
Abstract
Alcoholism, more professionally termed alcohol use disorder (AUD), is a widespread and costly behavioral health condition. The aims of this paper are draw attention to systemic gaps in care for patients with AUD and advocate for patient safety leaders to partner with both the mainstream medical and substance abuse treatment communities to reduce harm in this patient population. The authors performed a narrative review of the literature on the current state of AUD treatment and patient safety, finding extensive evidence that patients with AUD usually go undiagnosed, unreferred and untreated. When they do receive AUD treatment, little evidence was found to indicate that a patient safety approach is incorporated into their care. Behavioral medicine is virgin territory for the patient safety movement. Medical care and behavioral medicine in the United States currently constitute two separate and unequal systems generally lacking in pathways of communication or care coordination for AUD patients. Significant barriers include institutional culture, individual and systemic bias against those with AUD, and health care infrastructure, especially the separation of medical and behavioral treatment. It is the authors’ conclusion that care of patients with AUD is unsafe. We advocate for the patient safety approach common in American hospitals to be extended to AUD treatment. Experienced patient safety leaders are in the strongest position to initiate collaboration between the mainstream medical and substance abuse treatment communities to reduce harm for this patient population.
Keywords
Current state
A 45-year-old male with a history of alcoholism and inability to remain sober has exhausted options for private care. Patient X was placed in a licensed short-term housing facility with care service limitations. During his stay, he had an episode of alcohol withdrawl, with violent outburst and psychological instability. Staff at the residential facility were unable to manage the situation, and had him moved to a large, inner-city trauma center for care. The patient was given a document with a physician's name on it prior to accessing transport to the hospital, told to see this physician, driven to the hospital, and left at admissions, curbside. The driver left without confirming the patient was seen at the hospital or by the appropriate clinical team.
The day after drop-off, the family tried to obtain follow up information about the patient’s hospital care. They were told he had not been seen in the emergency room, and they could not account for his wereabouts. Later that day, he was discovered exiting a manhole on the hospital grounds, naked.
Patient X died two years later of acute alcohol and medication intoxication.
Alcoholism, more professionally termed alcohol use disorder (AUD), is a widespread and costly behavioral health condition. According to the Centers for Disease Control and Prevention (CDC), it constitutes the third-leading preventable cause of death in the US—after tobacco use and the combination of poor diet and sedentary lifestyle. 1 The scientific definition of AUD is “A chronic brain disorder marked by compulsive drinking, loss of control over alcohol use, and negative emotions when not drinking … Recovery is possible regardless of severity.” 2
Many factors influence how patients experiencing AUD are treated in healthcare settings including negative sociocultural perceptions associated with persons with AUD. Widespread bias toward those with AUD is often linked to an assumption among healthcare professionals, patients, family members and the public-at-large that treatment is useless and will be unsuccessful. The disorder tends to be falsely viewed as moral turpitude, a character flaw, or a failure of will, rather than a treatable behavioral disorder. 3 The stigma and implicit biases directed at patients with AUD is widespread in many healthcare settings, including inpatient and outpatient, medical and behavioral. 4
Much has been said and written about the physical, psychological, and social harms of AUD. However, the patient safety community has given little attention to the AUD patient population, as evidenced by the lack of patient safety research and action in the behavioral health setting. Few resources have been identified to address patient safety issues for this population in research, diagnosis, treatment, programmatic initiatives or outcomes. The patient safety community has yet to explicitly consider, adapt, and apply patient safety concepts and evidence-driven actions to the care of these patients, as reflected in the paucity of articles and initiatives on AUD found in the patient safety space. It is far more common to find research and published reports about safety issues due to substance abuse in clinicians than the safety of patients with the disorder.
The purpose of this narrative review is to draw attention to systemic gaps in care for patients with AUD and advocate for patient safety leaders to partner with both the mainstream medical and substance abuse treatment communities to reduce harm in this patient population. The search consisted of review of databases including PubMed, SCOPUS, OVID, Medline, and EMBASE and a review of online patient safety and addiction resources such as the AHRQ's Patient Safety Network, books, governmental reports, websites, journals, and reports. The broad database search was undertaken by a healthcare librarian exploring concepts associated with: alcohol addiction, abuse, OR dependance, OR alcohol use disorder OR alcohol use disorders OR alcoholic intoxication and outcomes, care continuity, treatment effectiveness, patient safety, medical errors, healthcare quality OR screening. The time frame was open as newer material relevant to the topic was limited. The results were initially reviewed by a content curator with 20-plus years’ experience assessing the medical literature for relevance to a broad patient safety audience (L. Zipperer). The results from this reviewer's analysis of safety concepts, rather than generic quality concepts, were then shared with the other authors who used who used these preliminary findings in addition to their individual searches to support their final contributions. The resulting paper highlights barriers to safe treatment, as well as tactics and systems interventions that are available to ensure safe care for the AUD patient population.
Two separate and unequal systems of care
Convergence of the challenges of COVID-19 and the opioid epidemic have shed light on weaknesses and inequities in healthcare, particularly for marginalized5,6 communities 6 whose plights are less “sexy” but still in need of attention, such as homelessness, obesity, or alcoholism. 7
The National Academy of Medicine (NAM) takes a firm position on treatment of alcohol use disorders. A 2020 NAM Perspective describes treatment of patients with AUD as inadequate and systematically divorced from traditional healthcare, creating two separate, unequal, and non-communicating systems: one using behavioral treatment approaches and the other using classical medical approaches.6,8 Few acute hospitals maintain inpatient units or beds for behavioral disorders9,10—even as American hospitals and large academic centers aggressively buy up other hospital systems and construct new buildings for more lucrative services like ambulatory surgery and cancer treatment. 11
Private-pay residential treatment facilities and partial hospitalization programs are untethered from main healthcare delivery systems and therefore lack resources to fully implement safe, efficient, and holistic treatment programs. This segregation of AUD treatment from mainstream healthcare exacerbates the silo effect, representing a system failure that perpetuates uncoordinated care, loss of information upon transfer, and lack of integration of addiction specialists into the medical team caring for persons suffering from AUD. 12
Undiagnosed, unreferred, untreated
Patients with AUD are over-represented in hospital emergency departments (ED) which may be due to a lack of AUD resources in the community to proactively care for the population. As a result, the ED is situated as a potential location for identifying undiagnosed AUD, but these patients are not routinely screened for the condition. Consequently, they are not typically evaluated for diagnosis, referral, or initial treatment plans while at an entry point of the healthcare system, and there is the potential for gender bias that leads to underdiagnosis in women. 13
Likewise in the inpatient setting, patients with AUD are over-represented, accounting for as many as 31% of hospitalizations, and there are likely others that have not been identified.14,15 Inpatient stays provide yet another opportunity to screen and identify AUD. 8 However, hospitals fail to screen patients for AUD, even when they present with blood alcohol concentrations signifying severe intoxication16,17 or in trauma centers where alcohol and substance abuse are commonly a root of accidents. 18
In the ambulatory primary care setting, 20% of patients present with medical problems related to alcohol use, but physicians often manage the presenting problem without addressing the underlying alcohol use disorder. 19
In all these settings—emergency, inpatient, and ambulatory care—clinicians report they feel unprepared and untrained to detect, refer or treat people with AUD.4,20–23 The result is that patients go unscreened and undiagnosed, and therefore are left vulnerable to worsening conditions.24,25 As a result fewer than 10% of those with alcohol use disorder receive any treatment, 12 and fewer than 2% have ever received medications for AUD.8,26 There are missed opportunities for identification and treatment of AUD patients, resulting in preventable death and harm and negative financial, emotional and management implications for a large portion of patients seen in all of the traditional healthcare settings across the US.
AUD through the patient safety lens
There are two key reasons why patients are at increased risk for harm if they have AUD: 1) if AUD is not recognized at all and, 2) if recognized and referred, the treatment is fragmented and suboptimal. There are three overarching factors that contribute to the degradation of safety in the care of AUD patients: stigma and biases, poor organizational culture, and misaligned infrastructure.
Stigma and Biases: Stigma is defined as a mark of disgrace associated with a particular circumstance, quality, or person. Bias is a tendency, inclination, or prejudice toward or against something or someone. Considered either individually or together, they are a primary underlying factor contributing to the unsafe care of patients with AUD at all levels. Societal norms and stereotypes among lawmakers, insurers, hospital administrators, healthcare practitioners, and the public negatively affect those with AUD.27,28 Persons with alcohol dependance are often viewed as not worth the time and effort to treat because it is assumed they will just go back to drinking. As Leggio and Lee state, “This deficiency reflects nihilism, stigma, and a failure to link behavioral and traditional medical research.” (
12
p.1214) The unaddressed influence of stigma and biases can result in:
denial of care or provision of substandard care, loss of AUD patient trust leading to lack of willingness to engage, physical or mental abuse of AUD patients, referral of AUD patients to junior, possibly less qualified colleagues.
28
○ uncoordinated care,
30
○ tolerance of clinician biases against patients with substance abuse disorders,
6
○ under-utilized or non-existent systems to report concerns, near-misses or mistakes,
31
○ impact of professional disrespect
32
fostered by medical system hierarchy that limits the application of training, skills, and knowledge, of the range of allied health professionals that interact in the behavioral health space,
33
○ underdeveloped and underresourced improvement initiatives, ○ nonexistent organizational learning from failure. ○ lack of interoperability between electronic health record (EHR) systems that can contribute to poor information transfer, access, and quality. If the hospital system and the behavioral health system do not share the same EHR platform neither will be able to successfully access patient records resulting in potential for error.
34
○ physical layouts that block easy visual access to patients, ○ lack of processes that ensure patients transfer without incident or loss of information through the healthcare system as treatment needs change,
35
○ lack of training programs that support and motivate staff competencies to support the work,13,36 ○ poor staffing levels that minimize effective evaluation, diagnosis, treatment (and/or transfer when necessary),16,37–40 ○ no structured effort to identify and inform failure analysis activities which include an actively used, updated, and reviewed database of safety incidents involving AUD patients,
41
○ minimal resourcing of point-of-care training to ensure reliable screening, treatment, and transfers.
Ineffective Organizational Culture: Organizational culture is the manifestation of the attitudes, behaviors, beliefs, and expectations of the organization.
29
Organizational culture strongly influences, even determines the actions and outcomes that occur within the facility, yet it remains understudied and underaddressed as an influence in addiction care. Recognizing the effect that a lack of safety culture has on treatment of AUD patients is a first step to identify the extent of failures and initiate change for this population. Patients may be harmed by attitudes and culture within the organization resulting in:
Misaligned Infrastructure: Infrastructure is the skeleton on which success of behavioral health and medicine program implementation success is determined. Organizations or initiatives do what they are designed to do; therefore, infrastructure should ideally be planned, built, funded and updated to accord with the current healthcare culture to address gaps in care that degrade safety for patients with AUD. Weak infrastructure contributes to:
These factors will need to be addressed by the healthcare system at large. New patient-safety driven approaches need to be instituted by individual hospitals/health systems, carried out by clinicians, and supported by patients, families, and community members.
Examining problems in AUD care as patient safety problems
Table 1 includes a selected set of AUD care problems identified in the literature reviewed that are exacerbated by infrastructure barriers: threat of physical harms; diagnostic errors; medication errors; and care discontinuities in referrals, transfers and discharges. Error reduction strategies are suggested from the literature to illustrate what organizations and cliniicans could do to improve patient safety for this patient population. Reorganizing how stigma, bias, culture and infrastructure inform attitudes, actions, assessments, and care can influence the patient experience. Embedding safe frontline processes, identifying actionable steps to mitigate the barriers listed above, and prioritizing safe treatment of AUD patients at the leadership level will result in a more holistic approach to care and safety of the AUD population. Staff will benefit from becoming aware of safety concepts, training to use them and tracking outcomes. Then patient safety becomes the norm rather than the exception.
Safety challenges in AUD care: system and staff actions for improvement.
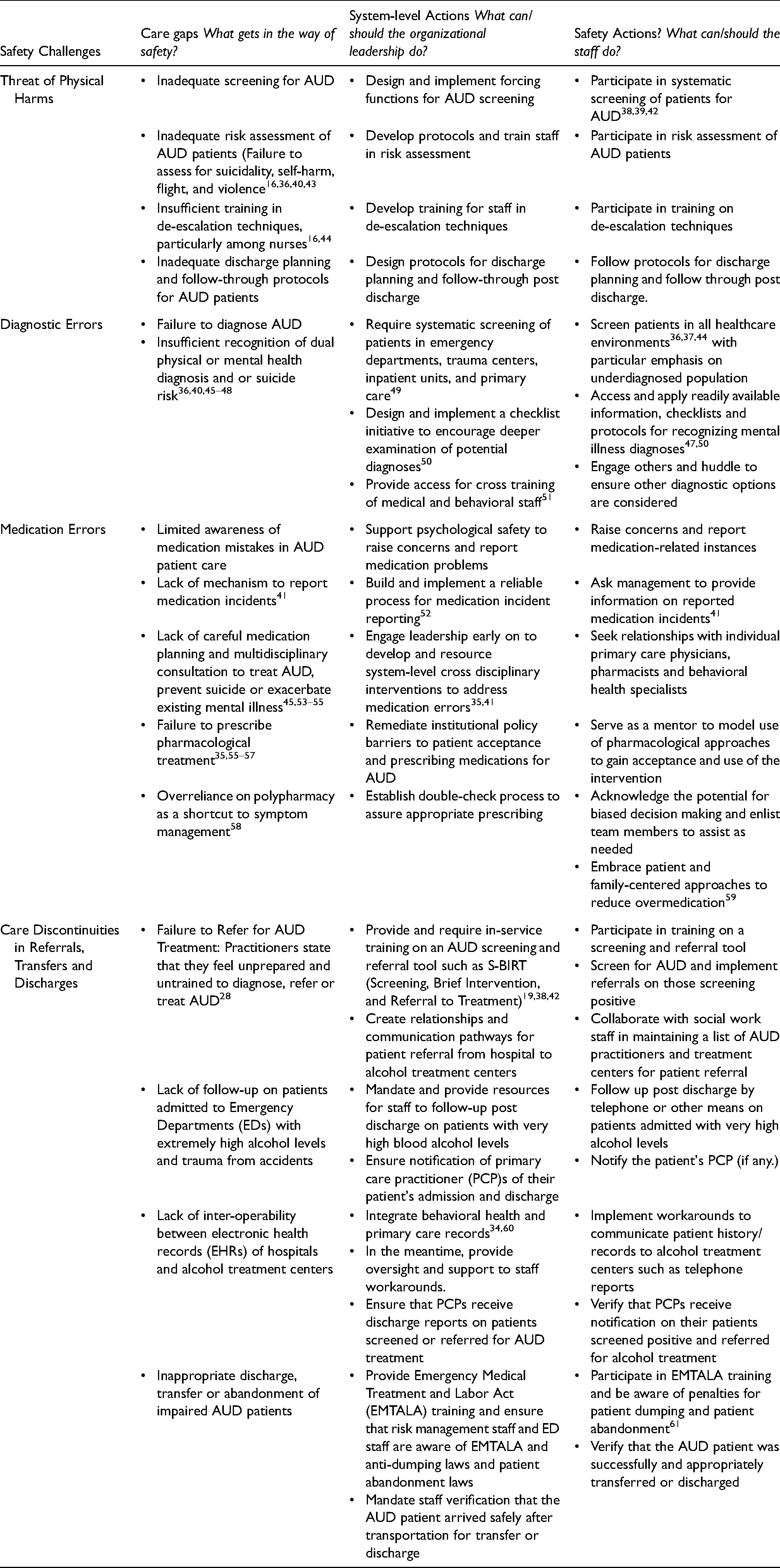
Care gaps noted in the table would be recognized, reported, and discussed as safety issues using language embedded in patient safety discourse and research. Organizational-level actions systemic in nature and thus apt to change, if implemented successfully, more than one gap, would be aligned with distinct tactics that staff could use in their practice. The approach highlighted below could address the overarching influences of historic stigma and bias, poor organizational culture, and infrastructure weaknesses surrounding persons with AUD to help acknowledge the gaps as patient safety concerns and drive improvement.
Desired future state
A 45-year-old male with a history of AUD and inability to remain sober has exhausted options for private care. Patient X was placed in a licensed residential facility where, upon admission, he was assigned a care team which included an advocate with training and lived experience in substance abuse treatment to assist in the patient's management. During his stay, he experienced an episode of what was likely alcohol withdrawal, where he exhibited violent outbursts and psychological instability. The team telephoned the local hospital regarding the transfer of the patient to their care. The patient's AUD advocate assisted with his transition to higher level care.
The residential facility's electronic health record was interoperable with the electronic health record in the receiving large inner-city safety-net trauma center. The patient was taken there by a staff driver who was trained to accompany and stay with the patient until the transfer was complete. Both the patient and the driver had a copy of a document with a physician's name on it. The patient was received by the in-house care team consisting of an advance practice nurse who was an addiction specialist and a social worker. The care team retrieved the patient's record during his admission to enhance communication across all team members, including the patient, about socioeconomic and medical factors that could influence care.
During his hospital stay, patient X received a thorough evaluation and treatment for his medical conditions as well his AUD. Prior to discharge, a comprehensive treatment plan was created and shared with the staff at his residential facility and, with the patient's permission, his family. Referral to a clinician for ongoing management of his health needs and comprehensive treatment plan was also arranged.
Moving forward
Safety is one of the six domains of quality healthcare, 62 and is often compromised in the diagnosis, referral, and treatment of patients with AUD. Behavioral medicine is virgin territory for the patient safety movement. 41 Those working in the addiction community have yet to collectively embrace the safety science approach to reducing patient harm. The patient safety community engages patients, family members, clinicians, administrators, and other non-healthcare experts to work toward improvement. It is affiliated with mainstream medicine and is in the best position to help build a communication link between medical practitioners and addiction treatment staff and promote a systems-improvement, patient-safety approach to care.
Care of alcohol use disorder patients, at the time of this writing, is unsafe. Alcohol use disorder is a medical condition that warrants patient safety approaches and systems improvements to reduce failure and improve coordination of care. The application of patient safety concepts should be jump-started to reduce harm to this population, particularly harm resulting from stigma and bias, unsafe organizational culture, and inadequate infrastructure. Safety as an improvement model is presently lacking in the care of patients with AUD. Science, knowledge, passion, and compassion are needed to generate true systemic change for those with alcohol use disorder.
Footnotes
Acknowledgements
The authors dedicate this work to the patients, families and communities that have been adversely affected by alcohol use disorder and those trying to catalyze significant change in the daily care of such patients. In addition, recognition is extended to Bruce Abbott, UC Davis Health Sciences Librarian who executed the literature review, and Linda Williams, David Meyers, Louise Miller, Geri Amori and the peer reviewers for their thoughtful comments that sharpened and informed manuscript development.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.