
Abstract
Purpose:
Corneal high-order aberrations due to pterygium have a significant impact on patients’ visual quality. This study aims to assess changes in corneal high-order aberrations following pterygium surgery.
Methods:
This hospital-based prospective study included 51 eyes of 51 patients with primary pterygium who underwent pterygium excision with conjunctival autograft. Corneal topography and ocular high-order aberrations (HOA) were measured using corneal topography and aberrometry scans with a Sirius Scheimpflug-Placido topographer, both preoperatively and 6 weeks postoperatively. These values were derived for both 3 and 5 mm pupillary diameters using Zernike polynomial expansion. The relative risk of residual postoperative aberrations was assessed in relation to increasing pterygium size.
Results:
The mean age of patients enrolled in the study was 40.3 ± 7.4 years. The root mean square value of total HOA significantly decreased at 6 weeks after uneventful pterygium surgery. Excision of pterygium significantly reduced all parameters (coma: 95% CI, p < 0.05; trefoil: 95% CI, p < 0.05; quadrafoil: 95% CI, p < 0.05), with trefoil being the main contributor. Astigmatism values also showed a significant postoperative reduction. In 15.9% of patients, preoperative “with-the-rule astigmatism” changed to postoperative “against-the-rule astigmatism.” A notable increase in the relative risk of residual postoperative HOA was observed when the pterygium length exceeded 4 mm.
Conclusion:
Pterygia are associated with corneal higher-order aberrations, particularly trefoil, which were largely eliminated by surgery. Earlier excision of pterygia reduces the likelihood of significant residual aberrations.
Plain language summary
This study investigated the impact of pterygium (a non-cancerous growth on the cornea) on corneal higher-order aberrations (HOA), which can degrade visual quality, and whether these aberrations improve after pterygium surgery. The study included 51 patients with primary pterygium who underwent surgical excision with conjunctival autograft. Researchers measured corneal topography and HOAs before surgery and six weeks after, using a specialized imaging system.
The results revealed a significant reduction in the total HOA, particularly in trefoil, a type of optical distortion, following surgery. Astigmatism also improved postoperatively, with some patients experiencing a shift from “with-the-rule” astigmatism to “against-the-rule” astigmatism. Additionally, the study found that larger pterygia (over 4 mm in length) were associated with a higher risk of persistent aberrations after surgery.
In conclusion, pterygium leads to corneal higher-order aberrations, especially trefoil, which are largely corrected by surgery. Early surgical intervention is recommended, as it reduces the likelihood of significant residual visual disturbances.
Introduction
A pterygium (plural: pterygia) is a triangular fibrovascular growth of degenerative bulbar conjunctival tissue over the limbus onto the cornea, 1 occurring predominantly in the nasal conjunctiva. 2 Ultraviolet-B radiation2,3 and various fibroangiogenic factors 4 have been implicated as its main etiological factors. Various types of topographic and refractive changes in the cornea can be observed depending on the size of the pterygia, in addition to their common symptoms. 5 The reason for this remains debatable. A possible cause could be the local pooling of tears at the pterygium apex. 6 Such pooling may be indicative of corneal flattening.
Pterygia lead to deterioration of the quality of visual performance not only by causing refractive changes but also by increasing the corneal higher-order aberration. Trefoil has been reported to be the most common high-order aberration among all patients with pterygium.7 –9 Many studies have shown that such high-order aberrations induced by pterygia cannot be corrected by optical aids, and the only definitive method of correction is surgery.10 –12 The possible reason for this might be that high-order aberrations are the result of corneal irregularities and/or imperfections. Previous studies have shown that uneventful excision with conjunctival autograft can significantly reduce most pterygium-induced high-order aberrations.5,9,13,14 Yasar et al. 6 explained that the disappearance of the pooling effect of tears after excision of pterygium results in dissipation of flattening, leading to improvement in high-order aberrations after surgery.
Corneal topographic studies6,15,16 have long been applied to study high-order aberrations induced by pterygium. The information thus obtained is expressed as mathematical functions in the form of Zernike polynomials,17,18 as per the American National Standards Institute (ANSI). 19 The information obtained from such data is valuable for better assessment of the impact of high-order aberrations, as well as for evaluation of the impact of surgery on the quality of vision. Alongside the study of the impact of pterygium length on residual high-order aberrations, the answer to the question of when the pterygia should be removed to minimize residual aberration in the postoperative period can be clarified with certainty.7 –9
Few studies have evaluated the effect of pterygium on corneal high-order aberration and the corresponding changes after surgery. Furthermore, to our knowledge, no other study in Nepal has evaluated such changes based on the lengthwise classification of pterygium. Therefore, we evaluated the variation in corneal high-order aberrations after pterygium surgery and the effect of pterygium length on high-order aberrations.
Materials and methods
Study population
All patients with pterygium who attended the General Outpatient Department, External Ocular Disease, and Cornea Clinic and underwent pterygium surgery at BPKLCOS were included in the study. Patients with recurrent pterygium, a history of anterior segment trauma or surgery, a history of contact lens use, corneal diseases, especially ectasia or corneal opacity, conjunctival diseases or scarring, active conjunctival or corneal infection, chemical injury, Stevens-Johnson syndrome, ocular pemphigoid, other causes of severe dry eyes, and those unwilling to participate in the study were excluded. Patients older than 50 years were also excluded to avoid the possible effect of age on ocular aberrations.
Ophthalmologic examination
Visual acuity testing, followed by refraction and detailed slit-lamp examination, was performed in all cases. Details of the pterygium were recorded, including site (nasal/temporal), involved eye, morphology, and the horizontal length between the nasal limbus and the apex of the pterygium, which was measured using a slit lamp with a slit beam of light (in millimeters). For further analysis, eyes were classified according to pterygium length into four groups: <2, 2–3, 3–4, and > 4 mm.
Measurement of high-order corneal aberrations
Corneal topography and HOA measurements before and after pterygium surgery were performed using the Bon-Sirius corneal topography and aberrometry scan® before surgery and 6 weeks postoperatively by the same examiner. Three images were recorded for each eye across a natural (nondilated) pupil, and the image with the best alignment was selected for analysis. Topographic astigmatism, high-order aberration (HOA), coma, trefoil, quadrafoil, and spherical aberration were observed at pupil diameters of 3 and 5 mm, respectively, and analyzed as RMS values.
Surgical technique
After receiving peribulbar anesthesia, the eye undergoing surgery was prepared by painting with 5% betadine solution and draped using a sterile technique. A universal eye speculum was applied, and surgery was performed under an operating microscope. An incision was made on the superior part of the pterygium at the level of the limbus. The pterygium was separated from the sclera, and the entire pterygium, including the Tenon capsule, was excised with conjunctival scissors at the limbus. The excess Tenon capsule was dissected and removed, and bleeding vessels were cauterized. The head of the pterygium was grasped with toothed forceps and removed using the principle of pterygiorrhexis. The wound bed was then scraped with a hockey stick knife, taking care not to dissect too much of the corneal surface.
The size of the conjunctival defect was measured using Castroviejo calipers, and a conjunctival graft of the same size was harvested from the superior bulbar conjunctiva, including the stem cells at the limbus, after separation from the underlying Tenon capsule. The conjunctival autograft was then placed over the defect and secured with 8-0 Vicryl sutures at the corners. Chloramphenicol ointment was applied, and the eye was padded for 24 h.
Postoperatively, all patients were treated with topical antibiotic drops mixed with steroids (Chloramphenicol 4 mg + Dexamethasone 1 mg + Polymyxin B 5000 IU) four times a day, lubricating eye drops four times a day, and antibiotic ointment. Topical steroids were gradually tapered over 4–6 weeks and then discontinued.
Statistical analysis
Data were entered into SPSS version 25 and analyzed using appropriate statistical tests, including the paired t-test, Wilcoxon signed-rank test, Pearson bivariate correlation test, and Spearman correlation test, wherever applicable. For the analysis of preoperative and postoperative best-corrected visual acuity, astigmatism, total high-order aberration, coma, trefoil, quadrafoil, and spherical aberration, the Wilcoxon signed-rank test and Spearman correlation test were applied when data were skewed. A p value less than 0.05 was considered statistically significant.
Results
The mean age of the patients was 40.3 ± 7.4 years. The range was between 27 and 50 years of age. Of the total of 51 patients, 38 (74.5%) were women and 13 (24.5%) were men. 33.3% (17) of the patients had pterygium in the right eye, 39.2% (20) had the disease in the left eye, and the remaining 27.5% (14) had bilateral disease. During the operation, the mean length of the pterygium was found to be 2.02 ± 0.73 mm. 58.82% (30) patients presented with OPD with pterygium of length 2–3 mm, 21.56% (11) had pterygium of length less than 2 mm, 15.68% (8) presented with pterygium of 3–4 mm and the rest 3.92% (2) had pterygium which was more than 4 mm in length.
Thirty-two patients (62.7%) had “with the rule of astigmatism,” 12 patients (23.5%) had “against-the-rule of astigmatism,” and the rest 13.7% had oblique astigmatism at the time of presentation. At 6 weeks after pterygium surgery, 27 patients (52.9%) had “with the rule of astigmatism,” 17 patients (33.3%) had “against-the-rule of astigmatism,” and the rest 13.7% had oblique astigmatism. Five patients (9.8%) who had preoperatively changed to “against-the-rule of astigmatism” postoperatively changed to “against-the-rule of astigmatism.”
There was a significant decrease in postoperative astigmatism values in both 3 and 5 mm pupil diameters in all categories of pterygium length of pterygium (p < 0.05 for both 3 and 5 mm pupil diameters). Among them, the values were statistically significant in the pterygium of length less than 2 mm (p = 0.041, 0.023 for the pupil diameter of 3 and 5 mm respectively), 2–3 mm (p = 0.004, 0.003 for pupil diameter of 3 and 5 mm respectively) and 3–4 mm (p = 0.036, 0.017 for the pupil diameter of 3 and 5 mm respectively; Table 1).
Statistical analysis of change in astigmatism after pterygium surgery at a pupil diameter of 3 and 5 mm (N = 51).
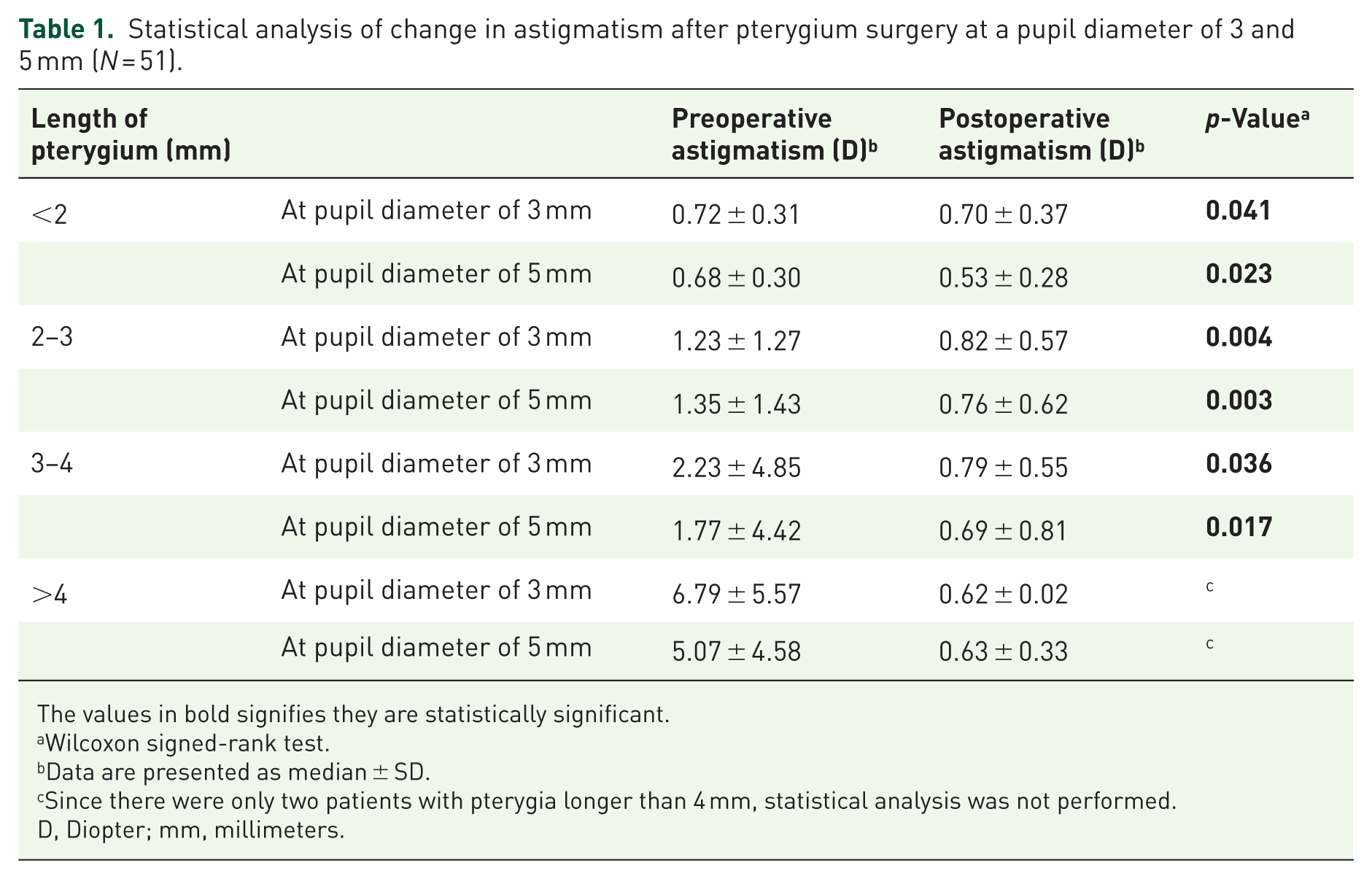
The values in bold signifies they are statistically significant.
Wilcoxon signed-rank test.
Data are presented as median ± SD.
Since there were only two patients with pterygia longer than 4 mm, statistical analysis was not performed.
D, Diopter; mm, millimeters.
In general, there was an increase in postoperative Keratometric mean (Km) values at the central corneal diameter of 3 and 5 mm in all categories of pterygium length. Among them, the values were statistically significant in the pterygium with length 2–3 mm (p = 0.024 for the central corneal diameter of 5 mm only), and the rest were statistically insignificant (Table 2).
Change in Km values after pterygium surgery in the central corneal diameter of 3 and 5 mm based on the length of the pterygium (N = 51).

The values in bold signifies they are statistically significant.
Paired t test.
Data are presented as mean ± SD.
Since there were only two patients with pterygia longer than 4 mm, statistical analysis was not performed.
D, Diopter; Km, Keratometric mean value; mm, millimetres.
There was a decrease in postoperative HOA at both pupil diameters of 3 and 5 mm in all categories of the length of the pterygium. Among them, the values were statistically significant in the pterygium with a length of 2–3 mm (p < 0.0001 for the diameter of the pupil of 3 and 5 mm, both) and 3–4 mm (p = 0.018, 0.012 for the diameter of the pupil of 3 and 5 mm, respectively; Table 3).
Statistical analysis of the change in HOA after pterygium surgery at a pupil diameter of 3 and 5 mm based on the length of the pterygium (N = 51).
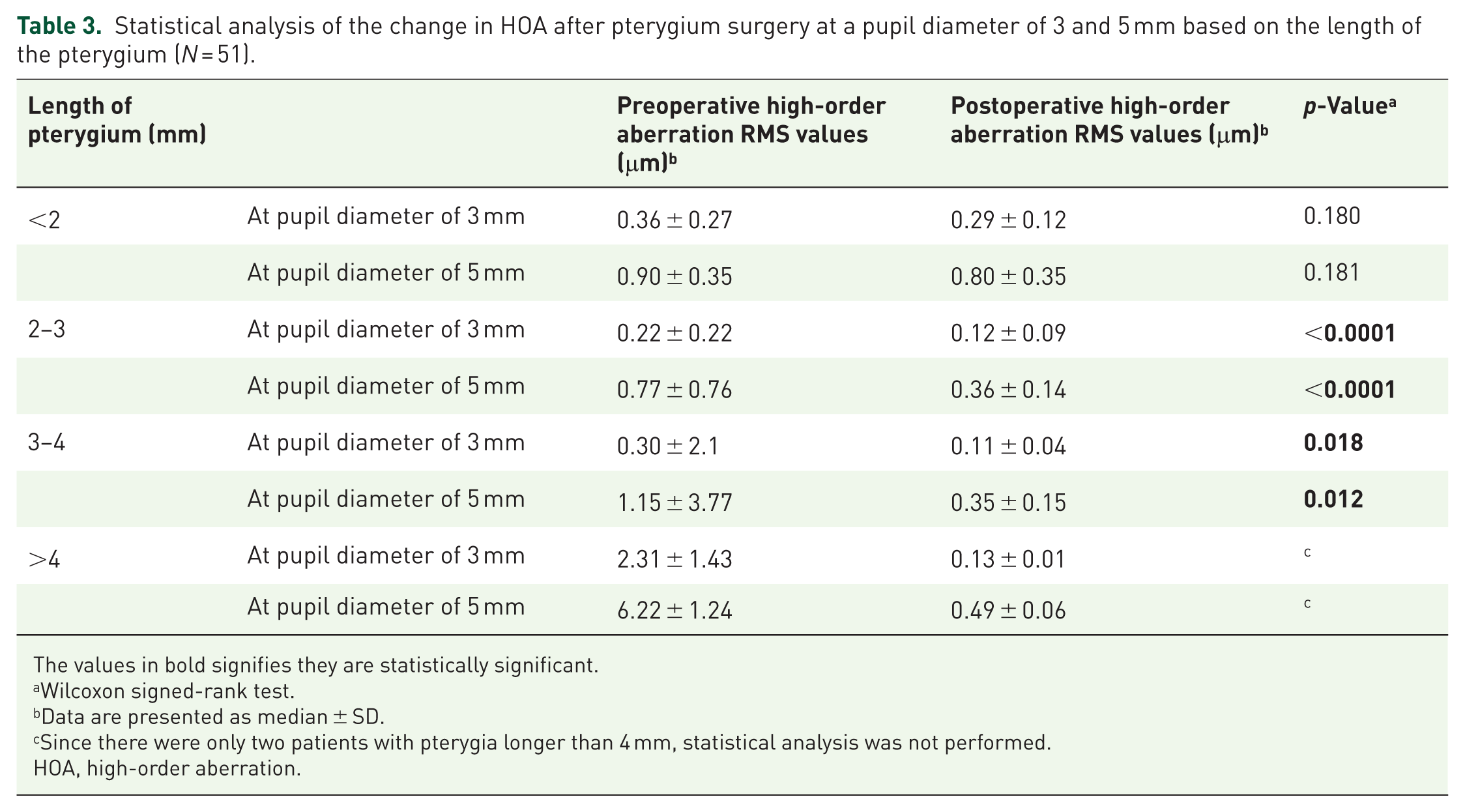
The values in bold signifies they are statistically significant.
Wilcoxon signed-rank test.
Data are presented as median ± SD.
Since there were only two patients with pterygia longer than 4 mm, statistical analysis was not performed.
HOA, high-order aberration.
When the analysis for the types of HOAs was performed irrespective of the length of pterygia, there was a significant decrease in postoperative value for Coma, Trefoil, and Quadrafoil in both the diameters of the pupil of 3 and 5 mm (Table 4).
Statistical analysis of change in coma, trefoil, and quadrafoil after pterygium surgery for pupil diameter of 3 and 5 mm (irrespective of the size of pterygia) (N = 51).

The values in bold signifies they are statistically significant.
Wilcoxon signed-rank test.
Data are presented as median ± SD.
μm, micron; RMS, root mean square.
The risk of postoperative residual higher-order total RMS was found to increase with the size of the pterygium twofold when the length of the pterygium increases to 4 mm. There was a marked increase in this risk (5.5 times) when the length of pterygium increased to more than 4 mm. Likewise, the likelihood of high values of postoperative HOA increased with pterygium size (likelihood ratio = 1.95; Table 5).
Risk estimate between length of pterygium and postoperative residual HOA.

Likelihood ratio of total data: 1.95.
HOA, High-order aberration.
Discussion
The cornea is the major part of the refractive surface of the eye. Pterygium, the fibrovascular growth on the cornea, has gained more attention due to its impact on visual performance. 7 In addition to its cosmetic aspect and the visual impairment caused by the invasion of the visual axis, pterygium induces focal corneal flattening and irregularities on the corneal surface, leading to astigmatism and high-order aberrations that contribute to the production of glare and halos. 5 Oldenburg et al. 20 hypothesized that the observed corneal flattening and topographic changes are due to the pooling of tears.
Many studies have revealed that uneventful surgical excision could improve vision and pterygium-induced corneal topographic changes in the postoperative period. The aim of this research was to study changes in pterygium-induced corneal high-order aberration.
We compared preoperative topographic astigmatism values, preoperative keratometric values, and HOAs with postoperative values after 6 weeks of pterygium surgery.
The average preoperative length of the pterygium among study subjects was 2.02 ± 0.73 mm, ranging from 2 to 4 mm. Most of the patients (58.82%) had a pterygium length ranging from 2 to 3 mm before surgery. Similarly to our findings, Mohammad-Salih et al. found the average length of pterygium to be 2.0 ± 1.2 mm (range 0.25–6.50 mm). 21 In contrast, Gumus et al. 7 found the average length of pterygium to be 3.2 ± 1.1 mm (range 1.8–6 mm).
In the preoperative period, “with-the-rule astigmatism” was common (62.7%), followed by “against-the-rule astigmatism” (23.5%) and oblique astigmatism (13.7%). These values changed postoperatively, resulting in “with-the-rule astigmatism” (52.9%), “against-the-rule astigmatism” (33.3%), with oblique astigmatism remaining constant. With-the-rule astigmatism usually occurs due to mechanical pull, causing localized flattening of the horizontal meridian of the cornea up to the leading apex of the pterygium. 22 Therefore, in our study, the preoperative “with-the-rule astigmatism” changed to postoperative “against-the-rule astigmatism.” Similar results were obtained in studies by Oh et al. 23 and Aziz et al. 24
In our study, there was a significant decrease in astigmatism in both the 3 and 5 mm pupil diameters after pterygium surgery (p < 0.05 for both the 3 and 5 mm pupil diameters). The decrease in astigmatism at both the 3 and 5 mm pupil diameters was significant for all categories of pterygium length, except for the length of pterygium greater than 4 mm. Similar results were obtained by Aziz et al., 24 Bahar et al., 25 Maheshwari et al., 26 and Yaycioglu et al. 27 The possible cause of such astigmatism is corneal flattening produced by pooling of tears at the apex of the pterygium and mechanical traction exerted by the pterygium.6,20,28
Keratometric readings have been shown to increase after pterygium surgery in most studies. Excision of the pterygium resulted in corneal steepening, as the mean keratometric power of the anterior surface changed significantly in a study by Omar et al. 29 Similar results were obtained in the work of Yilmaz et al. 30 and Razmjoo et al. 31 Saleem et al. found a statistically significant increase in the K1 and K2 values (p < 0.05) following pterygium surgery. 13 Similar findings were noted in studies done by Errais et al., 15 Kujur et al., 1 and Oh et al. 23 Kujur et al. have stated that the postoperative increase in keratometric values is due to the dissipation of corneal flattening, which makes the cornea steeper, after removal of the pterygium. 1 According to the studies mentioned above, our study showed a statistically significant increase in postoperative mean keratometric values for both the central corneal diameters of 3 and 5 mm (p < 0.05 for both). When the mean keratometric values based on the length of the pterygium were compared, there was a general increase in postoperative values, but the data were statistically significant for the increase in postoperative Km values at the central corneal diameter of 5 mm for the pterygium length of 2–3 mm only (p = 0.024).
Our study revealed a statistically significant decrease in postoperative HOA at the diameter of the pupil of 3 and 5 mm (p < 0.0001 for both pupil diameters). There was an overall decrease in postoperative HOA when the comparison was made based on the length of the pterygium. However, such a decrease was statistically significant for pterygium lengths of 2–3 and 3–4 mm for both the 3 and 5 mm pupil diameters (p < 0.05).
Similarly, at both 3 and 5 mm pupil diameters, we found that the median value of preoperative trefoil was the highest. Therefore, our study showed that trefoil is the major contributor to high-order aberration in patients with pterygium.
Limited information is available in the literature on changes in high-order aberration with the development of pterygium and the effect of pterygium surgery on these aberrations. We believe this is the first study in Nepal to have studied changes in high-order aberration after pterygium surgery based on pterygium length.
Gumus et al., 5 in their prospective study over 1 year, found that there was a statistically significant decrease in total HOA at 3 and 12 months after surgery. They found that although total coma and trefoil decreased significantly in the early postoperative period (3 months), the total quadrafoil and spherical aberration RMS values did not reveal a statistically significant decrease at 3 months. However, in the late postoperative period (12 months), all RMS values except total spherical aberration were found to decrease after pterygium surgery. They concluded that corneal stability is not achieved in the early postoperative period, and changes continue even after 1 year. However, we could not study long-term stability due to our short follow-up period of 6 weeks. Future studies with a larger sample size and longer follow-up durations could help confirm these findings.
In a similar study by Ozgurhan et al., a significant reduction was found in total HOA, coma, and trefoil values, but not in spherical aberration at 3 and 12 months postoperatively compared to preoperative values. 14 Pesudovs et al. 9 also found that eyes with pterygium had increased higher-order wavefront aberrations for all Zernike orders and modes tested, with trefoil accounting for the majority of the wavefront error. They emphasized that surgical excision eliminated most, but not all, of the induced higher-order aberrations. Their findings were consistent with our study.
In the literature, there have been reports of significant visual problems due to residual irregular astigmatism following pterygium surgery.32,33 Therefore, it seems imperative to assess whether we could predict residual high-order aberrations postoperatively based on pterygium length. This might provide a guideline for surgery concerning the optimal length of the pterygium for good visual quality. We estimate the risk ratio between the length of the pterygium and residual postoperative HOA. The relative risk seems to increase with each millimeter increase in pterygium length, with the highest risk observed for pterygium lengths greater than 4 mm. Similar results were found in the study by Pesudovs et al., 9 where they reported that the risk of residual HOA increases markedly with increasing pterygium length.
Pesudovs et al. 9 have suggested that excision of pterygium when its size is less than 3 mm will result in a better outcome in terms of residual high-order aberrations. Therefore, they recommend 3 mm as the optimal size for surgical intervention. 9 Our study showed that earlier excision of pterygium reduces the likelihood of significant residual HOA (likelihood ratio = 1.95). The risk of residual HOA after surgery is remarkably higher (RR = 5.5) when the length of the pterygium is >4 mm. In contrast, residual HOA is less likely when surgery is performed for pterygium lengths <4 mm. Therefore, we encourage surgeons to consider surgery before the pterygium reaches 4 mm in length, thereby reducing residual HOA and improving visual quality. In addition, patients should be informed about postoperative visual quality according to the length of the pterygium at the time of presentation. This has also been supported by a study done by Ucar et al. 33
The authors acknowledge that the sample size of our study was 51 patients, which is small. In addition, the frequencies of each group according to pterygium length were unequal, with the lowest frequency (N = 2) in the category of pterygium length >4 mm. This very low number of patients with pterygium length >4 mm made statistical analysis of this category impossible. Similarly, postoperative results were evaluated with a short follow-up period (6 weeks), which could have influenced our results.
Conclusion
Our study concludes the importance of evaluating corneal topographic parameters, especially high-order aberrations, in patients with pterygium. Pterygia are associated with corneal aberrations, particularly trefoil, which were largely eliminated by surgery. Our study shows a significant reduction in astigmatism and high-order aberrations after pterygium surgery, which can affect the quality of vision. There is a strong correlation between preoperative corneal topographic and aberrometry parameters and pterygium length, suggesting that these values can be important indicators for pterygium surgery.
This study emphasizes the need for appropriately timed surgery in primary pterygium cases to minimize residual high-order aberrations and improve postoperative outcomes related to visual quality. We recommend that pterygium surgery should not be delayed until the pterygium length exceeds 4 mm, and patients should be informed about the prognosis based on the pterygium’s size at the time of presentation.