
Abstract
Background
In 2009, the Erlanger Hospital System (EHS) in Tennessee introduced a Communications-and-Resolution Program (CRP) for addressing adverse medical outcomes. The program requires transparency from their medical staff whenever a patient suffers an unexpected outcome. Healthcare professionals often fear that such transparency could lead to worse liability outcomes, especially increased litigation and reporting to the National Practitioner Data Bank (NPDB).
Methods
Using a difference-in-difference model, we compared the liability outcomes of EHS to all healthcare entities in the state of Tennessee from 2005 to 2015. We reviewed charts after CRP was implemented to determine whether there was a written request for compensation or only a verbal request for compensation.
Results
After introducing the CRP, EHS defense costs fell by 58% (p < 0.001) and the number of claims filed fell by 42% (p = 0.01), compared to that in Tennessee. We found a statistically insignificant impact on compensation at EHS after CRP was implemented compared to compensation in Tennessee. We find weak evidence of relative reductions in Total Liability Costs (p = 0.34; 95% CI = −81% to +31%). Under the CRP, 40% of paid compensations resulted from only a verbal request for money, not a written request.
Conclusion
Our results provide the first evidence using a comparison group to demonstrate that CRP can lower defense costs and claims filed in court while not significantly increasing other compensation or total liability costs. The large fraction of cases with only a verbal request for compensation suggests that there could be less reporting to the NPDB when a hospital implements CRP.
Keywords
Introduction
Unexpected adverse outcomes will always occur in healthcare settings. These events, regardless of whether an error took place, can precipitate malpractice claims and lawsuits. This paper studies how a Communication-and-Resolution Program (CRP) approach for addressing unexpected medical events impacts liability outcomes differently than the traditional approach commonly called “deny-delay-and-defend” (DDD). It compares changes in liability outcomes at a hospital system after it implemented CRP to liability outcomes changes for all medical care providers within the same state during the same time period.
Under DDD, defense attorneys instruct their clients to not talk to the patient, their family, colleagues, or hospital leaders. This impedes improvements in the quality of care because the lack of transparency hinders the identification of potential flaws in systems and personnel. Patients rarely receive an explanation for the source of the unexpected event or an offer of compensation if an error resulted in injury. Due to the high cost of litigating malpractice claims, 1 only errors resulting in egregious injury will be litigated, leaving little room for patients to seek redress when they experience less severe injuries due to medical error. The adversarial DDD approach can increase healthcare costs due to the practice of defensive medicine. 2
Unlike with DDD, healthcare systems embracing CRP investigate adverse events, explain what happened, apologize if an error caused injury, tell the patient what will be done to prevent the recurrence of any errors, and offer compensation for injuries due to error. Providers must also report the event to the hospital. CRPs typically include emotional support for healthcare professionals after an unexpected bad outcome. 3
Individual healthcare systems have begun to invest heavily in CRPs, with currently over 800 US hospitals having implemented it or beginning the process of implementing it (Personal communication, T McDonald, 7 November 2022). Legislative efforts promoting CRPs continue to build at the state level.4–9 The Federal government also seeks to improve patient safety, and the 2023 Presidential Commission report, “A Transformational Effort on Patient Safety,” recommends all hospitals implement CRP or face financial penalties. 10 This is all taking place without rigorous statistical investigations into the impact of CRP on liability outcomes. Estimates of the effects of CRP controlling for state-level and nationwide confounders are urgently needed to help policy makers and hospital systems make more informed decisions involving their medical liability program. Our investigation is especially timely in assisting and informing these efforts.
Methodology
The Erlanger Health System (EHS) is a level 1 trauma center, level 4 NICU, 838 bed public hospital system in Chattanooga, TN. It is a self-insured, open hospital system; it neither employed nor insured the physicians during the study period. EHS implemented CRP on 1 January 2009. Subsequently, EHS required that all physicians and other medical staff be transparent with patients and families in the event of an unexpected adverse outcome. Physicians were allowed to use their own medical liability insurance resolution process instead of CRP. A complete description of this CRP can be found in LeCraw et al., 11 and the Online Appendix provides a detailed conceptual discussion of how resolution under CRP differs from resolution under DDD.
Data and outcome measures
Data sources about liability outcomes for EHS include EHS's digital records of annual reports submitted by Risk Management to the actuarial company managing EHS's malpractice trust fund from 2004 to 2015 and EHS's Department of General Accounting reports on the risk management budget for fiscal years 2006–2016. Additional data from January 2016 through September 2018 provide information about compensations and dates of closure for cases that remained open at the end of 2015. The annual Tennessee Medical Malpractice Claims Reports for 2004–201512–16 contain state-level aggregated measures for comparison outcomes. EHS's Department of Process Improvement and the TN Department of Health's Joint Annual Report of Hospitals (2004–2015) 17 provide counts of annual hospital admissions. All comparisons of differences in liability outcome are calculated after normalizing by the number of hospital admissions in each year for EHS and TN. All costs are measured in 2016 dollars. The characteristics of claimants at EHS were blinded to all authors except those who worked in EHS’ Risk Management Department. The study was approved by the EHS Institutional Review Board.
Liability outcomes for EHS include external defense costs for closed and pending cases; total Risk Management Budget; the number of cases reported to Risk Management and claims filed; compensation paid; total liability cost; and the fraction of cases with no written request for compensation. Total defense costs include external defense costs plus 65% of the Risk Management Budget. This 65% is added to account for the increased administrative costs of CRP relative to the previous medical liability program. A case is defined as an event reported to Risk Management. A claim filed is defined as a case that is filed in court.
Compensation is defined as any monetary payment made to a patient attributed to the year the case closed, with the Total Liability Cost being the sum of Defense Costs and compensation. All variables are measured per calendar year except the Risk Management Budget, which is only available for the fiscal year. We allocate half of each year's budget to the corresponding calendar years. The presence of a written request for compensation is determined using an individual chart review of all cases resolved by CRP.
New claims in TN in each calendar year are calculated as the number of pending claims at the end of that calendar year plus the number of claims that were closed during that year minus the number of pending claims at the end of the previous year (
It is important to note that the measured liability outcomes for EHS do not necessarily include information about liability outcomes for individual physicians. Since a hospital system would typically be sued whenever a physician practicing there is sued, it is likely that we do not understate severely the number of cases or claims filed due to adverse medical outcomes. The defense and compensation costs we analyze, however, only capture those expenditures for EHS. Our findings thus reflect only the hospital's experiences with CRP, and we can say little about the experiences of individual physicians.
Statistical analysis
We compare liability outcome measurements for EHS to similar measures in Tennessee for all events occurring between 2005 and 2015 using difference-in-difference analysis with common time effects in each year. We use ordinary least squares to estimate the impact of the CRP reform on liability outcomes. We measure these outcomes in logarithms, so CRP effects should be interpreted as percentage changes in the outcomes. Throughout, we present two-sided 95% confidence intervals (CIs), and we use Stata 18.0 for all statistical analyses. The Supplemental Online Appendix contains additional details about the estimations.
Results
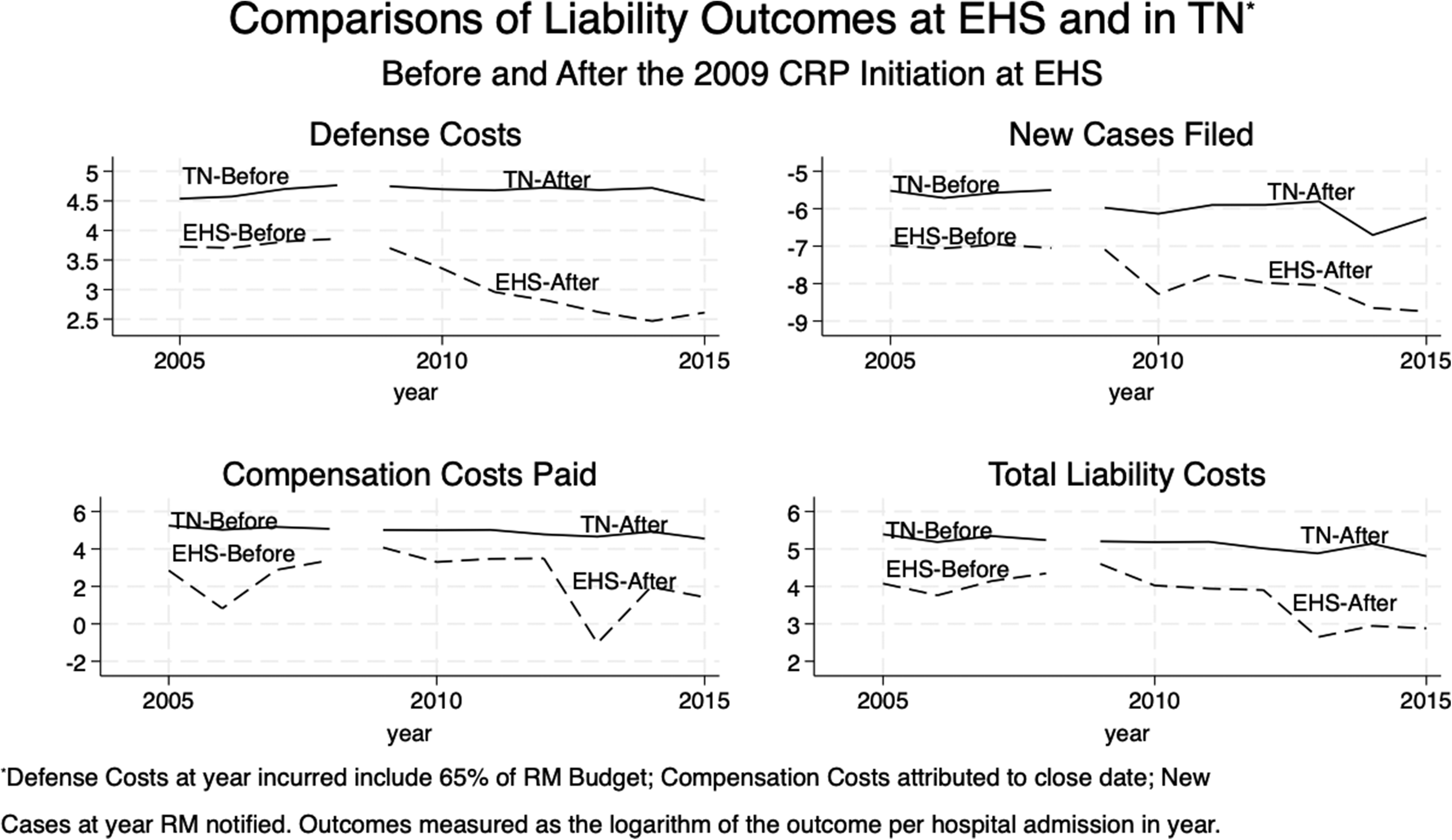
Annual admissions in the pre-CRP years average 823,641 in TN and 20,237 in EHS. After CRP implementation at EHS, annual admissions averaged 797,670 in TN and 21,399 in EHS. Online Appendix Table 1 contains additional summary statistics for EHS and TN by pre- and post-CRP implementation time periods. Figure 1 provides a graphical comparison of the liability outcomes (the logarithm of each dependent variable per hospital admission over the period 2005–2015) separately for EHS and TN. Note that the pre-CRP trends for new claims and defense costs at EHS and TN are quite similar. The pre-trends for compensation and total costs are dissimilar, but these differences are not statistically significant. See Supplemental Appendix Table 2 for the estimates of differences in trends in the pre-CRP period.
File designation.
The regression analyses reported in the Online Appendix Table 2 imply that post-CRP implementation, claims filed in court for EHS decreased by 42% relative to the changes in new written claims for TN (95% CI = −72% to −13%; p = 0.010). Defense Costs at EHS decreased 58% post-CRP compared to TN (95% CI = −79% to −38%; p < 0.001). This estimate includes 65% of the Risk Management Budget with defense costs, but even if 100% of it is attributed to the CRP, EHS's defense costs still would have decreased by 52% compared to TN (95% CI = −72% to −32%; p < 0.001). There is no evidence of a statistically significant change in EHS's compensation per hospital admission. While not statistically significant, total liability costs per hospital admission decreased by 25% compared to TN (95% CI = −81% to +31%; p = 0.34).
Between 2004 and 2015, Risk Management was notified of 274 adverse cases. Of these notifications, 113 occurred prior to the implementation of CRP, and 161 occurred after. 40% of the cases resolved with monetary compensation after the introduction of CRP had only a verbal request for money, with no written request.
Discussion
This is the first study using difference-in-difference (DiD) analysis to demonstrate a statistically significant decrease in defense costs and claims filed as a result of a CRP being implemented in an open and large public hospital system. Sensitivity analysis shows that even when 100% of the Risk Management Budget is included with Defense Costs, there is still a significant decrease in Defense Costs (−52%), suggesting administrative costs of CRP are a minor concern. We find a statistically insignificant impact on compensation at EHS with the CRP. Therefore, given the EHS's wide variation in annual compensation during the pre-CRP period compared to TN, no conclusion can be made regarding the impact of CRP on compensation. We find weak evidence of relative reductions in Total Liability Costs, p = 0.34, (95% CI = −81% to +31%). The 42% decline in Claims Filed at EHS after CRP's implementation, relative to changes in claims made across TN, suggests that many patients find their needs adequately addressed under CRP and are less motivated to pursue litigation.
A study by Kachalia et al. investigated liability outcomes at CRP implementing hospitals and nonimplementing hospitals. 18 However, they did not compare outcomes between the two groups. They relied upon a before-and-after analysis for only those hospitals implementing CRP to measure effects. (For a detailed examination of key methodological issues in Kachalia et al., see LeCraw et al. 19 ). Other studies also found decreased trends in claims and Defense Costs in hospitals that implemented CRP compared to before implementation.3,11,20 Since our study uses a contemporaneous comparison group, it provides more reliable evidence that CRP decreased defense costs and claims filed.
Most studies investigated the impact of CRP on liability outcomes in closed hospital systems, where physicians were employed and insured by the hospital.3,18,20 EHS was an open healthcare system during our study period, where physicians were independent and carried their own liability insurance. This distinction between open and closed hospital systems could be crucial for successfully implementing CRP. In closed systems, liability reforms can be implemented from the top down; but they can only be successful in open health systems if administrators obtain buy-in from their independent physicians. This is undoubtedly difficult to achieve given that as of 2020, 50.1% of physicians nationwide were self-employed and did not work in closed settings. 21 There is huge potential to improve outcomes if CRP can be shown to work in both open and closed settings. To our knowledge, only LeCraw et al. examined how a CRP impacted liability outcomes in an open system, 11 but that study used a before-and-after comparison. This paper extends that analysis by using a DiD analysis to estimate the impact of EHS's CRP on their liability outcomes.
Since CRPs can compensate patients for minor injuries, CRP is especially beneficial to injured patients from a low socioeconomic status. Under DDD, rarely is compensation made for minor injuries due to the high litigation costs for patients’ attorneys. Consequently, such patients suffer relatively large economic hardships arising from medical errors under the status quo.
Previous studies used a before-and-after or a simple interrupted time series research design. They did not control for national and state-level policy changes, trends, or other factors that may impact liability outcomes.3,11,18,20 Our DiD analysis compares changes in liability outcomes at EHS against similar measures for TN from before to after CRP implementation to adjust for such confounders. Examples of changes that occurred during the study period include the steady decline in malpractice claims nationwide, 22 four malpractice reform bills passed by the TN legislature23–26 and the Great Recession. The effects of such factors would be attributed to CRP impacts in simple before-and-after analyses. DiD controls for such factors when assessing whether the advantages of CRPs can be enjoyed without unacceptable increases in liability costs.
Many physicians believe that reports to the National Practitioner Data Bank (NPDB) when compensation is given can cause career damage. 27 However, reporting compensation is only required when there is a written demand for financial compensation. 28 An important finding in this study is the high percentage of strictly verbal requests for compensation at EHS under CRP (40%). While this percentage is only for cases involving the hospital, this pathway for dealing with medical error could allay physicians’ fears of being reported to the NPDB when they provide compensation through a CRP. This finding may encourage buy-in for CRP from physicians.
Many physicians consider a malpractice claim the most stressful experience in their career. 29 While we cover the hospital's experience rather than the physicians’, the finding of quicker resolution of cases and decreased litigation reported in this and previous studies11,20 may reduce the emotional costs physicians associate with malpractice litigation. In a survey of healthcare providers in 56 acute care hospitals, Friedson et al. found a positive association between CANDOR, a form of CRP, and provider satisfaction with their work environment and hospital leadership. 30 Both correlate with decreased burnout symptoms. More study is needed on this topic.
This retrospective study has limitations. The small number of cases involving compensation and the wide variation in injuries across years at EHS results in statistical insignificance when examining compensation and Total Liability Costs. The pre-CRP trends in compensation in Supplemental Appendix Table 2 differ between EHS and TN, unlike the close agreement in pre-CRP trends for Defense Costs and Claims Filed. Such differences, even though statistically insignificant, make the attribution of estimates for compensation from the DiD analysis to CRP effects problematic. Due to data limitations, this analysis cannot control for any differential changes over time between EHS and TN in illness severity or payer base. The DiD analysis, however, does control for any persistent differences over time in the determinants of liability outcomes between EHS and TN.
TN characterizes compensation paid only by the year of close, not by the year of notification of the claim, and to make the outcomes comparable we do likewise for compensation paid at EHS. Classification by notification date would be a more appropriate way to attribute the costs to pre- vs post-implementation when evaluating the CRP's impact on compensation, especially for cases that were open at the time the CRP started. CRP, by closing new and existing cases more quickly, likely causes compensation to be given sooner than would have otherwise occurred under the previous resolution process. This can lead to large and variable compensation payments especially during the first two years under CRP, which wrongly attributes these compensations to cases prior to CRP. Even with this misattribution, however, we do not find a significant increase in compensation. See Appendix Table 3 and Figure 3 for more discussion of this issue.
There are important differences in practice settings and patient characteristics between EHS and TN that could impact comparisons of their liability outcomes. The EHS reports cover only inpatient admissions while the TN reports contain information from all health care providers in the state. The patient mix at EHS became older, more commercial- and self-payer- and less Medicare- and Medicaid-based over time, but no readily available, comparable data is available for TN. While the outcomes reported at EHS are included in the TN liability reports, EHS makes up only a small share (2.5%) of total admissions for the state, which suggests that possible biases due to the overlap of treatment and control groups are small. Additionally, the largest health care system in TN, Vanderbilt University Medical Center (VUMC), did have a CRP in place throughout the study period. The presence of that large system using CRP in the control group should not lead to any appreciable overstatement of EHS’ benefits from the CRP, unless VUMC's effectiveness in utilizing its CPR declined over time. While these difficulties with variable definitions and measurement do complicate causal inference in this study, the fact that the literature contains no other DiD analyses makes the findings of this study the best existing estimates of the impact of CRP implementation on liability outcomes.
Since EHS physicians had the option to use the resolution practice of their malpractice insurance carrier, we can only examine cases that involve the hospital. TN does not separately report aggregate malpractice-related claims occurring at hospitals from other healthcare delivery points; only 63% of all TN claims (72% of all compensation paid) originated in hospitals.12–16 Our comparison group therefore also contains ambulatory surgery centers and other provider locations, so we assume liability outcomes at such sites would not be affected differently by state and national factors compared to hospitals. Unfortunately, there are no data available to examine whether quality improved with the implementation of CRP.
Summary
The results reported here provide the first evidence using a comparison group to demonstrate that CRP can lower defense costs and claims filed in court while not significantly increasing other compensation or total liability costs. We find that 40% of compensations were a result of verbal requests for financial compensation under CRP, and so would not be reportable to the NPDB.
The composite group of existing studies provides evidence that compared to DDD, CRPs present stakeholders with numerous advantages.3,11,18,20 These include a reduction in lawsuits, lower defense costs and time to resolve a case, greater patient satisfaction, and improved quality and safety. Since physicians and hospitals are concerned about the financial impact of CRPs, it is crucial that CRP researchers produce reliable estimates of the financial impact and incidence of malpractice claims to inform the decisions of hospital administrators and other providers.
Accessing research materials
All liability and outcome data obtained from the Erlanger Hospital System came from confidential administrative data and individual health records, and these data cannot be shared. If a researcher does obtain explicit written approval from the Erlanger Health System to have access to all the data used in this analysis, the authors will provide copies of all of the data used in this analysis along with the STATA code for carrying out the analysis. The State of Tennessee's aggregated liability claims data can be obtained through the documents cited in endnote references 12 through 17.
Supplemental Material
sj-docx-1-cri-10.1177_25160435251319859 - Supplemental material for Evidence on improvements in medical liability outcomes after the introduction of a communication-and-resolution program at a hospital in Tennessee
Supplemental material, sj-docx-1-cri-10.1177_25160435251319859 for Evidence on improvements in medical liability outcomes after the introduction of a communication-and-resolution program at a hospital in Tennessee by Florence R LeCraw, Daniel Montanera, Dale Hetzler, Joy P Jackson, Janice C Keys and Thomas A Mroz in Journal of Patient Safety and Risk Management
Supplemental Material
sj-pdf-1-cri-10.1177_25160435251319859 - Supplemental material for Evidence on improvements in medical liability outcomes after the introduction of a communication-and-resolution program at a hospital in Tennessee
Supplemental material, sj-pdf-1-cri-10.1177_25160435251319859 for Evidence on improvements in medical liability outcomes after the introduction of a communication-and-resolution program at a hospital in Tennessee by Florence R LeCraw, Daniel Montanera, Dale Hetzler, Joy P Jackson, Janice C Keys and Thomas A Mroz in Journal of Patient Safety and Risk Management
Footnotes
Declaration of conflicting interests
The views expressed here are the authors’ and not necessarily those of the Federal Reserve Bank of Atlanta or the Federal Reserve System.
Ethical considerations
This is a policy-focused observational manuscript that did not involve human subject research. The study was approved by the EHS institutional review board. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline. This is a retrospective study. All authors outside of the Risk Management Department at EHS were blinded to the characteristics of claimants at EHS.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.