
Abstract
Background
Communication and resolution programs have emerged as central to organizational responses to serious patient harm events, with demonstrated evidence of patient safety and medicolegal outcome improvements within a handful of healthcare systems. Hospitals, including those with open medical staffs, have struggled implementing communication and resolution programs, particularly around the components supporting resolution. Here, we describe our lessons learned early after implementing the resolution (“R”) component of Communication and Optimal Resolution, a comprehensive contemporary communication and resolution program at MedStar Health, a large community health system in the United States.
Context
MedStar Health is a regional healthcare system with 10 hospitals, 250 ambulatory care delivery sites, and 20 diversified businesses in the mid-Atlantic region of the United States. MedStar Health initiated Communication and Optimal Resolution implementation in 2015.
Approach
Our approach to resolution following patient harm yielded seven strategies supporting our resolution process. These included infrastructure and processes to (i) provide immediate support to patients and families, (ii) hold and waive bills, (iii) activate event review processes early to inform resolution, (iv) embrace a paradigm shift in legally defensible cases, (v) develop a communication and resolution program legal community, (vi) accept sacrifices with a principled resolution, and (vii) commit to address challenges with open medical staffs.
Summary
The resolution process in response to serious patient harm is complex. Our early experience in implementing the “R” of Communication and Optimal Resolution required enhanced infrastructure, embracing the clinician, legal, and insurance communities and instructing them in the principles of communication and resolution program, and a strong organizational commitment to “doing the right thing” for patients and families.
Keywords
Background
Transparency, zero preventable harm, and continuous learning are hallmarks of learning health systems. 1 Organizations across the United States (US) are striving to achieve the quadruple aim, better patient outcomes and experiences at lower costs while enhancing joy and meaning in the workplace, by implementing strategies coupling quality, safety, and care experiences. 2 These strategies include complex interventions such as high reliability organization training, engaging patients and families in care redesign, and embedding communication and resolution programs (CRPs) into practice. Since the seminal article describing the Lexington Kentucky Veterans Affairs Medical Center experience of “extreme honesty as a risk management strategy”, 3 CRPs have emerged as central to organizational responses to serious patient harm events. 4 CRP programs encourage transparent communication with patients and families after serious patient harm, seek a lasting and fair resolution, and support clinicians in these conversations including disclosure and apology when warranted. 5 These programs move healthcare organizations and professionals away from the practice of deny and defend to the promising approach of early communication, yielding better outcomes for patients, their families, and the staff, as well as important improvements in patient safety.
CRP models differ across the US. Early CRPs like the University of Michigan’s model of disclosure and early settlement or COPIC’s model of limited reimbursement have demonstrated important reductions in medical liability for organizations and physicians and established a core set of principles for organizations to follow when adopting CRP.4–7 These principles include (i) transparency through early, open, and honest communication with patients and families; (ii) dedication to reporting and rapid investigation of the event, (iii) commitment to fair and equitable resolution when patient harm was deemed preventable; (iv) support of the care team members involved in the event; and (v) prevention of future harm through learning and improvement. Contemporary CRPs, such as the Seven Pillars8,9 and the Agency for Healthcare Research and Quality’s (AHRQ) Communication and Optimal Resolution (CANDOR), 10 have evolved to promote intimate linkages between risk management and patient safety while embedding these core CRP principles into a systems response to serious patient harm grounded in organizational commitments to transparency, just culture, learning, and improvement.
The word resolution is defined as “the action of solving a problem, dispute, or contentious matter” or “the peaceful resolution of all disputes.” 11 In this context, we appreciate that “resolution” is a term of art describing the process of reaching financial and legal settlement between the organization and the patient and/or their family after serious preventable patient harm. For many hospitals, while there is organizational commitment to transparency and the principles of CRP, many encounter challenges when faced with implementing resolution, particularly in terms of financial compensation and the legal claims process.12,13 Tensions between doing the right thing for the patient and family and the medicolegal community’s definition of legally defensible often hinder the resolution processes within CRP. 14 Here, we describe some of our lessons learned early after implementing the resolution process of CANDOR at MedStar Health (MedStar), a large distributed healthcare system in the mid-Atlantic US.
MedStar’s resolution prior to CANDOR
MedStar is the largest healthcare provider in Maryland and District of Columbia in the US, with 6000 physicians and licensed practitioners, of which 2400 are employed, over 31,000 associates, and 1100 resident physicians. MedStar provides care to one in five patients within the region through 10 acute care hospitals and 250 ambulatory care sites. MedStar has experienced a growth in clinical exposure since 2014 relative to an ongoing expansion of ambulatory care delivery sites and acquiring a 10th hospital during this time.
MedStar’s employed physicians and associates are covered for medical professional liability claims through MedStar’s captive insurance company. MedStar also maintains commercial medical professional liability insurance coverage for claims and suits resulting in indemnity greater than MedStar’s self-insurance retention. MedStar’s claims and risk management team has long embraced a commitment to openness in the face of an adverse event, coupled with caring and compassion for the patient, their family, and our associates. Prior to CANDOR, disclosure of adverse events reported to risk management did occur; however, the claims and risk management process were somewhat disengaged from the clinical safety and improvement efforts.
MedStar’s CANDOR program
In 2012, MedStar initiated a five-year strategic plan to improve patient safety in the pursuit of the quadruple aim. 2 One of the five elements of the strategic plan was transparency through a CRP activated in response to reports of serious patient harm. In 2013, MedStar partnered with leaders from around the US to develop and pilot test a CANDOR toolkit. 10 MedStar contributed to both the development of the toolkit and piloted tested the toolkit in eight hospitals in partnership with the AHRQ.8–10 MedStar extended its CANDOR implementation to all 10 MedStar hospitals in the fall of 2015 and has since furthered its implementation to all ambulatory care sites and diversified business units.
CANDOR is initiated when a serious patient harm event is reported. This is followed by activating an immediate investigation (event review) at the local care site, a huddle with the patient safety and local care team, early communication to the patient and family, and activation of the health system’s critical incident response process including care for the care teams and notification of leadership and claims and risk management. Communication within CANDOR continues throughout the process, predicated on relaying facts as they emerge from the investigation. CANDOR is “completed” with apology and resolution if it is determined that the standards of care were not met and that this resulted in serious harm. Outcomes from the investigation are linked into MedStar’s patient safety and quality improvement activities. Our primary emphasis of the CANDOR program is on safety improvement rather than an emphasis on risk mitigation. 4
MedStar’s legal resolution with CANDOR
Prior to CANDOR implementation, MedStar had a history of early resolution in response to claims. Risk management was committed to disclosure of adverse events and transparency as well as authorized to provide offers of compensation as part of the claims management process. However, this process was limited due to incomplete or delayed event notification. Many times, the first notification to risk management of a potential patient harm event was a formal claim for compensation received months or years after the event occurred. Delays in event notification are problematic within the context of CRP for several reasons including: (i) it may introduce bias (e.g. hindsight) or lapses in memory limiting the investigation fidelity, (ii) exposes patients to additional risk due to delays in closing important safety problems, and (iii) allows an erosion of trust between the patient and family and the healthcare organization and team. Together, these challenges impede communication with patients and families and may lead to incomplete disclosure. During the early adoption and implementation stages of CANDOR, several barriers to resolution emerged. Here we define both the problems and the strategies that we have devised to overcome barriers to resolution.
Supporting the patient and family immediately
One hallmark of CANDOR is ensuring that the patient’s needs are met in the immediate aftermath of serious harm. Traditionally, this includes early, open, honest, and factual communication; activation of clinical resources to optimize patient outcomes; and pastoral or spiritual care for the family. One additional strategy has emerged as more events are reported earlier to claims and risk management—that of providing immediate support to patients or their family to avoid the financial hardships of unexpected hospital stays or disability that may be reasonably tied to the harm event. In our experience, this has included paying airfare for out-of-town family members to attend a patient in hospital or providing funds to support mortgage payments or out-of-pocket expenses. Unplanned expenses add additional stress and uncertainty to an already emotional and possibly life changing event. The MedStar claims and risk management team established structures for providing immediate financial support to patients and families. Claims managers are empowered to offer immediate compensation to avert financial hardships, usually ranging from the hundreds to the thousands of dollars (e.g. for mortgage payments), activated while the investigation of the event continues. This approach takes training, courage, empowerment, and trust. It also creates additional complexity to CANDOR adoption. Organizations must be transparent in the intent of the financial gesture (e.g. to allow patients and/or families to focus on healing and recovery), and leaders may need to absorb these expenditures if harm was not the result of a medical error.
Holding and waiving bills
Health systems adopting CANDOR are encouraged to hold and subsequently waive bills for cases of preventable patient harm. While simple in concept, operationalizing the holding and waiving of bills within a large system with open medical staffs is challenging, requiring careful planning, coordination, and oversight. Figure 1 provides the MedStar bill waiver process. All patient harm events that are considered potentially compensable immediately trigger the process for facility and professional fees. Concurrent to this, an event investigation is initiated. The results of the investigation provide the basis for resolution. If the investigation determines that the harm was preventable, all facility and professional bills are waived. When the investigation determines that care was appropriate, facility and professional bills are released.
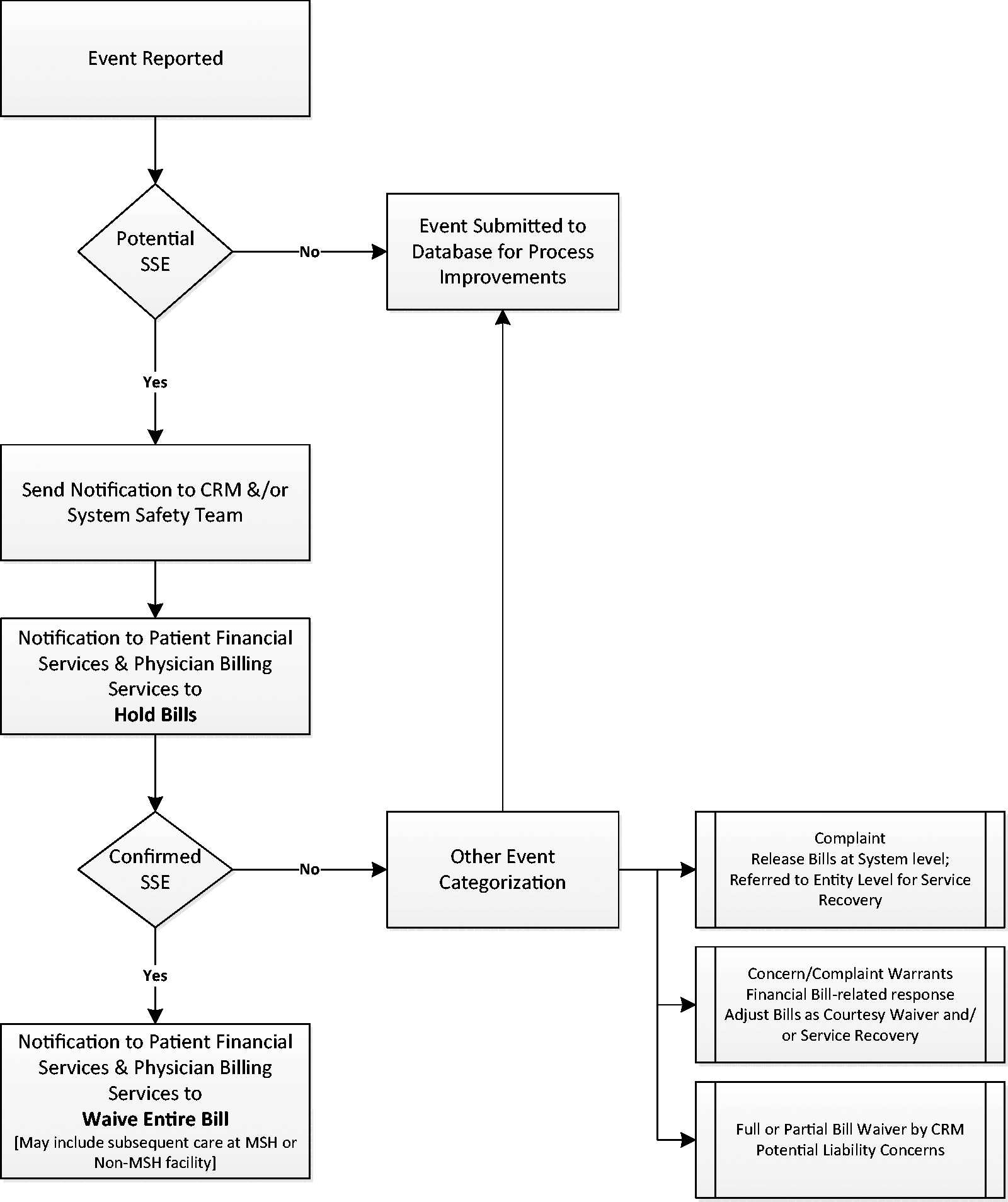
MedStar algorithm for holding and waiving bills in response to patient harm. CRM: claims and risk management; SSE: serious safety event (serious unexpected outcome).
For those cases where there is a significant time lag between the event and notification of the event, such as in the case of a missed diagnosis, the claims and risk management department works with the patient and insurers to provide restitution as appropriate.
Conducting immediate systems-based investigation to inform resolution
Root cause analysis (RCA) is a process adapted for use in healthcare from high-risk industries whereby serious adverse events are investigated to identify hazards and implement solutions to mitigate future occurrences. 15 In healthcare, the RCA process (or event investigation) traditionally brought multidisciplinary groups together to review an event, identify causal factors, and make action plans to prevent recurrence. 15 This approach has yielded limited improvements in patient safety,16,17 often taking weeks to months before the facts are available to disclose to patients and families. CANDOR employs a rapid approach to investigation that is tightly linked to the resolution process. At MedStar, our RCA process is termed an event review. For cases of serious harm, an event review is initiated within 60 min after notification of the event and often includes the patient or family.8,10 Interviews with clinicians, staff, and patients or family members are conducted within hours, and an initial assessment of the event is formulated. As the event review continues, information is shared with patients and/or their family along with system-level claims and risk management personnel. The outcome of the event review informs MedStar’s disclosure, resolution, and reconciliation process including the decision to release or waive the bills.
Embracing a paradigm shift in legally defensible cases
The “deny and defend” approach to healthcare litigation promotes defending cases of clear medical error, negligence, and never events. 18 When adopting CANDOR, health systems must come to an understanding with stakeholders including defense counsel and liability insurers, on the term “defensible.” Clinically defensible and legally defensible can vary greatly. Given decades of “deny and defend,” it may be challenging to abandon cases once considered defensible, before litigation begins. 14 As our CANDOR program matured, MedStar met with defense counsel and its liability insurers (excess carrier) to educate and inform them on a new definition of “defensible” for the system. Safety and risk management leaders also engaged the leading professional liability insurance carriers for our nonemployed physicians and plaintiffs council in an effort to inform them of our approach, establish rules of engagement in response to CANDOR events, and formulate a more amiable relationship in response to CANDOR events. This approach continues to evolve, maturing with each case.
Developing a CANDOR legal community
Adopting CANDOR requires that multiple stakeholders, including claims, risk management, legal, and patient safety, come together with the defense and plaintiff counsels in pursuit of a common goal—the swift and principled resolution to patient harm. History of adversarial relationships among these groups can often engender distrust in the process, effectively undermining the program.4,13 To this end, MedStar risk and safety leadership developed a CANDOR community, bringing together health system stakeholders with defense counsel in quarterly full day retreats. These retreats serve three purposes: (i) describe and educate on MedStar’s approach to patient harm events, (ii) discuss medical liability outcomes, and (iii) review specific cases so that defense counsel is informed and aligned with our CANDOR approach.
Be prepared for sacrifices within CANDOR resolution
Boothman and co-workers6,7 and McDonald and co-workers8,9 outline an approach to patient harm events that “rigorously defends cases where the event review determines that the standard of care has been met.” Our experience with CANDOR, however, has demonstrated that sometimes despite our best efforts patients and their family members may continue to pursue legal resolution. It is at these junctures where the organization must balance the needs not only of the patient and family, but also the care team and the organization. In some cases, it may not be in the organization’s or the clinician’s best interest to pursue lengthy litigation to rigorously defend care that met the standards. In cases where jury verdicts may be triggered by emotion and not reflective of the facts, seeking a settlement may be the most appropriate course for all parties. Box 1 describes a hypothetical situation where defending the defensible could result in a lengthy court process ending in a significant jury verdict.
19
Early settlement, however, could reduce the impact of medical malpractice stress syndrome on the clinician, moderate the financial impact of the case on the system, and provide the family with the opportunity to begin healing.20–22 Box 1. Case example.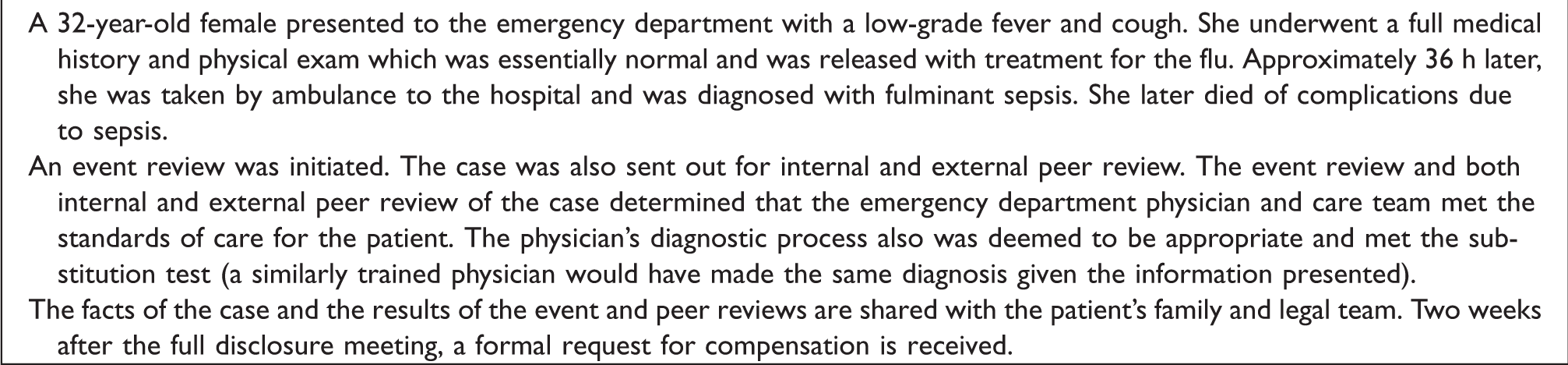
Addressing challenges with open medical staff
Unlike medical centers with closed medical staff, nonemployed physicians are much more common in community health systems, creating additional challenges for legal resolution in CANDOR. In a system with closed medical staff, coming to settlement after a serious patient harm event is somewhat straightforward. The claims and risk management for the physician and hospital are on the same side. Settlement negotiations within community health systems is somewhat more complex, often pitting the insurers of physicians and health systems against one another, at odds with the fundamental ethos of CRPs. Mello et al. 13 pointed to physician aversion to participate in the disclosure and early settlement process as a barrier to CRP implementation in hospitals with open medical staff. Our experience with CANDOR revealed a similar pattern. While physicians felt a duty to participate in the CANDOR process, insurers were less inclined to partner in early settlement negotiations, preferring to wait until a formal demand for compensation was received or until litigation commenced. In these instances, MedStar has been faced with “going it alone.” In such cases, MedStar may incur higher settlement costs by settling separately, leaving the physician in the case, or by paying the physician’s (and their insurer’s) portion of the financial settlement to move the case to early closure. Hospitals with open medical staff considering a CANDOR approach should fully understand and be prepared to address this challenge.
Summary
Our early experience with CANDOR implementation has revealed that the resolution process is complex. Our CANDOR program is still quite immature although early trends indicate an improvement in organizational transparency. Unadjusted rates of events reported to risk management observed an almost twofold increase in reported events (approximately 700/year before versus 1390/year after) and a reduced number of events first reported as a claim or lawsuit (50% before versus 29% after) in the three years following CANDOR initiation. We are also regularly reminded by our patient partners that true resolution following preventable patient harm is impossible. No amount of money or tangible support offered in reconciliation will make a family whole. Patients, and/or their families, sue not only for restitution but so that the health system responds to their loss with discovery and learning to prevent a similar event from happening to others. Additionally, settlement agreement is not the end of the resolution process for many patients and families. Several of patients who have experienced the CANDOR process, both in the immediate aftermath of harm as well as years after the event had occurred, continue to partner with us on our safety journey as part of patient and family advisory councils. In this way, CANDOR is part of the way MedStar has endeavored to achieve a collaborative relationship between their medical liability and patient safety programs to meet the patient, family, medical professional and organizational needs following serious patient harm.
Footnotes
Acknowledgements
The authors would like to thank Dr. Timothy McDonald, Director of the Center for Open and Honest Communication in Healthcare and Ms. Kelley Baker, Program Director, Research from the MedStar Institute for Quality and Safety for their editorial contributions to the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Smith received funding from the Association of American Medical Colleges, Learning Health Systems Award. The demonstration project for CANDOR was funded by the Agency for Healthcare Research and Quality under an ACTION II contract to the Health Research and Educational Trust under contract number HHSA2902010000251.