
Abstract
Background/Objectives:
To evaluate the effect of macular status and fixation, as determined by chord alpha, on refractive outcomes following combined phacovitrectomy for retinal detachment. Although an optical biometer can be used to calculate the required dioptric power of the intraocular lens, loss of central fixation can introduce errors into the biometric parameters.
Design:
Retrospective single-center observational study.
Methods:
Patients with retinal detachment and cataract who underwent combined phacoemulsification and vitrectomy following swept-source optical coherence tomography-based biometry (ZEISS IOLMaster 700) were included, and their preoperative macular status, chord-alpha length, and resulting refractive error at the final follow-up appointment were recorded.
Results:
A total of 305 eyes were evaluated, of which 150 had macular detachment. There was a statistically significantly higher rate of refractive error in eyes with macular detachment compared to eyes without (p < 0.001). Absolute refractive prediction error of more than 1 diopter was found in 31% of eyes with detached maculae, compared to 12% of eyes without macular involvement. Eyes with a detached macula showed a significantly longer chord alpha (right eye: p = 0.01; left eye: p < 0.0001), and linear regression analysis revealed that a longer chord alpha was associated with a myopic refractive error. The presence of other factors that also correlated with refractive error underscores the multifactorial pathogenesis of refractive prediction error.
Conclusions:
Compared to non-macular involvement, macular detachment led to worse refractive outcomes in combined phacovitrectomy, and chord alpha, as a marker for central fixation, might serve as an explanation. Further research is needed to determine whether combined phacoemulsification and vitrectomy should be performed in patients with macular detachment.
Plain language summary
Combined phacovitrectomy is a widely used procedure for retinal detachment, avoiding the need for additional surgeries and associated complications. However, macular involvement with central fixation loss alters biometric data for IOL power calculation. This study highlights that refractive outcomes may be significantly worse in such cases, with postoperative errors potentially explained by chord alpha, a measure of central fixation. These findings suggest that while the advantages of combined phacovitrectomy are compelling, future research should evaluate its suitability for patients with macular detachment, given the risk of refractive errors exceeding 1 diopter.
Introduction
Retinal detachment is an increasingly common disease that is most commonly treated with pars plana vitrectomy. 1 This type of surgery can be combined with cataract extraction and intraocular lens implantation in combined phacovitrectomy for phakic patients. Thus, the refractive power of the intraocular lens must be calculated prior to surgery. Overall, combined phacovitrectomy might be associated with a higher refractive prediction error than standard cataract surgery alone,2 –4 but has several advantages, including shorter visual rehabilitation time, prevention of future secondary surgery, 5 clearer visualization during surgery, 6 and a favorable cost-benefit ratio. 7
Following retinal detachment surgery, refractive errors can lead to further complications such as anisometropia and patient dissatisfaction. Therefore, it is crucial to identify the factors that may contribute to refractive error to counsel the patient and set expectations appropriately before the procedure. 7 One such factor is loss of central fixation, which can occur in macular disease such as macular degeneration or retinal detachment with macular involvement. This may lead to errors in intraocular lens power calculations 8 and inaccurate anatomical measurements of the eye, such as axial length and keratometry, when using a swept-source optical coherence tomography (SS-OCT)-based optical biometer. 9
The stability of fixation during optical biometry can be evaluated by measuring the first Purkinje reflex, which is quantified by the swept-source OCT-based biometer. 10 A shift in the first Purkinje reflex suggests a deviation from central fixation toward a coaxial fixation point. 11 This reflex is used in eye-tracking software to determine gaze position, and it is recorded while the subject fixes their gaze on a light source in the biometer. 12 In biometry, the Purkinje reflex is recorded while the subject fixes their gaze on a light source in the biometer, and it is correlated with anatomical landmarks such as the center of the circle formed by the limbus, also known as chord alpha. If fixation on the light source is not possible or if it is paracentral, the Purkinje reflex will be altered in relation to the anatomical landmarks.
Therefore, the primary objective of this retrospective analysis was to evaluate the influence of macular status and fixation stability, as determined by chord alpha during biometry, on refractive outcomes following combined phacovitrectomy for retinal detachment.
Methods
Patient selection and study design
This is a single-center retrospective study of 305 eyes of 302 individual patients. The inclusion criteria for the study were a diagnosis of retinal detachment in combination with cataract treated by combined phacovitrectomy with intraocular lens (IOL) implantation in one surgical procedure between January 2016 and January 2024. All surgeries were performed by experienced surgeons. The study was approved by the local ethics committee of the University of Ulm and conducted in accordance with the tenets of the Declaration of Helsinki. The exclusion criteria were any missing preoperative or postoperative data necessary for data analysis in this study. In this retrospective study of real-world data, surgical complications and media opacities were not excluded. For retrospective group allocation, when available, a macular cube OCT was used. Otherwise, we used a combination of the macular SS-OCT from the biometer and the surgeon’s documentation with a correlation to the visual acuity.
Clinical follow-up
Prior to undergoing surgery, all patients underwent a comprehensive ophthalmic examination, including slit-lamp biomicroscopy and dilated pupil fundoscopy. Once the diagnoses of cataract and retinal detachment were confirmed, a decision was made to proceed with a combined phacovitrectomy. The calculation of the intraocular lens power estimation was conducted using a swept-source OCT-based biometer (IOLMaster 700, ZEISS Meditec, Oberkochen, Germany). In the event of uncertainty regarding the axial length measurement, an ultrasound biometry was conducted to verify the accuracy of the axial length measurement prior to surgical intervention. The resulting objective refraction from the autorefractor was recorded without cycloplegia on the last day of follow-up, which occurred between 8 and 12 weeks after surgery.
Surgical technique
Four experienced vitreoretinal surgeons performed standard microincisional cataract surgery involving phacoemulsification and either 23- or 25-gauge vitrectomy under either retrobulbar or general anesthesia. The surgeons then implanted one of five different IOLs into the capsular bag according to their preference. The IOLs used in this study were the AcrySof IQ SN60WF (Alcon, Fort Worth, Texas, USA), the CT Asphina 409MP (Carl Zeiss Meditec), the TECNIS monofocal 1-piece IOL PCB00, and the monofocal 3-piece IOLs ZA9003 and Sensar AR40 (Johnson & Johnson Vision, Jacksonville, Florida, USA).
Data analysis
The XML data were extracted from the IOLMaster using the Forum Viewer (version 4.2.1.66, Zeiss Meditec). The biometric data were extracted from the XML files using a custom Python script (Python 3.12 in PyCharm IDE 2023.3.2, JetBrains, Praha, Czech Republic, all programming by C.M.W.) with the following libraries: CSV, Regex, Pandas, and NumPy. The script automatically selected data on the surgical side, axial length, anterior chamber depth, flat and steep corneal radii, and x and y coordinates of chord alpha (the first Purkinje reflex in relation to the center of the circle described by the limbus, fpx, and fpy). In addition, diagnosis, postoperative refraction, type and power of IOL implanted, age, and biological sex were manually extracted from the electronic medical records. The calculations were based on the Haigis formula, which was rearranged and adapted in a Python script for batch data processing. The target refraction was defined as the refractive prediction that the Haigis formula would make for the type and power of the IOL implanted in the patient’s eye. 13 Since this definition of the target refraction was neither recorded during surgery nor extractable from the biometer’s raw data, it was back-calculated using the dioptric power of the implanted IOL and the biometric data extracted from the biometer, using the following method, which reflects a back calculation of the commercially available Haigis formula.
First, the optical anterior chamber (Formula 1) was calculated according to the Haigis formula using the specific a-constants of the implanted IOL.
Simulated corneal keratometry (Formula 2) values were calculated using the IOL Master’s specific corneal index (1.332) and mean radius.

To back calculate the target refraction backward from the dioptric power of the implanted IOL, the anterior chamber depth, simulated keratometry, and optical anterior chamber depth, the Haigis formula was rearranged for target refraction (Formula 3).

The refractive prediction error (Formula 4) was calculated by subtracting the target refraction from the postoperative refractive spherical equivalent as measured by the autorefractometer (ARK-1s, NIDEK, Aichi, Japan), and the absolute value of the refractive prediction error was presented as the absolute prediction error.

To analyze the deviation of foveal fixation from the anatomical center, we used the difference in x and y coordinates between the first Purkinje reflex and the center of the circle described by the limbus (fpx and fpy, chord alpha). We then applied the Pythagorean theorem (Formula 5) to find the length of the vectorial sum of the two right-angled triangle vectors, with the start and end points defined by (0, 0) and (fpx, fpy).

Statistical analysis
All computations and data collection were performed in Python 3.12 in the PyCharm IDE 2023.3.2 using the following libraries: csv, regex, pandas, and numpy. Graphs were plotted using either matplotlib.pyplot v3.5.3 or GraphPad PRISM 9 (GraphPad Software, Inc., San Diego, CA, USA). A t-test was performed with GraphPad PRISM 9 to compare the different groups. For categorical comparisons, the Pearson chi-squared test was calculated using SPSS 28 (IBM, Armonk, NY, USA). An alpha error of 0.05 was considered statistically significant.
Results
Baseline characteristics
This is a single-center retrospective study of 305 eyes of 302 patients. Group selection was based on macular attachment status. Of the eyes examined, 150 had macular detachment and 155 did not. The mean age of the patients was 63 ± 8 years, and 111 patients were biologically female. The mean implanted IOL power was 19.2 ± 3.5 diopter. Patients with macular detachment had significantly worse baseline visual acuity (p < 0.0001) and significantly higher chord-alpha length (p < 0.0001). All other baseline factors were not statistically significantly different, and the groups were evenly distributed (see Table 1). Regarding influential factors, preoperative vitreous opacities (in particular vitreous hemorrhage) consisted of two cases (1.3%) in the macula-on group and one case (0.7%) in the macula-off group.
Comparison of baseline characteristics between the two groups of patients.

IOL, intraocular lens.
Macular status and refractive outcome
The proportion of refractive errors was found to be statistically significantly higher in eyes with macular detachment than in those without (p < 0.001, Pearson’s chi-squared test). In phacovitrectomy, for cases without macular detachment, 12% of patients had an absolute refractive error greater than 1 diopter, compared to 31% in macular detachment cases (Figure 1).

Stacked histograms are shown to depict the absolute refractive error from target refraction for patients with attached and detached macular regions.
Visual fixation as estimated by chord-alpha length
In the field of biometry, the Purkinje reflex is recorded while the subject fixes their gaze on a light source in the biometer and is then correlated with anatomical landmarks. Changes in the Purkinje reflex in response to visual fixation are commonly employed in eye tracking. The chord alpha represents the relative position of the first Purkinje image in relation to the center of the cornea (Figure 2). The chord alpha coordinates for each laterality can be plotted as a scatter plot using Cartesian coordinates (Figure 3(a) and (c)). As anticipated, patients with a detached macula exhibited a significantly larger chord alpha (right t-test: p = 0.01, left t-test: p < 0.0001) (Figure 3(b) and (d)). The plots and confidence ellipses also indicate a higher degree of scatter in the values observed in patients with a detached macula.

Two photographs were taken by the biometer during the biometric examination. The red arrows indicate the approximate center of the circle around the limbus, while the green arrows indicate the center of the Purkinje reflex. The chord-alpha distance is marked with a blue line. Patient (a) had an attached macula, good fixation, and a small chord-alpha distance. The patient in (b) had a detached macula and showed upward and medial gaze during the biometry examination, likely due to loss of central fixation with a long chord alpha.

The biometer obtained the chord alpha (first Purkinje reflex in relation to the limbal circle as an anatomical landmark) for the right (a) and left (c) eye in relation to the center of a circle described by the limbus (at 0, 0 coordinates). Measurements were divided into two groups: those with an attached macula (green) and those with a detached macula (red). The confidence ellipses enclose all points within 2 standard deviations of the results. While the centers of the ellipses are roughly similar, the points indicate a larger scattering range in eyes with larger refractive errors. In addition, the mean length of chord alpha in millimeters is significantly higher in eyes with detached macula (b, d).
Chord alpha, other biometrical data, and refractive outcome
Linear regressions were calculated to demonstrate the influence of chord alpha, keratometry, axial length, and anterior chamber depth on the refractive outcome, as well as to document the gradient of change between them. According to a slope significantly different from zero, factors that could predict refractive error for all eyes included in the study were chord alpha (p < 0.0001), keratometry (p = 0.007), and anterior chamber depth (p = 0.03). However, axial length (p = 0.6) and power of the implanted IOL (p = 0.2) did not significantly affect the slope, indicating that these factors played a minor role in our study group. The slope between prediction error and chord alpha was −0.61 diopters/mm in all eyes, showing an inverse correlation between refractive prediction error and increasing chord length, resulting in myopic error (Figure 4). These results emphasize the multifactorial pathogenesis of refractive prediction error.
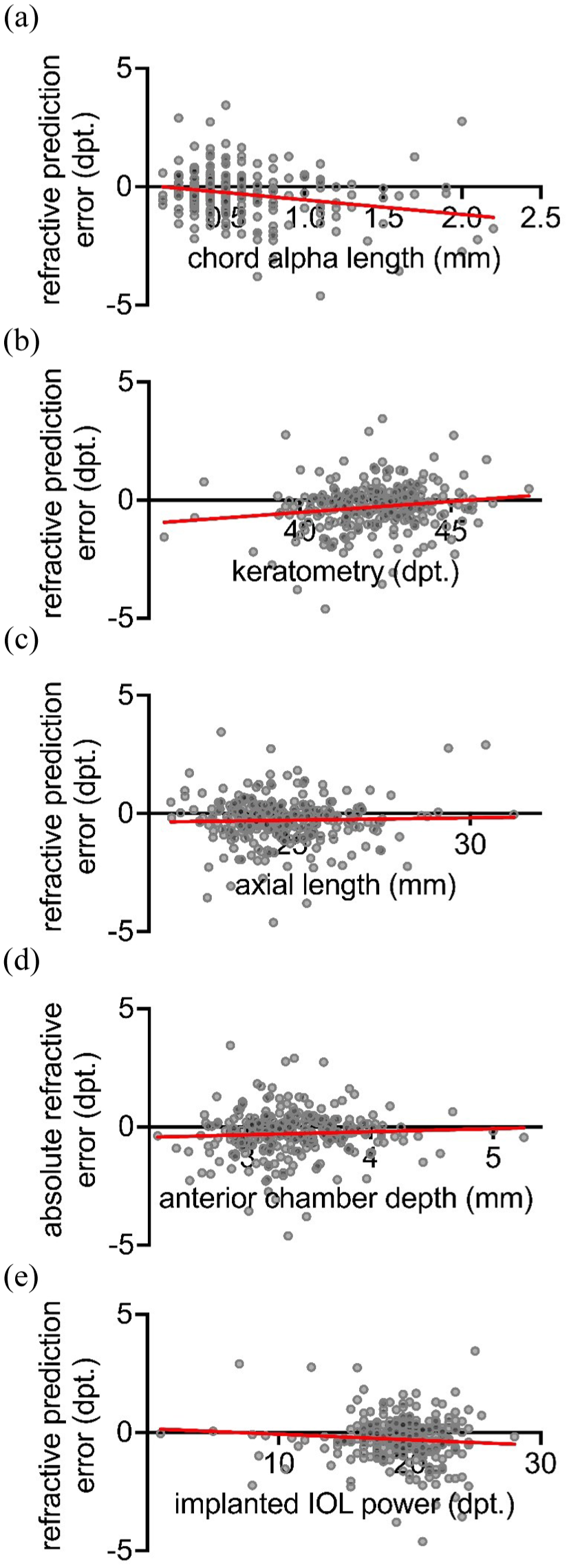
The study examined the correlations between the refractive prediction error and factors that may influence the refractive outcome. The axial length (p = 0.6) and the power of the implanted IOL (p = 0.2) were found to have no significant effect on the slope. ((c) and (e)) However, the slope between refractive prediction error and chord alpha (p < 0.0001), keratometry (p = 0.007), and anterior chamber depth (p = 0.03), respectively, was found to be significantly different from zero. ((a); (b) and (d)) These results highlight the multifactorial pathogenesis of refractive prediction error.
Complications and follow-up
Intra- or postoperative complications can affect the refractive outcome after combined phacovitrectomy. In this context, as intraoperative complications, we observed one posterior capsular rupture (0.6%) and one leaking trocar in the macula-on group. In the macula-off group, we observed four capsular ruptures (2.7%) and two intraoperative bleedings. Postoperative complications occurred in 34 patients (22%) in the macula-on group and in 37 patients (25%) in the macula-off group. A total of 24 re-detachments (16%) were documented in the macula-off group, while 23 (15%) occurred in the macula-on group. Furthermore, other specific complications included 13 cases of elevated intraocular pressure, 1 vitreous hemorrhage, 1 severe sterile intraocular inflammation, 12 proliferative vitreoretinopathies, and 44 macular complications (including, for example, epiretinal membranes, trapped fluid, and cystoid macular edema).
The mean prediction error values were −0.19 ± 0.72 in the macula-on and −0.39 ± 1.17 in the macula-off group. Best-corrected visual acuity was 0.17 ± 0.37 LogMar after surgery for macula-on retinal detachment and 0.54 ± 0.57 LogMar for macula-off.
Discussion
In our study of 305 eyes undergoing combined phacovitrectomy for retinal detachment, we found that patients with macular detachment had a poorer refractive outcome than those without. Although a normal population group was not included in the study, the chord alpha of the retinal detachment patients in the study group was observed to be higher than in previous studies of the general population.14,15 A Cartesian analysis of chord alpha indicated that visual fixation may have resulted in the miscalculation of biometric parameters, such as axial length and keratometry, which in turn resulted in refractive prediction error. Although chord alpha was the primary focus of the evaluation, other factors that also correlated with refractive error highlight the multifactorial nature of refractive prediction error.
There are several possible reasons for deviations in Purkinje images that cannot be determined from our data. One of these is eye movement during the examination, since Purkinje reflexes can be used as a method for eye tracking. 16 Loss of central fixation leading to parafoveal fixation is another possible reason. 9 In our cases with retinal detachment, including macular detachment, this was even more pronounced, possibly due to loss of central fixation in macular detachment or due to cloudy media caused by vitreous hemorrhage. A high individual constitutional deviation in angle alpha may also constitute a deviation in the Purkinje images.
Chord alpha is not a universally validated metric of fixation and has been used in other applications that are not dependent on fixation. In multifocal IOL implantation, chord alpha and chord mu play a role because centration in the optical axis is crucial for this type of IOL, as the central refractive elements must be within the optical axis. A higher chord alpha indicates a deviation of the anatomical axis from the optical axis, suggesting a displaced capsular bag and indicating postoperative multifocal IOL decentration. 17 In this application, however, fixation does not play a role; anatomical differences do. Chord alpha appears to be a more applicable and reliable determinant of postoperative outcomes than chord mu as a surrogate for angle kappa. 18 This may be because chord mu is dependent on intact pupil shape and size, whereas the circle around the corneal limbus for chord alpha is more robust. 18 Future studies should focus on other fixation stability indices that may be more robust than chord alpha, as measured by a biometer. These methods include microperimetry-based bivariate contour ellipse area 19 as well as deep learning-based approaches. 20
Chord alpha has been associated with a worse outcome in multifocal IOLs due to decentration of the IOL off the optical axis. 21 The same is true for corneal refractive surgery for centration of the optical zone, especially in patients with hyperopia. 22 In our study, we use chord alpha to measure fixation by the displacement of the Purkinje reflex toward an anatomical landmark during the biometry exam. Other studies have linked loss of visual fixation during biometry to a worse refractive outcome. In highly myopic patients, low fixation stability in the bivariate contour ellipse areas contributes to higher refractive error. 8 Dense cataracts and loss of fixation due to macular degeneration have been associated with reduced refractive outcomes and failure of the biometry exam. 23 A higher angle alpha has been correlated with a smaller axial length and higher corneal refraction in 74 healthy subjects. 24 The effects observed in the literature are consistent with those observed in this study.
It has been shown that optical axial length measurement varies in different gaze positions, with the forces exerted by the ocular muscles being cited as the cause. 25 In addition, significant refractive error in high myopes has been attributed to preoperative biometric fixation stability, longer axial length, and severe posterior subcapsular opacity. 8 A published study compared centrally and peripherally measured axial lengths obtained with the IOLMaster and Lenstar platforms in healthy adults by taking measurements at 5° intervals. Their measured axial length changed when measurements were taken more peripherally. 26
In our study, we deliberately chose the center of the circle formed by the limbus as the anatomical landmark that would best determine the optical axis using our data. Foveal fixation was approximated by the first Purkinje reflex, as indicated by the chord alpha. 10 Pupillary centration was considered to be less stable, as it varies with pupil size and pupillary disease, 27 and also to be less clinically useful than limbal centration. 28
The power of the IOL must be calculated prior to surgery. Phacovitrectomy is associated with a higher refractive error than standard cataract surgery alone. 29 This error was generally low but was higher in the groups where the vitreoretinal disease resulted in low vision and loss of foveal fixation. Despite the reduced refractive outcome, combining pars plana vitrectomy with cataract surgery still has several advantages, including a shorter visual rehabilitation time, the prevention of future secondary surgery, 5 clearer visualization during surgery, 6 and a favorable cost-benefit ratio. 30 Despite the advantages of combined phacoemulsification and vitrectomy, the question remains whether to perform the procedures simultaneously or sequentially in rhegmatogenous retinal detachment to achieve a better refractive outcome. A recent meta-analysis of 788 eyes across 7 studies found no significant difference in anatomical outcomes between the 2 groups, though the sequentially performed group had slightly better visual and refractive results. 31 The refractive prediction error was slightly myopic in the combined group, as was observed in our study. 31 Our study contributes to the field by focusing specifically on potential causes of refractive prediction errors within the combined surgical approach.
In our study, chord alpha has not been the only predictor of refractive error, and generally, prediction error in refractive outcomes is influenced by multiple factors, 32 including errors in axial length measurement, especially in macula-off retinal detachments. These errors can lead to myopic prediction errors, as the elevated retina is mistakenly marked more anterior than the retinal pigment epithelium. Lower accuracy in axial length measurements is a known issue with ultrasound biometry 33 and the IOL Master 700, accounting for up to 36% of inaccurate IOL predictions.34,35 To address this, we cross-check with the built-in OCT of the biometer and with the axial length of the fellow eye and validate discrepancies using manual A-scan ultrasound. This method resulted in statistically equal axial lengths in both macula-on and macula-off groups. We, of course, acknowledge that other factors influenced our results, but fixation is also a significant contributor to prediction error in our cohort.
The limitations of this study include the multifactorial genesis of refractive error, which leads to many confounding pre-, post-, and intraoperative factors that may have biased the observed results. 36 Another limitation is its retrospective nature, with no sample size calculation or power analysis being performed. As this was a retrospective observational study, the sample size was based on available patient data, which could lead to over- or underpowered analysis. Low postoperative visual acuity in patients with macular detachment may result in an inaccurate determination of postoperative manifest refraction, as poor fixation and unreliable subjective responses can lead to inconsistent measurements, 37 requiring special strategies to determine refraction in patients with low visual acuity. 36 We attempted to omit the refractive error in low vision by using the autorefractometer postoperatively to potentially obtain more reliable refractive results. A preoperative macular cube OCT scan was not available retrospectively in all cases, and it is possible that shallow subretinal fluid under the macula was missed in some cases, resulting in errors in group allocation. Determination of a shorter axial length by mistakenly selecting the detached retina instead of the retinal pigment epithelium as the posterior pole is much less common with the newer optical biometers, but it may still have influenced the results. 38 A limitation of this study is the use of multiple surgeons, a factor that accounts for 4% of the unexplained variance in refractive outcomes according to a large study of 490,987 cases. 32 In addition, while IOL type can influence refractive outcome after vitrectomy, 29 this effect is likely minimal in our cohort. Two IOL types were implanted in only 8 cases, and no difference in refractive prediction error was found among the other 3 IOLs. Further research is needed, and a prospective design would be a possible option to avoid bias.
In conclusion, our large retrospective study provides evidence that refractive outcomes are worse when macular detachment is observed during combined phacovitrectomy. The observed effects may be attributable to the reduction or loss of central fixation during biometry.