
Abstract
Background:
Selective suture removal has been demonstrated to be effective in reducing post-keratoplasty astigmatism, while the remaining sutures are left in place. Existing studies typically focus on outcomes immediately after selective suture removal, without delving into the final suture-out keratometric astigmatism.
Objectives:
To examine the impact of selective suture removal on corneal graft astigmatism following keratoplasty in keratoconus and identify potential factors associated with the changes in graft astigmatism after suture removal.
Design:
Retrospective, comparative interventional case series.
Methods:
The study included 118 consecutive eyes of 118 cases that underwent corneal transplantation for keratoconus and had a keratometric astigmatism of ⩾4 D. One or two interrupted sutures corresponding to the steep meridian were removed per session. Patients were re-evaluated at 1 to 2-month intervals, repeating the procedure until achieving a keratometric astigmatism of <4.0 D or no interrupted sutures remained in the steep meridian.
Results:
The mean recipient age was 28.4 ± 8.4 years. A total of 234 selective suture removals were performed, with a mean of 2.0 ± 1.1 removals per eye. Pre-suture removal keratometric astigmatism significantly decreased from 6.3 ± 2.0 D to 3.91 ± 2.23 D after the completion of selective suture removal (p < 0.001). This value was significantly increased to 5.45 ± 2.93 D after all suture removal (p < 0.001). Higher pre-suture removal astigmatism and deep anterior lamellar keratoplasty were associated with a more favorable response to selective suture removal.
Conclusion:
Selective suture removal effectively modifies graft curvature to reduce post-keratoplasty astigmatism in keratoconus patients. However, its efficacy markedly diminishes after all sutures are removed. This procedure is particularly effective in patients with higher pre-suture removal astigmatism and those undergoing deep anterior lamellar keratoplasty.
Plain language summary
Selective suture removal has been demonstrated to be effective in reducing post-keratoplasty astigmatism, while the remaining sutures are left in place. Existing studies typically focus on outcomes immediately after selective suture removal, without delving into the final suture-out keratometric astigmatism. The efficacy of selective suture removal markedly diminishes after all sutures are removed. Higher pre-suture removal astigmatism and deep anterior lamellar keratoplasty predict more favorable response to selective suture removal.
Introduction
Corneal transplantation for keratoconus has exhibited remarkable success in terms of graft survival, thanks to advancements in surgical techniques, instrumentation, and postoperative care.1–3 However, residual astigmatism poses a significant challenge to early visual rehabilitation and the overall success of keratoplasty.1–4 Various factors contribute to post-keratoplasty astigmatism, such as suture tension, centration of recipient trephination, transplant shape, alignment of donor tissue with recipient tissue, donor-recipient size and thickness differences, tissue apposition, and the healing response. 4
During the initial postoperative period with sutures in place, management of graft astigmatism primarily involves selective removal of interrupted sutures or adjustment of suture tension in continuous sutures. Multiple studies have demonstrated the efficacy of selective suture removal in reducing post-keratoplasty astigmatism.4–8 However, existing studies encompass a range of preoperative diagnoses and typically focus on outcomes immediately after selective suture removal, without delving into the final suture-out keratometric astigmatism. The long-term refractive success of corneal transplantation relies on corneal curvature when all sutures are eventually removed. The present study evaluates the effectiveness of selective removal of interrupted sutures in managing post-keratoplasty astigmatism specifically in keratoconus patients. Our assessment includes the impact of selective suture removal with remaining sutures in place and after complete suture removal. In addition, we aim to identify factors that could contribute to changes in graft astigmatism following suture removal.
Methods
We included all patients who underwent their initial corneal transplant for keratoconus between February 25, 1994 and January 27, 2020 and subsequently underwent selective removal of interrupted sutures for the management of high graft astigmatism. Inclusion criteria necessitated a follow-up visit performed at least 3 months after complete suture removal. Exclusion criteria comprised preoperative corneal vascularization, additional ocular diseases besides keratoconus, absence of keratometry readings before or after selective suture removal, graft ovality or eccentricity, donor-recipient junction abnormalities such as overriding and underriding, suture replacement due to premature suture loosening, suture-related complications, presence of retained sutures at the final visit, and graft opacity or failure. Furthermore, patients were excluded if the continuous suture was removed before all interrupted sutures were extracted. If subsequent surgical interventions were performed following complete suture removal, only outcomes preceding the secondary procedures were considered for statistical analyses.
Preoperative examination
Demographic and baseline data, including age, gender, uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), refractive error, keratometry readings using a manual keratometer (Javal-Schiotz keratometer; Haag-Streit AG, Köniz, Switzerland), and intraocular pressure, were documented. All patients underwent slit-lamp examination and dilated indirect ophthalmoscopy. Diagnosis of keratoconus was confirmed using a Placido disk-based topography (TMS-1 Topographic Modeling System, version 1.61; Computed Anatomy Inc., New York, NY, USA), and central pachymetry was measured using an ultrasonic contact probe (A/B scan; Sonomed Inc., Lake Success, NY, USA).
Surgical technique
All corneal transplantations were performed by a single surgeon (M.A.J.) under general anesthesia. Penetrating keratoplasty (PK) was the exclusive technique until April 10, 2006. Subsequently, deep anterior lamellar keratoplasty (DALK) became the primary procedure, with PK reserved for cases of previous hydrops or extensive intraoperative Descemet membrane perforation incompatible with lamellar keratoplasty. The recipient cornea was trephined using a single-use Hessburg-Barron trephine (Katena Products Inc., Denville, NJ, USA), with the trephine diameter set 2.5 mm smaller than the vertical corneal diameter for both PK and DALK. In DALK, attempts were made to achieve a big bubble; if unsuccessful, predescemetic DALK was pursued, involving stromal removal down to the Descemet membrane. Donor corneas were cut endothelium-side using a new Barron punch (Katena Products Inc., Denville, NJ, USA), with a donor-recipient disparity of 0.25 mm in all cases. The donor cornea was secured into the recipient using four 10-0 monofilament nylon cardinal sutures (Sharpoint; Angiotech, Vancouver, BC, Canada), which were later replaced by main sutures comprising either 16 interrupted radial sutures or 8 interrupted radial sutures combined with a 16-bite continuous suture. Continuous sutures were placed clockwise with two radial bites between adjacent interrupted sutures, extending approximately 0.75 mm on each side of the graft-host junction and to a depth of 70%–90% of corneal thickness. Suture knots were buried after ensuring adequate anterior chamber reformation. Intraoperatively, suture tension adjustment was performed, and any loose, tight, or nonradial sutures were replaced. Subconjunctival injection of betamethasone (4 mg) and cefazolin (100 mg) was administered at the conclusion of surgery. Patients received chloramphenicol 0.5% eyedrops four times daily for 14 days and betamethasone 0.1% eyedrops four times daily, gradually tapered off.
Selective suture removal
Selective removal of interrupted sutures was undertaken when refractive and keratometric astigmatism reached ⩾4 D; starting 1 month post-keratoplasty in eyes with combined suturing technique and 2 months postoperatively in eyes with interrupted sutures. At each session, one or two interrupted sutures corresponding to the steep meridian were removed: one suture for astigmatism between 4 and 6 D, and two opposing sutures for astigmatism >6 D. For astigmatism ⩽6 D, slit-lamp microscopy aided in identifying the tighter suture, based on tissue distortion and the angle acuteness at suture ends. Patients were re-evaluated in 1–2 months and the procedure was repeated until keratometric astigmatism was <4.0 D or maximum benefit was achieved with no interrupted sutures in the steep meridian. Remaining sutures were left until biodegradation upon reaching an acceptable level of keratometric astigmatism. Complete suture removal was scheduled after 12–18 months when high astigmatism persisted despite selective suture removal. Topical corticosteroids and antibiotics were administered for 1 week after each suture removal session. There was no tension adjustment of any continuous sutures during the study duration.
Outcome measures
The primary outcome measure assessed changes in keratometric astigmatism following selective and complete suture removal. The secondary outcome measure explored potential influencing factors on these changes, such as recipient sex and age, severity stage of keratoconus according to the Amsler–Krumeich keratoconus classification, 9 keratoplasty technique, donor quality, graft size, suturing technique, number of selective suture removals, duration of corticosteroid application, and intervals to initial and complete suture removal.
Visual acuity, refraction, and keratometric astigmatism were evaluated immediately before and 4–6 weeks after each session of selective suture removal, 2–3 months post final selective suture removal, and within 3–12 months after suture removal completion. Visual acuity changes were defined as an increase or decrease by at least one line on the standard Snellen chart. Changes in keratometric astigmatism were analyzed in two ways: net difference and vectorial difference. Net difference was computed by subtracting the keratometric astigmatism measured before and after suture removal, irrespective of axis change. Positive and negative values denoted a decrease and increase in keratometric astigmatism, respectively. A change of less than 1 D in keratometric astigmatism was categorized as “no change.” Vector analysis was performed using double-angled plots (Astigmatism Double Angle Plot Tool V.1.3.0 available online on the ASCRS website). These plots require doubling the axis of astigmatism to transform its magnitude into 360° Cartesian coordinates. Double-angled plots display the magnitude and axis of the vectoral center of the data (centroid) and the 95% confidence ellipse of the centroid, which is the two-variable analog of the confidence interval for single-variable analyses.
Statistical analysis
SPSS statistical software version 25 (IBM Corp., Armonk, NY, USA) was utilized for statistical analysis. Continuous variables were expressed as mean ± standard deviation and range, while categorical variables were presented as frequencies and percentages. Normal distribution of continuous data was assessed by the Kolmogorov–Smirnov test and Q-Q plots. The Wilcoxon test was employed to compare keratometric astigmatism before and after suture removal. Analysis of variance with Bonferroni correction was conducted to compare UCVA, CDVA, refractive error, and keratometry readings measured throughout the study period. Multinomial logistic regression models were used to assess the correlation between different patterns of change in keratometric astigmatism post-suture removal and independent factors. A significance level of p < 0.05 was considered statistically significant.
Results
A total of 1268 consecutive eyes diagnosed with keratoconus underwent corneal transplantation during the study period. Among these, 581 eyes underwent selective suture removal to mitigate high graft astigmatism. We excluded 463 eyes for various reasons: suture-related complications (310 eyes), removal of continuous sutures before interrupted suture removal (46 eyes), persistence of sutures at the last visit (33 eyes), suture replacement due to premature loosening (21 eyes) or traumatic wound dehiscence (9 eyes), absence of keratometry readings before or after suture removal (38 eyes), and graft opacity/failure (6 eyes). Following these exclusions, 118 eyes (62 right eyes, 52.5%) of 118 patients (77 males, 65.3%) remained for analyses.
The mean recipient age was 28.4 ± 8.4 years, ranging from 15 to 52 years. Corneal stromal scarring was observed in 54 eyes (45.8%). Preoperative central corneal thickness averaged 424.1 ± 59.9 microns (range, 325–531 microns). Preoperative mean keratometry and keratometric astigmatism were 54.83 ± 5.19 D (range, 49.0–69.5 D) and 7.21 ± 4.0 D (range, 3.0–18.0 D), respectively. According to the Amsler–Krumeich classification, 12 eyes (10.2%) were categorized as stage 2, 26 (22.0%) as stage 3, and 80 (67.8%) as stage 4 keratoconus.
The keratoplasty technique employed was PK in 50 eyes (42.4%) and DALK in 68 eyes (57.6%). Among DALK procedures, 50 eyes achieved a bared Descemet membrane, while 18 eyes underwent manual predescemetic DALK. Suturing technique included interrupted sutures in 51 eyes (43.2%) and combined in 67 eyes (56.8%). Table 1 provides pertinent data regarding donor corneas, including donor age, donor quality, and graft size. Patients received topical corticosteroids for 7.3 ± 2.8 months postoperatively, ranging from 5 to 11 months.
Characteristics of donor corneas used in keratoconus corneal transplantation.

Number and time interval of selective suture removal
A total of 234 selective removals of interrupted sutures were performed, with a mean of 2.0 ± 1.1 removals per patient (range, 1–6). The procedure was performed once in 47 eyes (39.8%), twice in 42 eyes (35.6%), three times in 18 eyes (15.3%), four times in 8 eyes (6.8%), five times in 1 eye (0.8%), and six times in 2 eyes (1.7%), with 90.7% of cases requiring three or fewer removals. The interval from keratoplasty to the initiation of selective suture removal was 5.9 ± 4.3 months (range, 1–22 months). Interrupted suture removal was initiated within 6 and 12 months postoperatively in 80 eyes (67.8%) and 107 eyes (90.7%), respectively. The intervals from keratoplasty to the second, third, and fourth selective suture removal were 7.6 ± 4.4 months (range, 2–27 months), 8.6 ± 2.7 months (range, 4–18 months), and 10.3 ± 4.6 months (range, 5–22 months), respectively. Sutures were completely removed at 8.6 ± 7.6 months (range, 3–42 months) after the final selective suture removal. No patients experienced complications related to suture removal, including inadvertent cutting of continuous sutures, wound leaks, wound overriding, wound dehiscence, graft rejection, or infection.
Visual, refractive, and keratometric outcomes
There was no significant difference in UCVA between the initiation of selective suture removal and its completion. However, UCVA showed a significant decrease after complete suture removal (Table 2). Notably, compared to the pre-suture removal levels, CDVA exhibited a significant improvement following selective suture removal (Table 2); CDVA improved in 69 eyes (58.5%), remained unchanged in 32 eyes (27.1%), and decreased in 17 eyes (14.4%). However, there was no significant alteration in CDVA upon complete suture removal (Table 2). Spherical equivalent refraction and mean keratometry significantly increased after selective suture removal and complete suture removal. Selective suture removal resulted in a significant reduction in refractive and keratometric astigmatism (Table 2). Compared to the outcomes of post-selective suture removal, refractive and keratometric astigmatism significantly increased after all sutures were removed (Table 2). Despite this increase, astigmatism was significantly lower following complete suture removal compared to the pre-suture removal values (Table 2).
Comparison of visual acuity, refraction, and keratometry before, during, and after suture removal following corneal transplantation for keratoconus.

p1: before suture removal initiation versus after selective suture removal completion. p2: before suture removal initiation versus after all suture removal. p3: after selective suture removal completion versus after all suture removal.
ANOVA, analysis of variance; CDVA, corrected distance visual acuity; D, diopters; LogMAR, logarithm of the minimum angle of resolution; UDVA, uncorrected distance visual acuity.
Figure 1 presents a comparison of keratometric astigmatism before and after each session of selective suture removal. A significant progressive decrease in astigmatism was observed until the third selective suture removal, with no further reduction observed thereafter. On average, selective suture removal resulted in a decrease of 2.40 D in keratometric astigmatism, ranging from a decrease of 10.0 D to an increase of 5.50 D. Compared to pre-suture removal values, 85 eyes (72.0%) exhibited lower keratometric astigmatism (mean difference, 3.63 ± 2.18 D; range, 1.0–10.0 D), while 14 eyes (11.9%) developed higher astigmatism (mean difference, 2.50 ± 1.17 D; range, 1.0–5.50 D) after selective suture removal. Nineteen eyes (16.1%) maintained their initial keratometric astigmatism (mean difference, 0.15 ± 0.46 D; range, −0.50 to +0.50 D). The procedure achieved keratometric astigmatism below 4 D in 70 eyes (59.3%).

Change in keratometric astigmatism after each session of selective suture removal for managing graft astigmatism in keratoconus eyes following corneal transplantation.
After complete suture removal, a mean increase of 1.46 D was observed in keratometric astigmatism compared to the results post-selective suture removal, ranging from a decrease of 5.50 D to an increase of 10.50 D. Twenty eyes (17.0%) exhibited less astigmatism (mean difference, 2.66 ± 1.42 D; range, 1.0–5.50 D), 64 eyes (54.2%) developed more astigmatism (mean difference, 3.41 ± 1.99 D; range, 1.0–10.50 D), and 34 eyes (28.8%) maintained their initial keratometric astigmatism (mean difference, −0.03 ± 0.43 D; range, −0.75 to +0.75 D).
Overall, keratometric astigmatism after complete suture removal was 0.87 D lower than before the initiation of selective suture removal, ranging from a decrease of 10.0 D to an increase of 8.50 D. Fifty-nine eyes (50.0%) exhibited less astigmatism (mean difference, 3.82 ± 2.15 D; range, 1.0 to 10.0 D), 39 eyes (33.1%) developed more astigmatism (mean difference, 3.24 ± 2.0 D; range, 1.0 to 8.50 D), and 20 eyes (16.9%) maintained their initial keratometric astigmatism (mean difference, 0.07 ± 0.46 D; range, −0.75 to +0.75 D). Keratometric astigmatism below 4 D was observed in 34 eyes (28.8%) after complete suture removal.
Axis and vectorial changes in keratometric astigmatism
Compared to pre-suture removal values, selective suture removal changed the axis of the steepest corneal meridian as follows: 0°–20° in 49.6%, 21°–40° in 18.6%, and 41°–90° in 31.8% of eyes. After complete suture removal, the corresponding figures were 43.5%, 18.3%, and 38.2%, respectively, as compared to pre-suture removal values.
The double-angled plots illustrated that the centroid shifted from 0.78 D @ 90° ± 6.58 D before selective suture removal to 0.94 D @ 78° ± 4.42 D post-procedure. Following complete suture removal, the centroid was 0.68 D @ 99° ± 6.17 D. Figure 2 shows that the clusters converged toward the center of the graph after selective suture removal, indicating a reduction in keratometric astigmatism. However, the data dispersed after complete suture removal, suggesting a diminishment in the effect of selective suture removal.
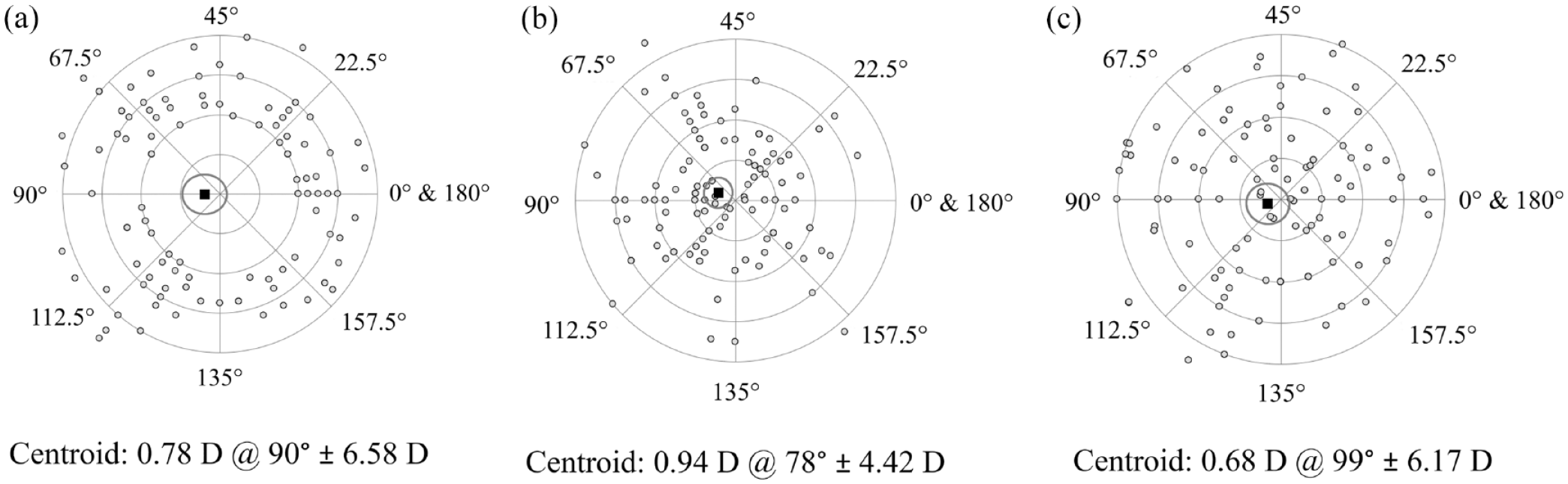
Double-angled plots of keratometric astigmatism measured before the initiation of suture removal (a), at the end of selective suture removal (b), and after complete suture removal (c) following corneal transplantation for keratoconus. Each concentric circle represents 2D astigmatism magnitude. The ellipses surrounding the centroids indicate the standard deviations of the x and y coordinates.
Evaluation of factors predicting changes in keratometric astigmatism after suture removal
We identified three distinct patterns based on changes in keratometric astigmatism following selective and complete suture removal (Figure 3). Pattern A, observed in 35 eyes (29.7%), exhibited astigmatism reduction by selective suture removal and further reduction or no change after complete suture removal. Pattern B, observed in 50 eyes (42.4%), showed a reduction in keratometric astigmatism after selective suture removal followed by an increase after complete suture removal. Pattern C, observed in 24 eyes (20.3%), demonstrated no change or an increase in keratometric astigmatism after selective and complete suture removal.

Change in keratometric astigmatism after selective suture removal and complete suture removal in keratoconus eyes following corneal transplantation.
We investigated potential factors predicting specific patterns after suture removal. Pattern A demonstrated a significant association with the DALK procedure (OR = 0.16, 95% confidence interval: 0.04–0.61, p = 0.003) and higher pre-suture removal astigmatism (OR = 2.89, 95% confidence interval: 1.59–5.02, p < 0.001). No association was found between different patterns of astigmatism change and patient sex (OR = 0.29, p = 0.09) or age (OR = 0.95, p = 0.21), stage of keratoconus (OR = 0.96, p = 0.97), donor quality (OR = 2.80, p = 0.25), graft size (OR = 5.32, p = 0.24), suturing technique (OR = 0.67, p = 0.48), interval to discontinuation of corticosteroids (OR = 1.49, p = 0.06), interval to initial suture removal (OR = 0.97, p = 0.65), number of selective suture removals (OR = 2.46, p = 0.19), or interval from final selective suture removal to complete suture removal (OR = 1.07, p = 0.11).
Discussion
Our study demonstrated the efficacy of selective suture removal in reducing post-keratoplasty astigmatism in 72% of eyes, without significant complications. Keratometric astigmatism decreased from 6.29 D before suture removal to 3.91 D at the end of the procedure while retaining the remaining sutures. These findings align with previous research outcomes.6–8 We adopted a strategy of removing one or two interrupted sutures per visit and reassessing graft astigmatism after 4–6 weeks. This approach allows the cornea time to adjust between visits, offering better control over the final astigmatism outcome compared to attempting multiple suture removals at once. However, our results indicated that the procedure had limited effectiveness in reducing graft astigmatism after more than three selective suture removals. Selective suture removal improved CDVA in 58.5% of eyes, indicating a more regular graft shape. We observed that selective removal of interrupted sutures increased graft steepness and induced a myopic shift, consistent with findings reported by other investigators. 6
Graft astigmatism unpredictably increased after complete suture removal in a significant number of our patients. We identified three distinct patterns of changes in astigmatism after selective and complete suture removal. The most favorable pattern, observed in 29.7% of cases, demonstrated a reduction in graft astigmatism after selective suture removal, followed by no change or further reduction after complete suture removal. In this subset of cases, suture tension emerged as either the primary contributor to graft astigmatism or acted in concert with non-suture factors.
The impact of selective suture removal significantly waned following complete suture removal in 42.4% of cases. In these instances, sutures, alongside non-suture factors, contributed to post-keratoplasty astigmatism. Subsequent to the selective removal of tightly placed interrupted sutures within this subgroup, the influence of sutures was nullified, with the appropriate tension of the remaining sutures compensating for other sources of graft astigmatism. Upon the removal of all sutures, non-suture factors became the predominant source of astigmatism.
Graft astigmatism persisted or paradoxically increased following suture removal in 20.3% of eyes. In these cases, sutures may not have been a significant contributor to graft astigmatism, suggesting the involvement of factors beyond suture tension that were unlikely to be rectified by selective suture removal. Another plausible explanation is the inaccurate identification of tightly placed interrupted sutures, leading to the inadvertent removal of a suture from the incorrect semi-meridian. The efficacy of selective suture removal hinges on the precise identification of sutures responsible for graft astigmatism. Keratometry’s capacity to depict corneal astigmatism as one flat and one steep meridian is inadequate for keratoplasty, given the presence of irregular astigmatism. Additionally, keratometry fails to specify which of the opposing sutures in the steep meridian exerts greater tension. Topography, on the other hand, can precisely pinpoint the steep semi-meridian and identify the tight suture for removal. 10 Studies examining the outcomes of selective suture removal with topographic guidance have reported an increase, rather than a decrease, in graft astigmatism in 18%–24% of cases, with no change observed in 19% of cases.7,10 These findings closely parallel our own results.
The present study investigated the factors influencing the alteration in astigmatism following suture removal. Our findings revealed that greater astigmatism prior to suture removal was indicative of more favorable outcomes following both selective and complete suture removal. Likewise, a previous study has noted a correlation between the change in graft astigmatism after selective suture removal and the level of graft astigmatism prior to suture removal. 8
On the contrary, other authors have demonstrated that higher levels of graft astigmatism are equally likely as lower levels to decrease to an acceptable level following selective interrupted suture removal. 7
The present study also found that the DALK procedure was associated with a greater reduction in graft astigmatism following both selective and complete suture removal compared to PK. To the best of our knowledge, a study comparing the change in astigmatism after selective suture removal in DALK versus PK has not been previously reported. The observed disparity between the two keratoplasty techniques may be attributed to differences in the healing response occurring at the graft-host junction. 11 In PK, wound healing occurs across three layers, including the Bowman layer, stroma, and Descemet membrane. 11 Conversely, in DALK, the healing response does not extend to the level of the Descemet membrane. 11 Consequently, when a tight suture is removed at the steep meridian of a PK graft, scarring between the recipient and donor Descemet membranes prevents excessive retraction of the graft. In contrast, a DALK graft retracts more easily due to the absence of scar formation at the Descemet membrane level, resulting in greater flattening at that meridian.
Investigation into additional factors, such as recipient sex, age at the time of keratoplasty, graft size, suturing technique, timing of suture removal, and the number of selective suture removals, did not reveal any association with a specific pattern of astigmatism change following suture removal. This finding is consistent with results from other studies.7,8 It has been suggested that retaining remaining sutures for an extended period after achieving an acceptable level of astigmatism may promote scar formation between the donor and recipient, potentially leading to less undesirable astigmatic change upon the removal of all sutures. However, the results of the present study indicate that the time from the final selective suture removal to suture removal completion did not influence the pattern of astigmatism change. This finding further supports the notion that a significant, unpredictable change in graft astigmatism can occur upon the removal of all sutures, even several years after keratoplasty. 4
Our study is limited by its retrospective design, which may introduce inherent limitations. Another limitation is the lack of power analysis for sample size calculation. Additionally, the utilization of manual keratometry to assess keratometric astigmatism may not provide optimal accuracy for evaluating post-keratoplasty irregular astigmatism. Corneal topography would offer a more precise means of delineating irregular astigmatic areas with steepening across the entire graft surface and is crucial in determining the suture to be removed during selective suture removal.
In summary, selective interrupted suture removal emerges as an effective strategy for reducing post-keratoplasty astigmatism and enhancing visual acuity, with minimal associated complications. This approach proves particularly advantageous in cases characterized by higher pre-suture removal astigmatism and in those undergoing DALK. The impact of selective suture removal remains significant until the remaining sutures are in place. In cases where graft astigmatism diminishes to an acceptable level following the procedure, it is prudent to leave intact sutures in situ indefinitely.