The prevalence rates of marked RAD symptoms (Gleason et al., 2011) were 10% (FC_IC) and 19.4% (FC_FC) in foster children, whereas no child in the control group displayed marked RAD symptoms. Fisher’s exact test was statistically significant, p = .047. Marked DSED symptoms were found in 26.7% (FC_IC) and 35.5% (FC_FC) of the foster children compared to 7.1% of the children from the control group. Fisher’s exact test was statistically significant, p = .025.
In terms of mean scores on the inhibited subscale of the DAI, a statistically significant difference was found among the three study groups, Welch’s F(2, 43.15) = 15.33, p = .000, η 2 = .17. Post hoc analyses showed that both groups of foster children had significantly higher RAD scores than the control group (FC_IC group p = .003, and FC_FC group p = .000). The difference between the two foster care groups was not statistically significant. Referring to the mean scores on the disinhibited subscale of the DAI, a statistically significant difference among the three groups was found, Welch’s F(2, 50.47) = 6.43, p = .003. Post hoc analysis revealed a significant difference between the foster care group without experiences of institutionalization (FC_FC) and the control group, p = .016, and between the foster care group with prior institutionalization (FC_IC) and the control group, p = .034.
Relationships Among Children’s Attachment Behaviour, Attachment Representations, and Symptoms of Reactive Attachment Disorder and Disinhibited Social Engagement Disorder
Correlations Between Attachment Behaviour, Attachment Representations and Symptoms of RAD and DSED in Foster Children.
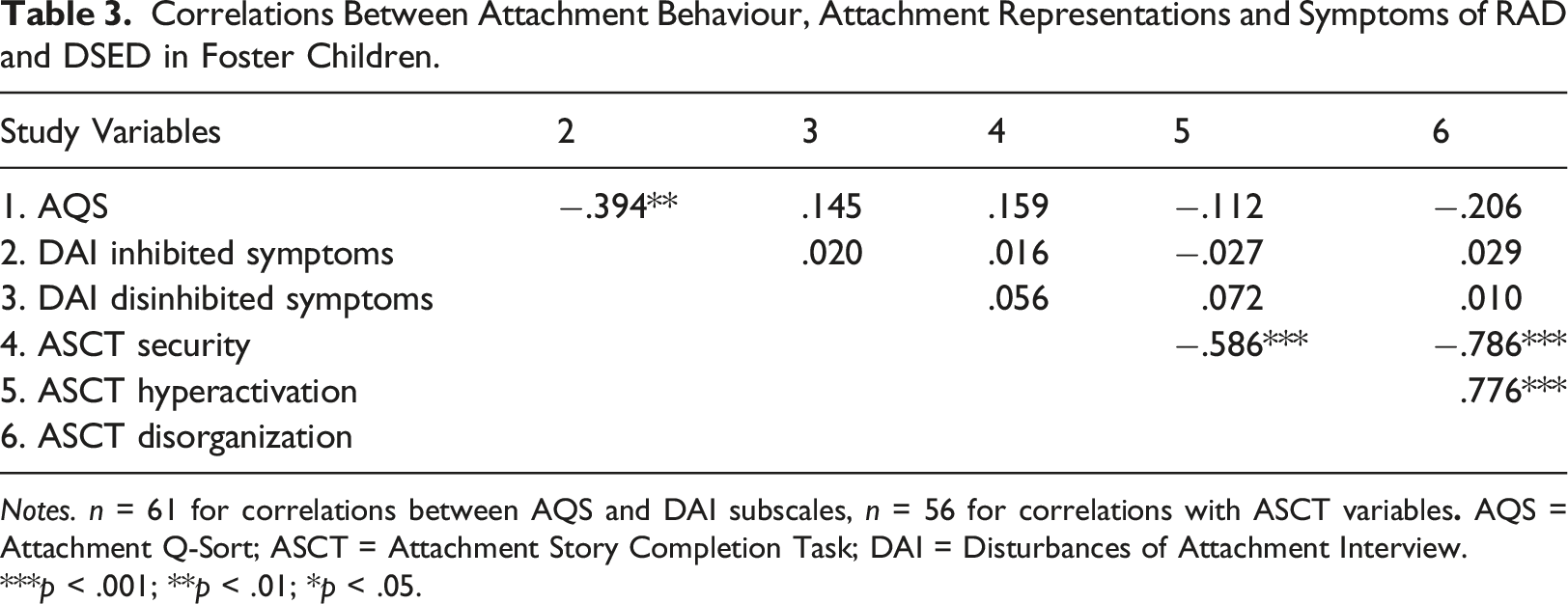
Notes. n = 61 for correlations between AQS and DAI subscales, n = 56 for correlations with ASCT variables
***p < .001; **p < .01; *p < .05.
Relationship between Preplacement Characteristics of the Child and Attachment Variables
Referring to research question 3, we performed bivariate correlation analysis of all attachment variables (attachment security on a behavioural level, ASCT dimensions, RAD, and DSED symptoms) and preplacement characteristics (the number of placements, the duration of institutionalization, age at placement in the first foster family and age at placement in current care). Previous research showed that attachment security on the behavioural level (Carlson et al., 2014) and on the representational level (Gloger-Tippelt & Kappler, 2016) tend to be related to child’s current age, with older children showing higher security levels. In both foster care groups, the child’s age was related to AQS and ASCT variables. Therefore, age was controlled for in all analyses including AQS and ASCT variables.
Correlations Between Attachment Behaviour, Attachment Representations, RAD and DSED Symptoms and Preplacement Characteristics In Two Foster Care Groups.
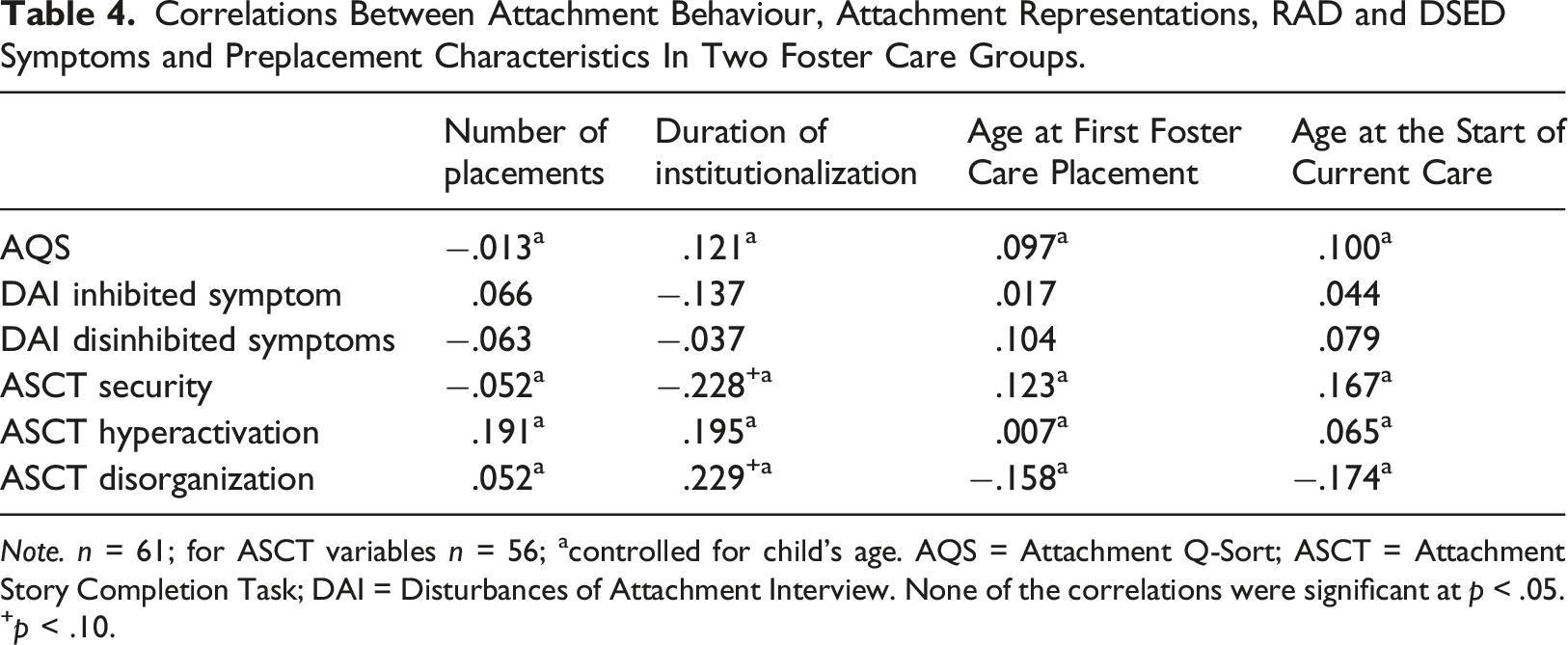
Note. n = 61; for ASCT variables n = 56; acontrolled for child’s age. AQS = Attachment Q-Sort; ASCT = Attachment Story Completion Task; DAI = Disturbances of Attachment Interview. None of the correlations were significant at p < .05. +p < .10.
Discussion
This study aimed to extend knowledge on attachment in children moved to foster care after their first year of life. We examined foster children’s attachment security and attachment representations, as well as the presence of RAD and DSED symptoms, and compared their scores with those from a community sample. Our results revealed lower attachment security among foster children on the behavioural level, as well as higher hyperactivation and disorganization on the representational level, compared to the control group. Moreover, approximately 15% of foster children showed marked RAD symptoms, and almost one-third had marked DSED symptoms, indicating increased rates of both types of disorders of attachment and sociability. Surprisingly, we did not find any significant differences between foster children with and without institutional experience.
In terms of attachment behaviour, both groups of foster children in our sample had difficulties forming secure attachment relationships with their foster caregivers. Although this finding seems to contrast that of meta-analyses by van den Dries et al. (2009) and Vasileva and Petermann (2018), this discrepancy may be explained by the influence of child age when entering foster care. For example, the meta-analysis by van den Dries et al. (2009) showed that children who were adopted after 12 months of age were less securely attached than those adopted at younger age. Similarly, two more recent studies on foster children who moved to foster care after their first year of life (Bovenschen et al., 2016; Carrera et al., 2021) found that these children exhibited lower attachment security than normative samples. Older children seem to need more time to build stable relationships with their new caregiver, and when distressed, they tend to show behaviour that pushes caregivers away (Stovall-McClough & Dozier, 2004). Hence, our results indicate that developing a trusting relationship might be challenging for children who move to foster care after their first year of life and that their foster families may need more postplacement support to foster secure attachments.
On the representational level, we found increased hyperactivation and disorganization in foster children compared to the community sample. This finding is in line with other research on foster and adopted children. Higher attachment hyperactivation (Román et al., 2012) and disorganization on the representational level have frequently been reported (Bovenschen et al., 2016; Carrera et al., 2021; Garcia Quiroga et al., 2017) and may be explained by enduring effects of preplacement experiences of maltreatment and/or neglect (Cyr et al., 2010).
In terms of attachment security on the representational level, we did not find significant differences between the foster care groups and our community sample. However, the mean security score of the community sample in the current study was lower than findings in other studies (Bovenschen et al., 2016; Miljkovitch et al., 2004). This may be explained by the low socioeconomic status of the control group, which was matched to that of the foster families. Thus, further data may be required on attachment security at the representational level in less disadvantaged populations.
Marked symptoms of RAD were found in up to 15% of all foster children, and nearly one-third (31.1%) showed marked DSED symptoms. This finding is in line with previous studies reporting lower rates of RAD symptoms than DSED symptoms in foster children who have been in their current placement for longer periods (Smyke et al., 2012; Zimmermann, 2015). This finding is also reasonable, as both foster care groups consisted of foster children who moved to foster care after being exposed to adversity in the first years of life (i.e., children with experiences of institutionalization or with experiences of abuse and neglect). Again, our findings highlight the importance of the availability of psychological services for foster families, as marked symptoms of these two disorders could induce disturbance and resentment in family life (Kroupina et al., 2023; R. Nelson et al., 2020).
In sum, our findings demonstrate that children with aversive experiences in early life struggle to develop a secure attachment to their caregiver and show elevated rates of hyperactivation and disorganization as well as more RAD and DSED symptoms. However, in contrast to our expectation of finding more problems in postinstitutionalized children than in children who moved to foster care after living with their biological families, we did not find any differences in attachment between the two groups of foster children. At least three factors may have contributed to this. First, the majority of foster children without institutionalization in our sample had experienced neglect and emotional abuse in their biological families, which might have been as detrimental as institutionalization. Second, 76.7% of previously institutionalized foster children had lived at their current placement for more than 2 years, and specific effects of institutionalization could have faded with time. Finally, postinstitutionalized foster children lived in an institution with smaller groups and low child-to-caregiver ratios before moving to foster care. Although the quality of care in this institution was still low (Jorjadze et al., 2018), the ongoing welfare reforms may have mitigated the negative effects on child’s development.
Concerning the second aim of our study, we found a negative association between attachment security and RAD symptoms in our foster care sample. However, the analysis did not reveal a statistically significant association between attachment and DSED symptoms. Our finding on RAD symptoms is in line with the findings of several studies investigating symptoms of RAD and DSED in postinstitutionalized children. These results indicate a weak to moderate association between symptoms of inhibited attachment disorder and attachment security (Gleason et al., 2011; McGoron et al., 2012; Zeanah et al., 2005). According to the DSM 5, the fundamental aspect of reactive attachment disorder is an underdeveloped attachment between the child and the caregiver (American Psychiatric Association, 2013), and RAD symptoms tend to be responsive to interventions and improvement in quality of care (Zeanah & Gleason, 2010). In contrast, the essential features of DSED are culturally inappropriate, overly familiar behaviours with strangers. Associations between symptoms of DSED and attachment security are debated. A recent meta-analysis (Zephyr, Cyr, Monette, Archambault, et al., 2021) found a significant but small association between attachment security and DSED symptoms when nonobservational measures were used. Due to the small effect size across all studies detected by Zephyr, Cyr, Monette, Archambault, et al. (2021), one explanation for the nonsignificant association in our study could be the small sample size, which may not have been sufficient to detect small effects due to lack of statistical power. Several other studies with comparable sample sizes also did not find an association between secure attachment-related behaviours and indiscriminate behaviours in foster and adopted children or children living with their biological parents (J. Bruce et al., 2009; Pears et al., 2010; van den Dries et al., 2012;Zephyr, Cyr, Monette, Langlois, et al., 2021).
We did not find significant associations between the two measures of attachment security. Our finding contradicts the findings of Bretherton et al. (1990) but is in line with those of two previous studies (Bovenschen et al., 2016; Stievenart et al., 2012) and underscores the idea that these two instruments might capture different facets of the same attachment system (Spangler & Zimmermann, 1999). While the Attachment Q-Sort captures the attachment security of a child to a particular caregiver, the ASCT measures representations of attachment that are derived from interactions in broader caregiving contexts. Thus, if a child’s experiences with the current main caregiver differ significantly from those with other caregivers, attachment measurements capturing different aspects of the attachment system may diverge. Specifically, in the case of foster children, adverse experiences with previous caregivers seem to influence their attachment representations even years after placement, whereas attachment security on the behavioural level seem to be mainly influenced by experiences with the new main caregiver and, thus, is changed more quickly by positive caregiving experiences, as also shown in adoptive families (Palacios et al., 2014).
Referring to our third research question, we did not find significant associations between specific preplacement experiences and attachment variables. The duration of institutionalization was the only variable with a potential difference, showing that children who had spent more time in an institution, showed lower security and higher disorganization on the representational level. This is in line with the findings of Lionetti et al. (2015) and reflects the enduring effects of institutional rearing on children’s attachment development. However, overall, our results provide limited evidence of differential effects of preplacement experiences on attachment and symptoms of disordered attachment and sociability. In contrast, two longitudinal studies reported that specific preplacement experiences influenced attachment (Carlson et al., 2014; Lang et al., 2016). However, in both studies, the effects were significant only immediately after placement in foster care and disappeared in the first year of placement. Thus, it is possible that the differential effects of prior aversive experiences diminish over time, and the current caregiving characteristics and quality of care might increasingly become important and influential compared to past experiences (West et al., 2020).
Due to the limited number of studies on differential effects of early adversity on attachment, more studies are needed to evaluate the impact of specific dimensions of early adverse experiences on both attachment behaviour and representations and disorders of attachment and sociability.
Limitations
Several limitations should be considered when interpreting the findings of our study. First, the cross-sectional design of the study limits the interpretation of our findings, as we did not have information on attachment-related variables before and shortly after placement in the current foster family. This also prevented us from determining the effects of parental separation on the attachment variables, which might be relevant for children entering foster care from biological families. Second, the sample size of the study groups was small, which could hinder the detection of small effect sizes. However, with support from the service agency responsible for foster care, we were able to include more than two-thirds of all eligible children in foster care at the time of data assessment, enhancing the representativeness of the sample. Next, assignment to study groups was challenging in some cases, as some children had experienced both family and institutionalized care before placement in foster care. Signs of RAD and DSED were only assessed based on reports from caregivers. Thus, we did not use observational data, as recommended in recent literature (Zephyr, Cyr, Monette, Archambault, et al., 2021). Case files of foster children were often ambiguous, and some information on children’s preplacement experiences was lacking, which might have impeded the identification of associations between early adversity and attachment. Moreover, in the comparison group information about child maltreatment was gathered from children’s parents. Thus, the possibility that these children previously had experiences of maltreatment in the family cannot be excluded.
An additional limitation may arise from the fact that the video recordings of children’s verbal responses during the ASCT had to be translated into German and subtitled. Inaccuracies in these translations might have caused some misunderstandings by raters.
In the recruitment of the control group, we intentionally approached families from lower socioeconomic status to match the comparison group with the study groups. This might have introduced some selection bias such that families perceiving difficulties in their children agreed to participate, although the control group showed considerably better outcomes on nearly all variables. The generalization of our findings to foster children in other countries should be considered with caution. Child welfare systems differ from country to country, as do community support services available for foster parents. Psychological services and other resources for foster families in Georgia are not comparable to the support available in most high-income, Western countries.
Conclusion
Our findings indicate that foster children who moved to foster care after their first years of life, independent of their previous placement experiences before moving to foster care, showed low attachment security on the behavioural level, high hyperactivation and disorganization on the representation level, and more symptoms of RAD and DSED. Moreover, we were not able to find significant differences in attachment variables between foster children with and without institutionalized experience, which might indicate that maltreatment within the family and early institutionalization may be equally detrimental to child’s attachment development. Our findings highlight the fact that all foster families with children who moved to foster care after their first years of life need social and psychological support services. Especially in developing countries, where large-scale institutions were the only form of alternative childcare until recently, it is essential to expand the availability of community resources for disadvantaged families and foster families.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Shota Rustaveli National Science Foundation (DO/383/2/-200/14).