
Abstract
Background:
Visual outcome of eyes has often been found to be unsatisfactory even after successful closure of a macular hole, owing to factors like persistent metamorphopsia, scotoma, and reduced sensitivity. Therefore, it becomes critical to evaluate and study the probability and risk of developing a macular hole in the fellow eyes of the patient. This study analyzed the multifocal electroretinographic responses to help predict the risk of macular hole development in fellow eyes.
Methods:
In total 26 fellow eyes, 26 eyes with macular hole, and 50 eyes of 25 controls were enrolled prospectively. The retinal responses from the different rings were compared in the three groups. Optical coherence tomography was done to rule out macular pathology or vitreomacular traction in the fellow eyes.
Results:
All the fellow eyes under observation showed significantly reduced mean amplitudes of retinal response densities, in all rings as compared with controls (31.45 ± 10.38 versus 48.87 ± 7.55, p = 0.00). Three of the fellow eyes developed a macular hole during the 24 months observation period. The prevalence of fellow eye involvement was 11.5%. Relative risk of developing macular hole in the fellow eye ranged from 25 to 75.
Conclusion:
All the fellow eyes, including those that did not develop a macular hole, showed significantly reduced responses on multifocal electroretinogram. This indicates that macular hole may not be a focal disease. It may have widespread functional deficit which is bilateral in nature and suggestive of a degenerative or ischemic insult.
Keywords
Idiopathic macular hole (MH) is not an uncommon abnormality. Its prevalence is reported to be 2 to 3 in 1000.1,2 While it has been found to be unilateral in nature at presentation, the risk of developing a full-thickness MH in the fellow eye has been variedly reported to range from 1.2 to 28%.3–5 The pathogenesis of an idiopathic full-thickness MH has always been of interest to researchers. In 1988, Gass 6 elaborated the clinical stages of an MH based on contact lens slit lamp biomicroscopy. He postulated the cause of development of the MH to be contraction of prefoveal vitreous cortex. It was not until the advent of the optical coherence tomography (OCT) that the exact relationship between the prefoveal vitreous and the retina could be studied in detail in vivo. 7 This confirmed the role of vitreous traction as a causative factor for MH. Vitreomacular traction was described as anomalous posterior vitreous detachment (PVD) accompanied by anatomic distortion of the fovea by an international study group. 8 Although vitreous detachment of the macula is strongly attributed as a factor in the development of MH, it is not the sole factor, as in many instances MH has been seen to occur in eyes without PVD or vitreomacular traction. 9 Researchers have attempted to understand the pathogenesis of the MH better by assessing retinal function. Many studies have shown reduced retinal response densities on electrophysiologic testing in eyes with MH, not only at the fovea but also affecting a wider area around the fovea.10–13 Electrophysiologic testing in the fellow eye has also revealed interesting findings. Various authors have reported retinal responses ranging from normal to reduced, in the fellow eyes which developed MH at a later point.14–16 The purpose of this study was to assess the electrophysiologic responses in the fellow eyes of patients with unilateral idiopathic MHs and to calculate the relative risk of developing an MH in the fellow eye.
Methods
In this prospective study, patients diagnosed with idiopathic unilateral full-thickness MH were recruited from March 2016 to August 2016. In total, 52 eyes of 26 patients were enrolled along with 50 eyes of 25 age-matched normal controls for comparison. Institutional Ethics Committee of Sankara Nethralaya approved the study (514-2016-P). All participants provided informed consent. The study followed the Declaration of Helsinki.
Demographic details like age, sex, systemic illness were collected. All the subjects were made to undergo visual acuity testing, refraction, anterior segment, and detailed fundus examination as a part of comprehensive eye examination. Patients with high refractive errors beyond 6 diopters, glaucoma, corneal opacities, diabetic retinopathy, lamellar MHs, or bilateral MHs were excluded. Visual acuity was recorded in logMAR and Snellen fractions, using the illuminated Snellen LED Vision Chart (ALVC-20; Appasamy Associates, Chennai, India). Pupils were dilated with 1% tropicamide eye drops and fundus examination was carried out with indirect ophthalmoscopy and slit lamp biomicroscopy using 78D lens. OCT was done using Cirrus HD-OCT (Carl Zeiss Meditec, Dublin, CA, USA) for verifying the diagnosis. Retinal morphology and vitreoretinal relationship were examined for all eyes. Electrophysiological responses for both eyes were recorded by multifocal electroretinography system (VERIS compact; Electro-Diagnostic Imaging Inc, Redwood City, CA, USA). It was done monocularly using the Burian-Allen contact lens electrode for active and reference electrodes and gold foil electrode as the ground electrode. The examination was done in accordance with the guidelines prescribed by the International Society for Clinical Electrophysiology of Vision (ISCEV). Amplitude and implicit time of the retinal responses in the foveal, parafoveal, and perifoveal rings were measured. The size of the fixation target was increased while checking for the eye with MH and fixation was monitored.
The subjects were followed up for 24 months. The tests were repeated 6 weeks after the initial visit, after 3 months, and every 6 months thereafter.
Statistical analysis
Statistical analysis was performed using Statistical Package for Social Sciences (SPSS) Version 20.0 software (IBM Corp, Armonk, NY, USA). Normality of the data was checked by performing Kolmogorov–Smirnov test. Wilcoxon signed rank test was performed to compare the pre- and post-surgery parameters. Spearman’s correlation was performed to find the strength and direction of association between two parameters. A p value of <0.05 was considered as significant. The risk of developing MH in the fellow eye was assessed by calculating the relative risk using crosstabs in SPSS.
Results
In total, 52 eyes of 26 patients with unilateral idiopathic MH were included in this study, and 50 eyes of 25 age-matched normal controls were also included for comparison analyses. The mean age of patients with MH was 59.92 ± 9.39 years (range: 40–74 years) and that of controls was 56.73 ± 7.13 years (range: 40–70 years) (p = 0.09). Of the 26 patients, the MH was present in the right eye of 11 (42.3%) patients and left eye of 15 (57.7%). The baseline mean visual acuity of eyes with MH was found to be 0.77 ± 0.34 logMAR (20/120 Snellen acuity) and that of the fellow eyes was 0.17 ± 0.28 logMAR (20/30 Snellen acuity). The OCT test confirmed that none of the fellow eyes and the control eyes had a full-thickness MH, lamellar hole, or a macular cyst at baseline. No vitreomacular traction was seen in any of these eyes at the baseline level. Four eyes showed vitreomacular adhesion which, however, did not progress to traction or hole formation. While 4 of the fellow eyes were found to have PVD at baseline, 18 eyes did not have PVD at baseline.
The implicit time as well as the multifocal electroretinogram (mfERG) amplitudes of all rings was significantly different in eyes with MH as well as the fellow eyes when compared with normal controls. The mean implicit time was 29.09 ± 1.34 ms in controls, 29.87 ± 1.24 ms in MH (p = 0.019), and 29.27 ± 1.43 ms in the fellow eyes (p = 0.58) and the mean amplitudes were 48.87 ± 7.55 in normal eyes, 31.45 ± 10.38 in fellow eyes (p = 0.00), and 26.31 ± 8.81 in eyes with MH (p = 0.00).
Table 1 shows the comparison of mfERG components between normal eyes, fellow eyes, and eyes with MH. Compared with normal eyes, the eyes with MH showed significantly delayed implicit times (except for ring 1) and reduced amplitudes in all rings. In fellow eyes, the implicit time was found to be significantly delayed in rings 5 and 6, whereas amplitude was significantly reduced in all the rings. The comparison of amplitudes of the retinal responses on mfERG is shown in Figure 1.
Comparison of multifocal electroretinogram (mfERG) parameters of normal eyes, fellow eyes, and eyes with macular hole.

Bold values signifies statistically significant p values.
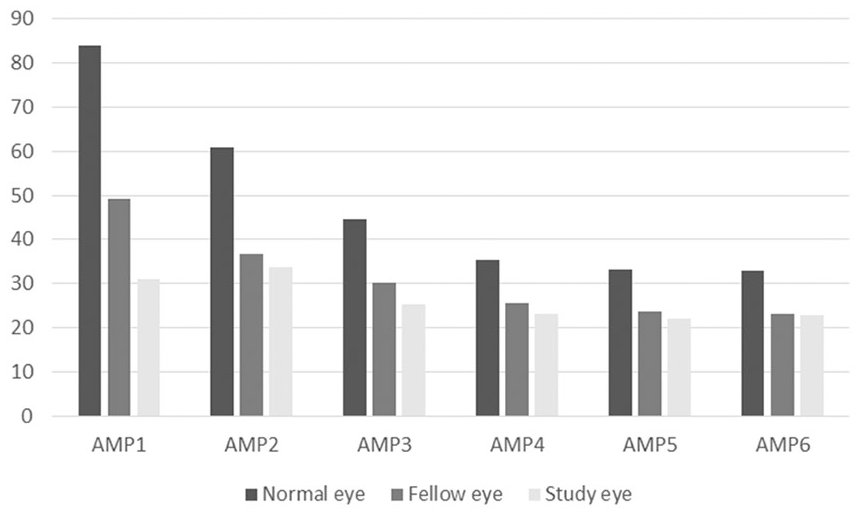
Comparison chart of mean amplitudes of rings 1–6 of multifocal electroretinogram in all normal eyes (n = 50), fellow eyes (n = 26), and eyes with macular hole (n = 26).
Implicit time (latency) is measured in milliseconds, and amplitude is measured in nv/deg2.Analysis was done to find out the correlation between logMAR visual acuity and mfERG components in these eyes. The study revealed that in the eyes with MH, except for ring 1, the amplitudes were significantly correlated with logMAR visual acuity (average r = −0.49, p = 0.012). The ring 1 corresponding to the area of the MH did not show any correlation with visual acuity, whereas in the fellow eyes, amplitudes of all rings except ring 5 were found to significantly correlate with logMAR visual acuity (average r = −0.54, p = 0.005).
These patients were followed up for 24 months; 3 eyes of the 26 fellow eyes developed an MH during this follow-up (11.5%). All the three eyes showed a change in the vitreoretinal relationship during the follow-up but none had any predisposing lesions such as vitreomacular traction, vitreomacular adhesion, or lamellar MH.
The relative risk of developing MH in the fellow eye of patients with unilateral MH was calculated. The normative values of mfERG amplitude and implicit times for all the rings were used to calculate the relative risk. It was observed that if the implicit time is greater than the upper limit [mean + 2 SD (standard deviation)] at rings 1 and 2, it carries a relative risk of 39.1 and 25, respectively. Whereas if the retinal response amplitudes in the fellow eye are lesser than the lower limit (mean − 2 SD) at rings 1–6, then the relative risk of developing an MH was found to be 33.3, 75, 54.5, 39.1, 30, and 36.8, respectively.
Discussion
Visual outcome may be unsatisfactory in the affected eye even after successful closure of an MH owing to factors like persistent metamorphopsia, scotoma, and reduced retinal sensitivity. Therefore, the risk of developing an MH in the fellow eye leading to overall poor vision in the patient is a distinct threat. Although it is generally unilateral at presentation, bilaterality has been reported in 3 to 7% of patients.3,17 The incidence of MH formation in the fellow eyes was found to be 11.5% in this study. Various authors have reported the incidence to be varying widely, from 1.2 to 28%.3–5 Presence of a predisposing lesion, vitreomacular traction, and duration of follow-up has been found to contribute to the incidence of an MH in the fellow eye. In a retrospective study of 49 eyes, Trempe and colleagues 3 found that over a mean period of 47 months, 28% of fellow eyes without a PVD at presentation developed a full-thickness MH compared with 0% of fellow eyes with a PVD at presentation. Whereas Ezra and colleagues, 18 in a prospective 5-year study of a cohort of 114 normal fellow eyes without a PVD, found the risk of developing MH to be 7.5% at 18 months which increased to 15.6% at 5 years. Based on OCT evaluation of change in vitreofoveal relationship, Niwa and colleagues 19 estimated the risk to be 11%.
Tuzson and colleagues 15 used mfERG and found that the ratio of the ring 1 to the outer rings was predictive of the risk of MH development in the fellow eye. If the ratio of R1 to R2 was lower than 2 SD below the mean, the risk was 7.44% and it increased to 23.9% if the ratio of R1 to all the three rings was lower than mean − 2 SD. Of the 40 fellow eyes, 13 eyes which developed MH showed significantly reduced retinal responses in ring 1 and correspondingly reduced ring ratios. The 27 eyes which remained intact did not show significant difference from controls. Chung and colleagues 20 analyzed mfERG responses in eyes with lamellar MH and found that eyes with lower response amplitudes in rings 1 and 2 showed higher morphologic deterioration compared with eyes which maintained higher response levels in the same amplitudes. The current study, however, revealed significantly reduced retinal responses not only in the three eyes which developed an MH, but also in all the fellow eyes.
All the fellow eyes were apparently healthy with no evidence of retinal morphologic changes at the macula. None had any evidence of vitreofoveal traction at baseline. Of the 26 fellow eyes, 6 eyes (23.07%) had vision less than 20/20 on account of cataract. Cataract can cause a reduction in the mfERG amplitudes; however, it is seen to affect only the central ring sparing the rest of the rings. In this study, the mfERG amplitudes in all the fellow eyes showed significant reduction in all the rings which could not be attributed to the presence of cataract. Uniform reduction in the retinal responses on mfERG indicates a more generalized nature of the disease. This highlighted the fact that MH is not a focal, unilateral disorder as it is widely believed to be but it might be affecting a wider area in both the affected and the fellow eyes. It could be safely concluded that the multifocal ERG changes observed in the fellow eyes may actually be an early indication of ischemic or degenerative damage affecting not only the cones but also the inner retinal layer including bipolar and Müller cells. Andréasson and Ghosh 21 found delayed cone implicit time in the full-field ERG in eyes with MH, before surgery. They thus postulated that the entire cone function might be affected in macular pathologies such as MH and cone implicit time was a good predictor of visual outcome. Delayed and reduced 30 Hz flicker with reduced b-wave amplitudes were noted on full-field ERG in MH by others as well. 22 Many disorders such as age-related macular degeneration (AMD) and central serous chorioretinopathy (CSCR) considered to be focal in nature, affecting only the foveal and parafoveal area, have now been found to affect the entire retina. Similarly, recent studies have demonstrated reduced scotopic and photopic b-wave amplitudes as well as delayed a-wave implicit times in the full-field ERG, in patients with drusen, unilateral choroidal neo-vascularization, pigment epithelial detachment, or geographic atrophy and CSCR indicating the involvement of the whole retina in both the eyes.23–25 A higher occurrence of bilateral macular disorders and pathological changes in the morphology of the vitreoretinal interface have also been noted in the fellow eyes over a longer time span.26,27
Interestingly, Kay and colleagues 28 reported increased familial occurrence of MHs in patients with idiopathic MH, as compared with controls. This trend was more common in patients with bilateral MH, a factor which was seen to persist even after disregarding confounding factors such as age and number of relatives suffering from the syndrome. These findings are significant and suggest a familial component to MH.
Our study is limited because of its small sample size. Also, a longer duration of follow-up would is desirable.
Conclusion
While vitreoretinal traction is the commonly accepted cause behind pathogenesis of the formation of an idiopathic MH, the findings of the current study go beyond this lone contributing factor and gives a larger perspective to the disorder by indicating that an MH could in fact be a basic bilateral retinal disorder with multiple pathological and functional alterations occurring in both the eyes, possibly extending beyond the central retina. The study also throws light on the fact that changes in the vitreoretinal relationship may act as a trigger in these fellow eyes resulting in the formation of MH over a period of time.
Footnotes
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.