
Abstract
This study aims to provide an update on infectious scleritis (IS). A comprehensive search was conducted using Google Scholar, Scopus, and PubMed. IS is a rare but critical condition that presents significant diagnostic challenges and often leads to poor visual outcomes. It accounts for approximately 5%–10% of scleritis cases and warrants significant attention due to its delayed diagnosis. Ocular surgery is the primary contributor to IS, accounting for a substantial proportion of cases ranging from 58% to 83%, followed by trauma contributing to approximately 10% of cases. IS can be caused by various microorganisms, including bacteria (86%–87%), fungi (11%–13%), viruses, and parasites. Conjunctival hyperemia is a prevalent manifestation in approximately 98% of IS cases, while scleral necrosis is observed in around 93% of cases. Distinguishing IS from inflammatory scleritis before initiating steroid treatment is crucial. Surgical debridement of infected tissue, accompanied by appropriate topical and systemic antibiotic therapy significantly improves treatment outcomes by removing infected tissue and reducing the infection burden. Early surgical intervention markedly increases the likelihood of preserving the eye globe in severe cases. Risk factors for poor visual outcomes include poor visual acuity at presentation, associated endophthalmitis, keratitis, fungal etiology, and medical therapy without surgical debridement. Early diagnosis of IS is crucial as the disease can progress rapidly and lead to vision loss. While bacterial infections are the most common etiology of IS, the prognosis is particularly poor in cases of fungal IS. Surgical interventions, when combined with appropriate medical treatment, improve outcomes.
Introduction
Scleritis manifests with diverse clinical presentations and is associated with various etiologies, including autoimmune diseases, idiopathic causes, and infections. It is classified into anterior and posterior types based on the location of inflammation relative to the recti muscles. Anterior scleritis is further divided into nodular or diffuse and necrotizing or non-necrotizing subtypes. 1
Infectious scleritis (IS), which accounts for approximately five to ten percent of scleritis cases, is a rare but critical condition requiring urgent attention due to its frequently delayed diagnosis and poor visual outcomes. 1 IS can originate from the sclera itself or may progress from the cornea, episclera, or uvea. Another classification divides IS into exogenous scleritis, which commonly occurs after surgery or trauma or spreads from the adjacent cornea, and endogenous scleritis, which arises more rarely from systemic infections like tuberculosis or syphilis.
IS has been reported most commonly following pterygium surgery, although cataract surgery, glaucoma surgery, vitreoretinal surgery, and conjunctival neoplasm removal also contribute to its development.2–4 Other reported risk factors for IS include trauma,1,5 exposure to mitomycin-C (MMC), irradiation, 2 and immunosuppression.2,6 Clinical manifestations of IS include hyperemia (redness), loss of visual acuity (VA), and pain that worsens at night and intensifies with eye movement.5,7 Purulent exudates, scleral abscesses or pus points, scleral ulcers, and hypopyon are all signs that can be observed during clinical examination. 8 Initially, IS can resemble autoimmune scleritis (AS), leading to the administration of corticosteroids as a treatment for AS. However, delayed recognition and misdiagnosis of IS can result in disease progression and unfavorable visual outcomes. 2
Considering the diagnostic challenges and poorer prognosis of IS compared to AS, this study will review the epidemiology, risk factors, causative microorganisms, and visual outcomes of IS. By providing a better understanding of IS, this research aims to enhance diagnostic and management strategies for this condition.
Methods
A comprehensive search in Google Scholar, Scopus, and Medline was conducted in January 2025 using the following keywords: “Infectious” OR “Infection” OR “Bacterial” OR “Bacterium” OR “Fungal” OR “Fungus” OR “Viral” OR “Virus” OR “Parasitic” OR “Parasite” and “scleritis” in combination. Relevant articles from 1984 to 2025 were collected. We excluded non-English articles, letters, preprint articles, and studies on animals. Papers related to noninfectious scleritis were excluded during the screening process. Original articles, reviews, and case reports were enrolled in the study. Demographic characteristics and sample sizes of the subjects in the studies were not restricted. Then, the articles underwent rapid screening by topic and abstract to select the most relevant articles. The final collection was thoroughly reviewed to explore the epidemiology, risk factors, causative microorganisms, and visual outcomes of IS. Figure 1 illustrates the step-by-step screening and selection process. No informed consent or institutional review board approval was necessary, given the nature of this study as a review.
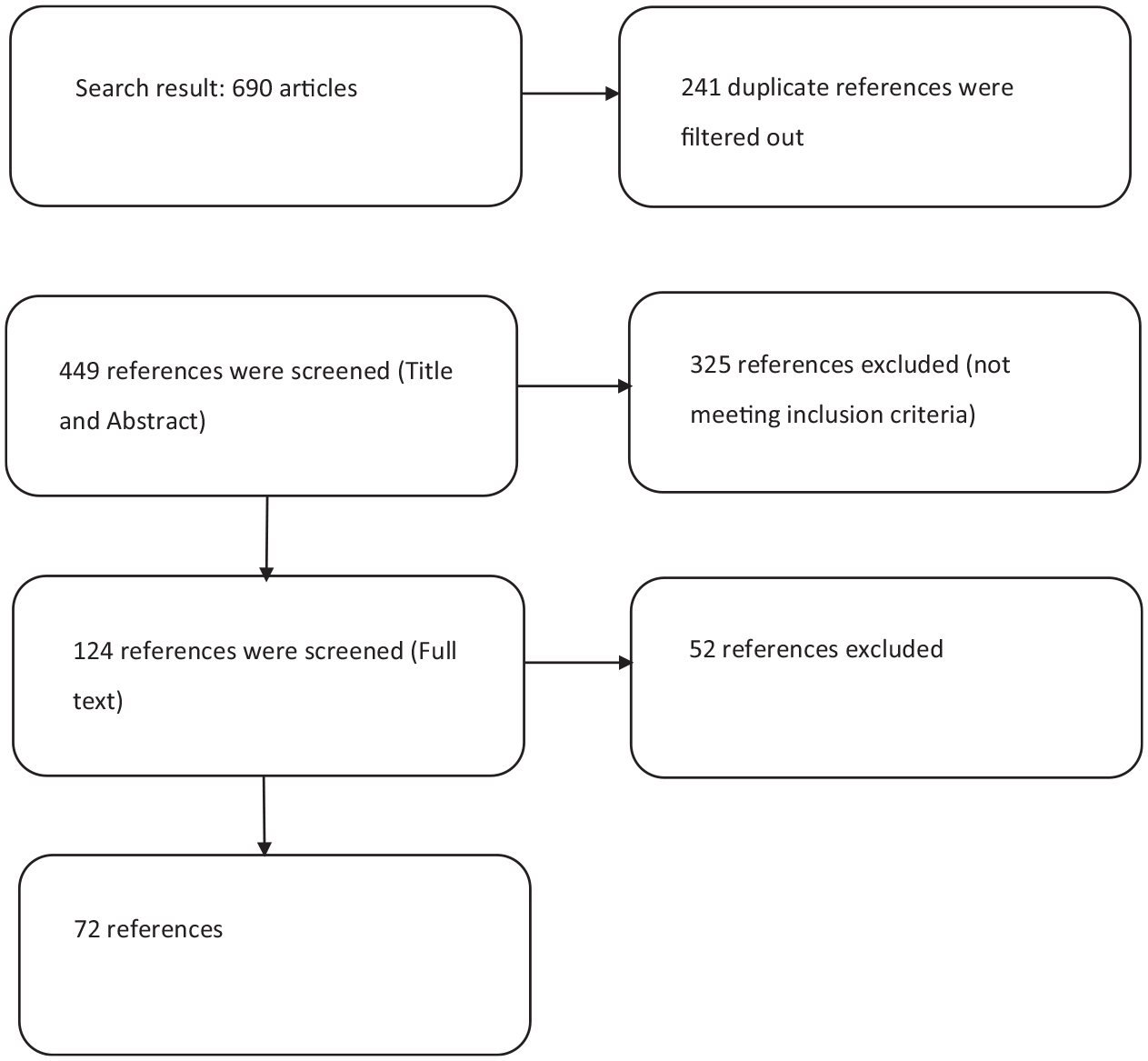
Flowchart of study selection and inclusion process.
Results
Epidemiology
The epidemiology of IS has been extensively studied in retrospective analyses. A large-scale study conducted in the United States in 2020 reported a mean annual incidence rate of 1.6 per 100,000 individuals and a prevalence rate of 4.6 per 100,000 individuals, with associations found between IS and factors such as female gender and African American ancestry. 9 However, a retrospective case series from India revealed that IS predominantly affected males, with a median age of 49.3 years. 10 Similarly, in a study from Thailand, IS-related endophthalmitis was more prevalent in male patients, often accompanied by comorbid diabetes, with a mean age of 56.4 years. 11 Older age has consistently been linked to IS, with mean ages ranging from 67.1 to 70 years in various studies.12–14
Several studies have reported on the epidemiological characteristics of IS concerning causative microorganisms. Fungal-associated IS was more commonly observed in regions with hot and humid climates, often following ocular surgery or trauma. 1 Studies focusing on Herpes simplex virus (HSV)-related IS reported median ages of onset ranging from 54 to 60 years, with a higher incidence among women.15,16 Also, according to studies in the United Kingdom, IS attributed to Acanthamoeba infection had an annual incidence rate of approximately 0.13 per one million individuals, with a median age of 38.5 years. In a retrospective study involving 178 patients with Acanthamoeba keratitis, 33 cases (18.5%) progressed to Acanthamoeba sclerokeratitis, with all but 2 of these cases being contact lens wearers. 17
Risk factor and pathophysiology
IS may result from either primary or secondary etiologies, both of which share common predisposing risk factors. 18
Primary IS mainly develops following traumatic and surgical events. 18 Ocular surgery is the most common etiology of IS, accounting for a significant proportion of cases, ranging from 58% to 83%.2,12,19,20 During the procedures, pathogens invade the sclera, initiating immune-modulated vasculitis and necrosis at the surgical site. 21 Pterygium surgery is the most common surgical procedure associated with IS, followed by scleral buckle surgery and cataract surgery (Figure 2). For instance, Nocardia-associated IS may occur in patients who have hardware in the eye, such as a scleral buckle. 22 It is noteworthy that the interval between a triggering event and the onset of IS varies across different studies. For instance, following pterygium surgery, symptoms can appear within 2 weeks to 20 years 23 (Figures 3 and 4). Other surgeries, such as glaucoma surgery, vitreoretinal surgery, suture removal, and strabismus surgery, have also been linked to IS. 19 Immune-mediated inflammatory conditions, such as atopic dermatitis, synergistically contribute to postoperative IS after eye surgeries. 24 Furthermore, adjunctive administration of radiation or antimetabolite drugs such as MMC is associated with scleral thinning and avascular necrosis, increasing the likelihood of IS development. 25 There are also other iatrogenic causes for IS. For instance, a case report study documented an iatrogenic case of IS with Pseudomonas aeruginosa (PA) following intravitreal ranibizumab injections in a patient suffering from wet age-related macular degeneration. 26

Scleritis following ocular surgeries. (a) After pterygium excision. (b) After scleral buckling. IS following scleral buckle surgery requires the removal of the scleral buckle, similar to any case of IS, due to the presence of a foreign body that necessitates its removal.
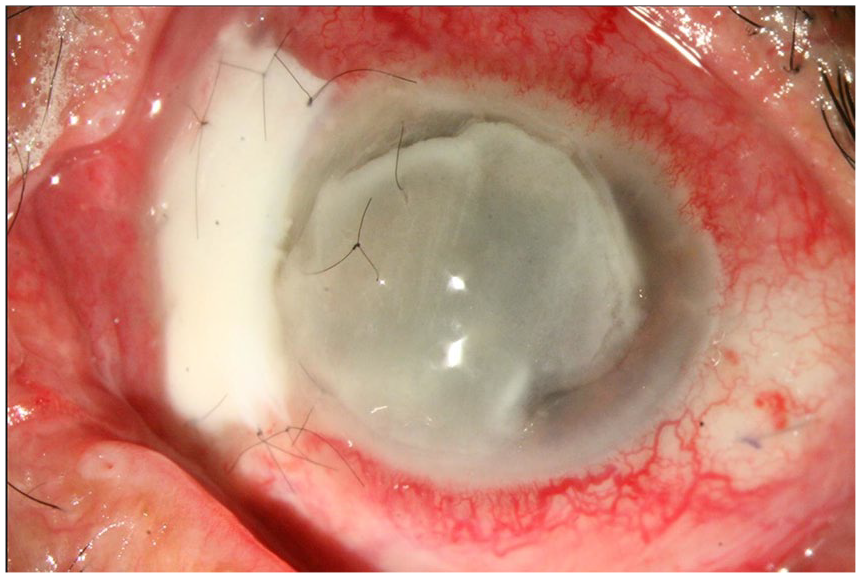
A case of keratoscleritis following pterygium surgery. A scleral patch graft and amniotic transplantation were done previously for that.

Neglected necrotizing scleritis, an 80-year-old patient presented with red eye and decreased vision for 20 days. His surgical history was positive for nasal pterygium removal in his left eye 2 months ago. (a) Prolapsed uvea is notable. (b) Multifocal small pockets of abscess within the necrotic sclera and beneath areas of seemingly healthy sclera (black arrows).
Trauma is another significant risk factor, associated with approximately 10% of IS cases as an independent cause.3,27,28 Traumatic events with organic material are particularly linked to fungi and Nocardia microorganisms. 25 Traumatic cases happen when germs enter the eye through penetrating injuries or when foreign objects are lodged in the sclera. However, getting IS after a trauma is not as common as getting posttraumatic endophthalmitis. 1 Furthermore, a study examining 55 eyes from 53 patients with IS revealed that inciting factors such as preceding ophthalmic surgeries and traumas are the cause of IS for approximately 91% of IS cases. 14
Risk factors for IS also include rheumatologic diseases, chronic use of topical steroids, and systemic immunosuppression such as acquired immunodeficiency syndrome, chemotherapy, and diabetes mellitus.1,9,10,20,29–32 Corticosteroid injections may also increase the risk of IS, as reported by Todokoro et al., where a posterior subtenon injection of triamcinolone acetonide for treating macular edema resulted in late-onset development of Scedosporium apiospermum IS. 33 Although Nocardial scleritis is not typically related to a systemic infection, immunosuppressed patients or those receiving corticosteroid therapy are at higher risk of developing ocular or central nervous system Nocardial infection. 34 Smoking, however, does not appear to significantly impact the incidence and prevalence of IS. 9 Secondary IS, known as corneoscleritis (keratoscleritis) or sclerokeratitis, occurs when a primary corneal infection extends to involve the sclera. Risk factors for corneoscleritis overlap with those of primary IS, and additional factors such as the use of contact lenses, debilitating systemic diseases, and corneal tissue devitalization have been identified. Corneal ulceration is a relatively common underlying cause of IS accounting for 20% of Pseudomonas IS. 29
Organisms can also reach the sclera through the bloodstream, causing septic deposition of emboli. This mechanism may occur in the absence of trauma, surgery, or concurrent corneal infection. Scleral inflammation can also arise as an immune response to foreign or self-antigens in the sclera, along with an underlying infection. 1
Microorganisms
IS can be caused by various microorganisms, including bacteria, fungi, viruses, and parasites (Table 1). The predominant role of bacteria in necrotizing IS has been observed in studies where bacteria accounted for the majority of cases, followed by fungal infections. Bacterial infections are reported to be responsible for approximately 86%–87% of IS cases, while fungal infections account for 11%–13%. 2 However, there are regional variations in the microbial profile of IS.2,14
Causative microorganisms for infectious scleritis in the included studies.

PA is frequently mentioned as the most common pathogen causing IS, followed by gram-positive cocci.1,11,12,18,19,35 The use of MMC as an adjunctive therapy during surgery has been identified as a risk factor for PA infection. This pathogen uses collagenases to destroy the scleral tissue.19,20 Other bacteria that should be considered as a postoperative pathogen for IS are Stenotrophomonas maltophilia, 31 Staphylococcus epidermidis, and Serratia marcescens. 35 Stenotrophomonas maltophilia is less virulent than other more common bacterial causes of IS and less invasive due to its enzymatic properties, leading to an indolent development of IS and thus a later diagnosis. Coinfection with other pathogens is relatively common, and this pathogen is reported to be resistant to multiple antibiotics. These characteristics, along with the risk of recurrence, highlight the need for longer follow-ups. 31 In trauma-related IS, bacteria such as Klebsiella pneumoniae, Enterobacter cloacae, Viridans streptococcus, Enterococcus faecium, and Citrobacter freundii should be considered as potential pathogens. 12 Another study mentioned that Nocardia, Staphylococcus species, and Klebsiella species were also implicated in a significant proportion of cases, often associated with trauma or previous cataract surgery. 10 Different microorganisms have been associated with IS following specific types of ocular surgery. Gram-negative bacteria, particularly PA, were found to be the main culprits after pterygium surgery, while acid-fast microorganisms were responsible for IS following other ocular surgeries. 2
Fungal scleritis demonstrates a more unfavorable prognosis in comparison to bacterial or viral scleritis. This can be attributed to several factors. First, the diagnosis of fungal infections is often delayed due to the inherent difficulties in identifying fungal organisms and the requirement for specialized laboratory testing. Consequently, fungal scleritis has more time to progress before appropriate treatment can be initiated.1,36 Secondly, the dense and avascular nature of the sclera poses a challenge for antifungal medications to effectively penetrate the scleral tissue. As a result, achieving therapeutic drug levels in the sclera becomes problematic, potentially compromising the treatment response. Lastly, fungal infections exhibit more aggressive behavior by invading and destroying tissue rapidly, leading to extensive damage and an increased likelihood of complications. 1 Fungal infections include species such as Cladosporium, Aspergillus, Fusarium solani, Acremonium, Candida albicans, Paecilomyces, Candida parapsilosis, Paecilomyces lilacinus, Pseudallescheria boydii, Bipolaris, and Scedosporium apiospermum.11,12,32,35 Aspergillus is the most common cause of fungal IS that occurs following trauma or has an endogenous origin, while Fusarium oxysporum and Scedosporium apiospermum are more common in fungal IS following ocular surgeries. 2 It is noteworthy that Fusarium is the most significant fungus responsible for keratitis in subtropical regions. Hence, Fusarium-related cases of IS may have originated from the conjunctiva or cornea, even in the absence of surface infection manifestations. 37 Filamentous fungi are more invasive and a more common etiology of IS than yeasts among the fungal etiologies. On the other hand, they also cause more important complications like endophthalmitis. 38 In a study conducted in India, fungal infections were found in around 50% of IS cases, with Aspergillus being the most common fungus identified. 10
Less common microorganisms associated with IS include Treponema pallidum, Corynebacterium diphtheriae, Brevibacterium species, Mycobacterium chelonae, Streptococcus species, Acanthamoeba, and Toxoplasma gondii.7,39,40 Although not common, IS may be the sole and first presentation of syphilis. Shaikh et al. reported a rare presentation of sole nodular syphilitic IS in a patient initially misdiagnosed as having an ocular tumor but showed positive Venereal Disease Research Laboratory (VDRL), Rapid plasma reagin (RPR) test, and Treponema pallidum hemagglutination assay (TPHA), which consequently responded well to a three-week benzathine penicillin treatment. 40 Mycobacterium chelonae, among the other subgroups of Nontuberculous Mycobacterium sp. (NTM), has the greatest number of reports of IS. Mycobacteria grow rapidly and are resistant to typical antituberculous drugs, requiring 4–6 weeks of treatment, longer than other bacterial etiologies such as Pseudomonas, even after initial improvement of the signs. 39 Streptococcus pneumoniae is a well-known pathogenic bacterium associated with IS particularly in seniors with underlying anterior segment diseases. This germ can lead to endophthalmitis and enucleation because of its potential to progress rapidly. 30 Acanthamoeba-related scleritis is likely a result of an immune-mediated response to direct invasion by the organism. Approximately 18.5% of individuals suffering from Acanthamoeba keratitis (AK) progress to develop Acanthamoeba scleritis. Indeed, the majority of Acanthamoeba scleritis cases arise as a complication when the keratitis extends further. 17 Toxoplasma gondii is in the group of pathogens responsible for IS in immunosuppressed patients. It can progress if the treatment is not suitable and may lead to endophthalmitis, retinochoroiditis, and finally enucleation. 41 Intraocular infections from endogenous causes may extend into the sclera and present as scleritis. Such cases of Toxoplasma- and Toxocara-induced scleritis have been reported.42,43
Fastidious organisms, including fungi, NTM, and Nocardia, often lead to a longer interval between the symptom onset and treatment initiation, partly due to the initially negative Gram stain results and the extended time required for acid-fast positivity. 2 Consequently, in cases of IS following retina surgery or when there is no improvement with fluoroquinolone therapy, a higher level of suspicion for fastidious organisms should be maintained. Additionally, conducting acid-fast cultures at the initial presentation may improve diagnostic accuracy and ensure appropriate management of fastidious organism-related IS. 2 Viral infections, specifically HSV or varicella zoster virus (VZV), can also lead to IS, which may manifest as acute or chronic forms, often with a diffuse anterior presentation.15,16 The mechanism underlies direct invasion and the following immune response to the virus, highlighting the autoimmune compartment of viral scleritis. A case report study involving a patient with a positive HLA-B27 demonstrated that VZV scleritis is associated with an autoimmune process by releasing sequestered self-antigens, and both antiviral and immunosuppressive therapy (methotrexate) contributed to the resolution of this condition. 44 Other viral microorganisms, such as Cytomegalovirus and Epstein-Barr virus, are responsible for less frequent cases of scleritis. 8 It is important to consider the diverse range of microorganisms when diagnosing and treating IS, as the appropriate management depends on the underlying pathogen involved.
Clinical manifestation
The presentation mode and course of IS depend on the type of causative organism and the inciting factor. 8 The manifestation of IS following trauma tends to occur more rapidly. The shorter latent period in posttraumatic cases, compared to postsurgical scleritis, might be due to a higher load of microorganisms in trauma. 8 In one study, symptoms appeared within a range of 2–15 days and a median of 7 days after the injury. In contrast, IS caused by surgical factors has a longer latency period, ranging from 10 days to 30 years, with a median of 60 months. 12 Another study, conducted on 56 cases of IS, reported that the mean duration from the onset of clinical manifestations to diagnosis was 1.9 months for postoperative IS, ranging from 0 to 183 months, and 0.2 months for trauma-related IS, ranging from 0 to 3 months. Among the postoperative group, pterygium surgery exhibited a wider range of duration, spanning from 0 to 183 months, with an average duration of 49 months, compared to other surgical procedures, including glaucoma surgery (1 month), cataract surgery (1.4 months), and retinal surgery (1.6 months). 2 Clinical manifestations in fungal IS tend to manifest later than those with IS due to other organisms,12,20 typically occurring around 54 days following fungal infection compared to 32 days following bacterial infection in one study. 20 On the other hand, bacterial infections often present more acutely than those caused by fungi, Nocardia, and mycobacteria. 25 Furthermore, fastidious microorganisms, including fungi, can present as indolent infections, causing a longer course of disease than organisms such as Pseudomonas spp., Staphylococcal spp., and viruses. 8 Fungal IS, even after initiation of treatment, often demonstrates progressive worsening and poor outcome. 1
Regarding symptoms, pain is a key characteristic of scleritis, present in both infectious and noninfectious types. 8 IS with scleral necrosis could be associated with severe pain, while diffuse and nodular scleritis exhibit mild to moderate pain levels. 45 IS following retinal surgeries often exhibits a rapid progression and is characterized by heightened levels of pain compared to IS arising from anterior orbital segment surgeries. 3 In the majority of cases of IS, episcleral or conjunctival hyperemia is a prevalent manifestation, observed in approximately 98% of cases. 2 A study, focusing on 45 cases of IS, identified hyperemia and pain as the main signs and symptoms, presenting in 87% of cases. Notably, the occurrence of hyperemia and pain was closely associated. 19 Furthermore, a study involving 11 eyes with IS reported that pain was the primary symptom in 96% of cases, followed by hyperemia in 89% of cases. 46 Other notable symptoms include redness, purulent discharge, and tearing of the infected eye.25,37
A helpful characteristic in favor of IS diagnosis is when the pain is disproportionate to the findings observed during the exam. 25 Several studies have reported scleral necrosis as a common presentation in patients with IS.2,12 A study revealed that the average extent of necrotic area in cases of scleritis was approximately 3.6 clock hours. Interestingly, patients without a specific triggering factor exhibited a smaller necrotic area compared to those with an identifiable inciting event. Furthermore, when comparing bacterial scleritis to fungal scleritis, bacterial IS cases were found to have larger necrotic areas at initial presentation. 12 The presence of hypopyon is a key sign in distinguishing the infectious nature of the scleritis. 37 The characteristics of IS, such as diffuse or nodular and necrotizing or non-necrotizing, provide partial insight into the etiologic microorganism. 25 In the case of nodular IS, the nodules may present as solitary or multiple lesions with a yellowish appearance beneath the conjunctiva. However, the number of nodules in nodular IS cases is not indicative of a specific pathogen; instead, it is more related to elements such as the burden of infection. 25 HSV-related IS characterized by diffuse anterior scleritis (80%), anterior nodules (11.4%), scleral necrosis (8.6%), and corneal involvement (23%).8,16 Gonzalez et al. described 35 cases of herpes-associated scleritis; most patients presented with acute (85.7%) and unilateral (80%) scleral inflammation. Unilaterality was more common in herpetic scleritis (80%) than in idiopathic disease (56.7%, p < 0.05). 16 In cases of IS related to tuberculosis infection, the presentation can manifest as diffuse scleritis (66.6%) or nodular scleritis (33.3%), with rare cases of concurrent posterior scleritis. 47 A summary of clinical manifestations is provided in Table 2.
Clinical manifestations and complications in patients with infectious scleritis in the included studies.

Differential diagnosis and evaluation
During the examination, it is crucial to differentiate scleritis from conjunctivitis and episcleritis, as these conditions involve inflammation that occurs superficially to the sclera. 5 A key distinguishing factor is the presence of pain and tenderness upon palpation of the globe, which is a characteristic of scleritis but not of conjunctivitis or episcleritis. Additionally, the specific pattern of the injected vessels provides valuable diagnostic information. In scleritis, the injected scleral vessels exhibit a crosshatched pattern and are firmly adherent to the sclera. Conversely, in conjunctivitis and episcleritis, the injected vessels of the conjunctiva and episclera may be moved relative to the sclera when gently touched with a cotton-tipped applicator, although less so for the episcleral than the conjunctival vessels. Also, in scleritis, the injection does not blanch much using phenylephrine eye drops. These clinical features aid in accurately identifying and distinguishing between these ocular conditions. 5 Another important differential diagnosis in suspected IS cases is anterior uveitis, which can also be a complication of IS due to the extension of inflammation from the sclera.18,48 Clinical features can help differentiate between the two conditions. For example, the vascular congestion seen in anterior uveitis is usually perilimbal, while the congestion associated with scleritis tends to be diffuse or sectorial. The cases of post-scleritis uveitis occur following the extension of the scleral inflammation, whereas primary uveitis is associated with a different process involving environmental and genetic factors. 48
Differentiating between IS and noninfectious scleritis is challenging but important. Delays in diagnosing IS cause poor outcomes due to the administration of immunosuppressives as the main treatment for immune-mediated scleritis and the lack of antimicrobial treatment. For instance, the lack of systemic and corneal manifestations often leads to delayed diagnosis of HSV-related IS and subsequent treatment, underscoring the need for thorough evaluation in patients with a previous history of documented HSV infection, especially when there is no improvement with immunosuppressive therapy.8,16 There are some ways of differentiating IS from noninfectious scleritis. Noninfectious scleritis is more common worldwide, and its incidence rate varies according to the geographical zone. IS majorly occurs after trauma or ocular surgeries worldwide, while noninfectious scleritis is more common following autoimmune diseases. A diverse range of underlying diseases leads to the formation of noninfectious scleritis, such as connective tissue diseases and other inflammatory conditions accompanying vasculitis (e.g., systemic lupus erythematosus, rheumatoid arthritis), vasculitic diseases (e.g., polyarteritis nodosa, IgA vasculitis), medication‑induced (e.g., anticonvulsants, bisphosphonates), and miscellaneous disorders (e.g., Gout). Noninfectious scleritis is not associated with abscesses and pus, and has general pain that can spread to the face. Moreover, it can present either with nodular or diffuse patterns accompanied by episcleral vessel congestion. On the other hand, IS presents with purulent exudates, scleral abscesses, and ulcers or may be associated with hypopyon. 8 Another helpful factor is that peripheral keratitis, a condition characterized by inflammation of the cornea periphery, is more commonly observed in patients with IS compared to those with noninfectious scleritis, with frequencies of 22.9% and 10.3%, respectively. It should also be noted that unilateral sclerouveitis or sclerokeratitis, inflammation involving the sclera and uvea or cornea, respectively, may indicate an underlying infectious etiology, particularly when there are no accompanying symptoms of systemic disease. 16 Unilateral presentation is more common in HSV-related IS compared to infections caused by other microorganisms.8,16 A notable differential diagnosis for postsurgical IS is surgically induced necrotizing scleritis (SINS), a rare complication of pterygium or extracapsular cataract extraction surgery due to extreme conjunctival manipulation and cautery of episcleral vessels in cases with an approximately 90% undiagnosed systemic autoimmune disease. 8 The most notable surgical procedure related to both IS and SINS is pterygium excision. Distinguishing between the two conditions could be challenging since they closely resemble each other. The key characteristic of SINS is scleral necrosis, which is present in many cases of IS. However, the presence of hypopyon and discharge tends to indicate IS. 49 SINS typically exhibits a more prolonged latent period. 8 Furthermore, the type of abscess contributes to the diagnosis, with unifocal abscesses being more commonly observed in IS, accounting for approximately 78% of cases, compared to multifocal abscesses, which are more frequently seen in inflammatory scleritis and SINS. 20 Conversely, the diffuse form of abscesses is rare in comparison to the other two groups. 20 These abscesses typically exhibit a distribution pattern extending superiorly or inferiorly in an arc shape, with a distance of approximately 3–4 mm from the limbus. 50 The clinical symptoms for both infectious and AS can appear similar. To differentiate IS from AS, accurate history is crucial. About 94% of patients (n = 48) had a predisposing factor for the infection. 14 Histopathological examination may also help in differentiating between them, yet it is challenging in certain IS cases such as herpes zoster scleritis. 8
Although uncommon, malignancies can present similarly to IS. Therefore, in cases of treatment-resistant IS or atypical manifestations, it is crucial to rule out malignancies. 8 Table 3 presents a summary of differential diagnoses.
Differential diagnosis for infectious scleritis.

At the time of initial diagnosis of scleritis, it is recommended that patients undergo both clinical and laboratory evaluations to assess for vasculitis. The suggested laboratory tests include complete blood count (CBC), comprehensive metabolic panel (CMP), urinalysis, testing for perinuclear antineutrophil cytoplasmic antibodies (P-ANCA) and cytoplasmic antineutrophil cytoplasmic antibodies (C-ANCA), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and a chest x-ray. This comprehensive evaluation aims to identify potential underlying vasculitic conditions.
In cases where patients have a high-risk history or clinical suspicion of IS, further evaluation is warranted. Diagnostic measures for IS involve preparing microbiologic smears and culturing samples obtained from swabs, spatulas, or biopsies of the affected scleral tissue. These samples should be cultured on various media, including blood agar, chocolate agar, thioglycolate, Sabouraud dextrose agar, non-nutrient agar with Escherichia coli, and brain–heart infusion broth. 51 If initial culture results are negative, additional methods such as immunohistochemistry and titers should be employed to enhance the detection of possible infectious agents.3,16 Repeat scraping for culture or even a scleral biopsy, sent for both culture and histopathology, may also be warranted. 51
In cases of suspected IS, specific laboratory techniques should be employed to detect certain pathogens. For example, specimens should be stained for acid-fast bacilli and cultured on Löwenstein–Jensen medium, which is commonly used for tuberculosis detection. 52 Additionally, obtaining the QuantiFERON-TB Gold in-tube test can be beneficial in assessing the presence of tuberculosis infection. 47 Another helpful technique is the polymerase chain reaction (PCR) analysis of the aqueous humor in case of suspicion of viral microorganisms, for example, scleritis due to reactivation of latent VZV. 44
When sclerokeratitis with a possible Acanthamoeba infection is suspected, additional staining techniques such as calcofluor white or specific antibodies should be utilized. Moreover, confocal microscopy serves as another useful diagnostic tool. 53 Furthermore, plating the specimens on non-nutrient agar overlaid with Escherichia coli can facilitate the growth and identification of Acanthamoeba. It is important to note that staining and cultures for Acanthamoeba are more commonly positive from the cornea rather than from the sclera. 17 Ultimately, serological assessments, along with blood and urine tests, and diagnostic imaging are critical to exclude endogenous IS linked with Lyme disease, syphilis, tuberculosis, and Toxoplasma gondii. 47 In confirmed syphilis cases, IS must be differentiated from intraocular inflammation due to ciliary body gummas, which are the characteristics of the tertiary stage of syphilis. 40 A flowchart for the diagnostic workup is presented in Figure 5.

Flowchart for the diagnostic workup.
Prevention and treatment
Multiple studies emphasize the significance of preventing IS. Various measures have been identified to reduce the risk of infection. In the case of postsurgical IS prevention, opting for the optimal surgical technique, ensuring regular postoperative follow-up sessions, and informing the patient about the rare possibility of IS development are recommended. 48 For example, during surgery, it is recommended to avoid excessive cautery to preserve episcleral blood flow, thus promoting better wound healing. 50 Leaving the sclera bare, as this leaves the surface vulnerable to infection, should be avoided. 51
It is crucial to consider the possibility of IS before initiating treatment with steroids for presumed inflammatory scleritis. This precaution is essential to prevent worsening of the infection and associated complications. Accurate diagnosis and appropriate management are vital for achieving favorable outcomes in patients with scleritis.
Treatment strategies for IS depend on the causative microorganism. In addition to the necessity for choosing the correct antimicrobial drug, opting for the optimal administration route of medical treatment is important, considering that the sclera is an avascular tissue that poses the risk of poor drug penetrance. 54 In all cases, medical treatment involving topical, systemic, and sometimes subconjunctival injection of antibiotics (in more severe cases) is employed. In case of aggressive infection, a combination of topical, oral, and intravenous antimicrobial agents may be required. 26 However, the success rate of medical treatment alone in IS for clearing the sclera of infection, is relatively low at 18%. 2 It is noteworthy that the treatment regimen should be primarily determined by antibiotic sensitivity analyses and, in more complex cases, ophthalmologists should consider consultation with infectious disease specialists using a multidisciplinary approach. Further studies are recommended regarding the optimal duration of antimicrobial therapy.
In cases where PA is suspected, Fluoroquinolone drugs such as ciprofloxacin are considered as useful therapeutic options. 36 Moreover, studies show that topical gatifloxacin 0.3% or amikacin 2.5% and systemic gatifloxacin at a dosage of 400 mg every 12 h can effectively cover the pathogen.12,27 In our experience, topical tobramycin 1.4% and other topical and systemic fluoroquinolones with coverage of PA are also useful. Systemic fluoroquinolones are systemic broad-spectrum antibiotics and cover a wide range of both gram-positive and gram-negative microorganisms. It penetrates well in most extracellular and intracellular fluids and distributes easily to all tissues of the body. 55 Unfortunately, with the increasing prevalence of multidrug-resistant PA keratitis, we may encounter this type of infection in IS cases. There is one recent report of IS caused by this strain of PA that was successfully treated with both topical (0.19%) and intravenous colistin, alongside dexamethasone. 56 Despite controversies in the use of corticosteroids for IS, a study on 24 individuals with confirmed PA scleritis compared patients receiving corticosteroids as part of their management with those who did not and reported using oral steroids could be beneficial as a part of treatment in PA-related IS cases without causing adverse effects, which is probably due to the inflammatory nature of the condition following the pathogenic invasion of the eye. The mean age of participants in this study was 72.5 years, with a standard deviation of 12.5 years, and previous surgery was the most common inciting factor. 29
For infections caused by Staphylococcus and Streptococcus, cefazolin 5% and topical gatifloxacin or ofloxacin 0.3% (also effective against PA) can be used. 27 Intravenous administration of antibiotics can be considered in extensive infections of the sclera. 45 In cases of cefazolin resistance or a positive culture for methicillin-resistant Staphylococcus aureus, topical, intravenous and subconjunctival vancomycin may be necessary. 25 If an abscess is present in IS, surgical drainage and debridement in addition to the use of topical and systemic antibiotics are recommended. 46
Trauma involving agricultural material requires consideration of fungal microorganisms, underscoring the need for prompt diagnosis and appropriate therapeutic measures targeting fungi in such cases. Topical antifungals like natamycin 5% or voriconazole 1% and systemic administration of ketoconazole or itraconazole are suitable treatment options. Fungal IS typically requires a longer treatment duration compared to bacterial IS, with bacterial cases often treated for a maximum of 3 months and fungal cases sometimes necessitating treatment for up to a year. 45 Moreover, in vitro and human studies have suggested that in cases of limited effectiveness with treatment by only topical voriconazole, systemic treatment with intravenous voriconazole could be beneficial. 33 Streptococcus pneumoniae-related IS can be managed with oral and topical moxifloxacin, topical ciprofloxacin, and systemic intravenous cefalotin. However, the response of Streptococcus pneumoniae to fluoroquinolones is variable.4,30,57 Standard antituberculosis therapy, combined with corticosteroids or methotrexate in some cases, has shown favorable outcomes in cases associated with tuberculosis, resulting in remission in approximately 93.3% of patients. Notably, antituberculosis therapy should be initiated in collaboration with infectious disease specialists before starting any immunosuppressive treatment. 47 Nocardia infections can be treated with trimethoprim–sulfamethoxazole, while amoxicillin–clavulanate and moxifloxacin are alternative options for patients allergic to this medication.34,58 Oral steroids are not recommended in Nocardia-related IS. 48 Amikacin has demonstrated success in treating Nocardia infections, and it has also been effective in cases of IS caused by Mycobacterium chelonae. 45
Because of the combined infectious and inflammatory nature of AK-related scleritis, the use of oral NSAIDs, steroids, and systemic immunosuppressive therapy for severe cases is recommended in addition to anti-AK drugs including topical amoebicidal agents, for example, biguanides (such as polyhexamethylbiguanide 0.02% and chlorhexidine 0.02%) and diamidines (such as propamidine isethionate 0.1% or hexamidine 0.1%), and systemic voriconazole and miltefosine. 17
In patients diagnosed with Toxoplasma gondii, a combination of oral medications has demonstrated effective resolution of the infection. Specifically, treatment with oral trimethoprim/sulfamethoxazole (160 mg/800 mg twice daily) and azithromycin (500 mg) has shown positive outcomes. Notably, no topical application was reported as part of the treatment regimen. 59 This suggests that systemic administration of these medications is effective in managing Toxoplasma gondii infections, leading to successful resolution of the condition.
Acyclovir (first 800 mg five times per day and then less maintenance dose) has shown promise in the case of HSV and VZV IS. 15 Valacyclovir 1000 mg three times daily, or famciclovir 500 mg three times daily, are alternative regimens. 60 Of note, oral corticosteroids have been reported to be detrimental for individuals with HSV-related IS. 48 Table 4 presents a summary of appropriate antimicrobial regimens for different causative microorganisms.
Appropriate antimicrobial regimens for different causative microorganisms in infectious scleritis.

Necrotizing scleritis in IS cases necessitates a combination of treatments, including lesion debridement and possible scleral repair. IS-related endophthalmitis cases often require intravitreal antimicrobial treatment and pars plana vitrectomy, along with corticosteroids. However, although additional interventions like keratoplasty associated with vitrectomy may be necessary, a significant proportion of these cases (70.1%) ultimately require enucleation. 11
Surgical debridement is considered beneficial and is required in many cases to improve prognosis. It can help to better penetrate antibiotics into micro-abscesses in the avascular zones.12,23,27,61 Debridement serves two important functions in the treatment of IS. Firstly, it involves the removal of necrotic tissue, which helps reduce the amount of infected and unhealthy tissue present. Secondly, debridement plays a crucial role in improving the effectiveness of locally administered drugs. Performing surgical debridement involves the removal of necrotic tissue and abscess materials to promote healing and prevent the spread of infection. The conjunctiva is opened up peripherally to the infected area. The necrotic tissue and abscess materials are dissected. Sometimes, the dissection continues until the choroidal pigmentation is visible through the scleral fibers. In cases where the infection involves the sclera beneath the rectus muscle, the muscle may need to be detached and reanchored.23,62 After the debridement is completed, the surgical defect, or the area where the necrotic tissue was removed, is typically covered with conjunctiva, amniotic membrane, umbilical cord tissue, sclera, or cornea as mentioned below. One study suggested that leaving the conjunctiva open at the site of necrosis resulted in successful outcomes in five cases. The purpose of leaving the wound open is to ensure good exposure to topical fortified antibiotics. 61 However, given the need to address severely thin scleral defects and the highly vascularized nature of conjunctival tissue, we generally do not use this technique.
Early surgical intervention within 2.5 days of diagnosis increases the chance of preserving the eye globe by 100%. 23 As previously mentioned, only 18% of IS cases were treated solely with antimicrobial drugs, while the majority of patients undergo some form of surgical treatment. 2 Another study found a lower enucleation rate in IS patients who received surgical treatment (2/11) compared to those treated solely with antimicrobial drugs (3/4). 28 Additional surgical interventions may include scleral transplantation, conjunctival autotransplantation, conjunctival flap procedures, 35 corneoscleral amniotic graft for epithelial defects,12,17,63 cryotherapy, removal of exposed (infected) glaucoma drainage devices, or scleral buckling.2,51 In instances where keratitis poses a threat of invading the sclera, placement of umbilical cord tissue or a therapeutic penetrating keratoplasty (corneal transplant) may be considered.
In brief, surgical intervention is required in cases of IS with the presence of abscesses and necrotic tissue. 46 Thinning of the sclera, with or without exposure of the uveal layer, may warrant consideration for scleral patch grafts or amniotic membrane transplantation. 7 No response to medical treatment, refractory IS, and involvement of adjacent structures are further indications for surgical intervention.11,64
In our practice, we treat localized necrotic or abscess-forming IS lesions of less than 2 mm in diameter using debridement, sometimes supplemented with cyanoacrylate glue or conjunctival graft. Cyanoacrylate has antimicrobial effects, suppresses neutrophil migration, and can induce vascularization at the site. However, for more extensive IS cases, we employ surgical debridement along with conjunctival autografts, amniotic membrane grafts, umbilical cords, or mucous membrane grafts. Scleral grafting also aims to reconstruct and reinforce the damaged scleral tissue. 59 We commonly use a corneal patch graft in our approach to patients, as it offers increased resistance to further melting and provides transparency for examining underlying tissue, making it an excellent option, particularly in recurrent cases.59,65
Visual outcome
Several studies have reported varying outcomes in terms of VA after treatment for IS. Some studies have shown improvements in VA, while others reported sustained or decreased VA.11,30,45 Poor visual outcomes have been associated with certain prognostic parameters, including poor VA at presentation, endophthalmitis, keratitis, fungal etiology, and medical therapy without surgical debridement.13,66 There is conflicting data regarding surgery, as some studies have shown that despite its beneficial role in maintaining the eye globe, surgical intervention does not enhance visual outcomes. 25 Moreover, worse visual outcomes are not significantly associated with the type of responsible organism or the multifocal abscesses. 25
In a study focused on fungal IS, it was found that after treatment, 41.6% of patients had BCVA (best corrected visual acuity) better than 6/18, 33% had BCVA between 6/18 and 6/60, and 25% had final BCVA worse than 6/60. The study also reported a rate of evisceration of approximately 13%. 10 Another significant finding was that patients with initial VA less than 20/200 experienced a higher rate of vision loss compared to those with VA above 20/200. The vision loss rates at the first and third months were 86% and 74%, respectively, for patients with VA less than 20/200, while for patients with VA above 20/200, the rates were 5% and 18%. 2
In a study by Glenn et al. in 2022, which included 26 cases of IS, the mean BCVA at presentation was approximately 20/400, with a final BCVA of about 20/800. Among these patients, 27% experienced vision loss, and 54% had poor vision as the outcome. The study identified initial low VA, fungal infection, and scleral necrosis as factors associated with poor visual outcomes, while combined medical and surgical treatments affected only the time required to resolve the infection, not the final visual outcomes. 13
Another study suggested that visual outcomes were not related to surgical or traumatic causes of IS but were poor in cases involving scleral thinning, VA less than 20/200 at presentation, and prolonged hospitalization. In this study, 79% of patients had VA less than 20/200 after treatment. 12 Scleral necrosis was identified as another parameter associated with poor visual outcomes in IS, requiring immunosuppressive drugs for management. Overall, visual outcomes in IS, even with appropriate treatment, tend to be poorer compared to anterior scleritis or idiopathic scleritis. 67 Isolated IS, however, has a better prognosis compared to sclerokeratitis. 2
Ophthalmic conditions, such as cataracts, fibrotic pupillary membranes, glaucoma, detachment of the retina or choroid, keratitis, and endophthalmitis, can lead to visual loss.2,27,68 In a study involving 56 eyes, it was found that 50% of eyes lost VA after appropriate treatment of IS, with 25 out of 33 cases being irreversible and only 8 cases showing improvement (VA above 20/200). 2
Ahmad et al. reported that in their study of 24 IS cases related to presumed autoimmune etiology, 54% of patients had VA less than 20/200 at baseline. After 1 year of treatment, 53% of patients had VA above 20/200, and at the end of the 14-year follow-up, 58% had VA above 20/200. Approximately 37.5% of patients experienced vision loss due to corneal scarring, retinal changes, and glaucoma. One patient underwent enucleation due to phthisis. 29
In cases of HSV-related IS, vision loss occurs in 34.3% of patients, with no significant difference observed among the various types of scleritis. However, herpetic scleritis is associated with a significantly higher rate of vision loss compared to idiopathic scleritis 16 (34.3% vs 11.5%; p < 0.001).
Complications
Complications associated with IS have been extensively documented in the literature, highlighting the potential risks and adverse outcomes of this sight-threatening condition (Table 2). Notable complications include glaucoma, corneal opacity, cataract formation, epithelial defects, uveal prolapse, globe perforation, endophthalmitis, scleral thinning, calcified plaques, retinitis, retinal and choroidal detachment, and fibrotic pupillary membrane formation.2,12,17,20,21,27,69 Furthermore, complications such as macular scarring and phthisis bulbi have been reported. 36 Of particular concern are complications such as endophthalmitis and keratitis, which may necessiate enucleation or evisceration.2,17,20,27 Recurrence, which is more common in fungal IS compared to bacterial IS, has also been identified as a potential complication.20,35 It is worth noting that certain microorganisms, including Brevibacterium species and Acanthamoeba, have been associated with recurrence even after completing a course of treatment. 20 Recurrence rates were found to be significant in IS cases related to tuberculosis, with all 15 patients in one study experiencing subsequent episodes. 47
In a study focused on IS-related endophthalmitis, various complications were observed, such as corneal scarring (64.4%), glaucoma (58.6%), panophthalmitis (18.4%), phthisis bulbi (10.3%), iris neovascularization (3.4%), cataract (3.4%), and retinal detachment (2.3%). 11 Other associated complications include posterior synechiae formation, subconjunctival abscess, and a reduction in VA.35,69 It is worth noting that the actual affected area may be larger than what specialists observe during examinations, such as when using a slit lamp, suggesting that the full extent of the involvement may not always be apparent. 10 Surgical debridement, a treatment approach employed in IS cases, can result in additional complications, including itching, pain, and blurred vision. 70
IS resulting from Nocardial infection presents with typical manifestations with pain, hyperemia, and visual disturbances and is characterized by the formation of nodular abscesses.58,71 IS following retinal surgery is more frequently associated with posterior scleral thinning and choroidal or retinal detachment.3,72 Additionally, tuberculosis-related IS patients may exhibit uveitis and peripheral keratitis, both of which are observed in approximately 33% of affected individuals. 47 Fungal IS associated with the development of cataracts, choroidal or retinal detachment, phthisis, and endophthalmitis. Enucleation is more common in fungal scleritis than in other etiologies. 1 Additionally, approximately 37% of HSV-related IS patients may initially present with both scleral inflammation and uveitis, while 23% may exhibit peripheral keratitis alongside scleritis.8,16 HSV-related IS presents with distinct features such as perilimbal devascularization, moderate to severe pain, uveitis, corneal and scleral thinning, significant VA decline compared to other causes of IS,15,16 as well as a higher prevalence of glaucoma when compared to idiopathic IS. 16 However, it does not involve the posterior sclera or vitreoretinal areas, nor does it cause scleromalacia.15,16
Conclusion
This study highlights the clinical importance of IS despite its relatively low incidence and prevalence. IS constitutes a critical medical condition that often results in vision loss among patients presenting with scleritis. Early diagnosis of IS crucial as the disease can progress rapidly, leading to a poor prognosis, especially in cases misdiagnosed as noninfectious scleritis. Particularly in cases of treatment-resistant anterior scleritis or when disease progression continues despite ongoing treatment, consideration should be given to the possibility of IS. Therefore, it is essential to include IS as a differential diagnosis in patients presenting with ocular pain and hyperemia, especially in those with a documented history of trauma or ocular surgeries, given the wide range of the timeline for IS incidence.
While bacterial causes, particularly PA, are the most common etiology of IS, the prognosis is particularly poor in cases of fungal-related IS. Empirical treatment should account for the possibility of bacterial involvement, particularly PA. In our experience, surgical interventions such as debridement, grafting, or device removal, when combined with appropriate medical treatment, can improve outcomes. It is important to note that relying solely on medical treatment without considering surgical options should be avoided in managing IS.