
Abstract
Background:
In young adults with rhegmatogenous retinal detachment, pneumatic retinopexy can be a cost-effective and minimally invasive highly effective method in suitable cases.
Objectives:
To evaluate the role of pneumatic retinopexy in the treatment of young adults with rhegmatogenous retinal detachment (RRD) and the factors that may affect the success of pneumatic retinopexy.
Design:
Retrospective study.
Methods:
The study included 67 eyes of 67 patients aged between 21 and 40 who underwent pneumatic retinopexy (PR) between January 2015 and June 2021 for primary RRD. We retrospectively analyzed the prognostic factors that may affect the success of PR, such as preoperative age, best corrected visual acuity, tear site, lens condition, and axial length.
Results:
PR was successful in 61.2% of the patients, whereas 38.8% required secondary surgery. Between the group that had a single surgery (Group 1) and the group that required secondary surgery (Group 2) the tear location, axial length, and volumes of gases used were statistically different (p = 0.04, p < 0.001, and p = 0.02, respectively). There was a significant difference in visual acuity before and after surgery in the group that was successful with a single surgery (Friedman χ2 = 40.051, p < 0.001). There was no significant difference between the two groups in terms of intraocular pressure (p > 0.05), and glaucoma was not observed in the postoperative period.
Conclusion:
Since it is a minimally invasive and cost-effective method that provides rapid visual rehabilitation, it can be considered as first-line therapy in young adults who are suitable for PR.
Keywords
Introduction
Rhegmatogenous retinal detachment (RRD) is a condition that can cause significant visual morbidity, which is one of the most common causes of vitreoretinal surgery. 1 Scleral buckling (SB), pars plana vitrectomy (PPV), and pneumatic retinopexy (PR) are the three main surgical methods currently used to treat RRD. 2 Approximately 10% of the RRD cases occur in young adults. Thick vitreous, partiality or absence of posterior vitreous detachment, and the presence of transparent lenses can cause difficulties in surgical approaches.3,4 In young patients with RRD, however, treatment with ab externo and minimally invasive approaches may be more appropriate to preserve clear lenses.5,6
PR for the treatment of RRD was first described by Dominguez in 1985 and by Hilton and Grizzard in 1986 and can be performed in an operating room, outpatient department, emergency room, or office as an outpatient procedure in normal office conditions without the need for sedation or general anesthesia.7,8 Compared to SB and PPV, PR is more advantageous in terms of being able to be performed in a short time with no preparation, faster visual rehabilitation, less invasiveness of the procedure, and a lower risk of complications and morbidity. 9
To date, there are few studies of PR in young adults with RRD. This study aimed to investigate the success of PR in young adults with RRD. Several preoperative and perioperative parameters were also examined to determine whether they could predict outcomes of PR.
Materials and methods
The study was retrospectively designed to include all individual eyes that received a PR for RRD in the retina department of Beyoglu Eye Training and Research Hospital in İstanbul between January 2015 and June 2021. Inclusion criteria included patients between 18 and 40 years old who underwent primary PR. As previously described in the literature, 10 these patients had a single retinal break or tear or a group of breaks within 2 and 8 h of the retina (between 8 and 4 o’clock). Patients were scheduled for a follow up visit within 6 months of the initial surgery. Patients with proliferative vitreoretinopathy exceeding Grade B, tears in the inferior retinal quadrant, a history of ocular surgery other than phacoemulsification (especially a history of previous retinal detachment surgery), and/or conditions that may affect retinal examinations, such as vitreous hemorrhage and cataracts, and were excluded from the study, as were mental and physically incapacitated patients who could not adapt to the head position.
The study included 67 subjects (50 men and 17 women) with the youngest being 21 years old and the oldest being 40. The mean time between presentation and PR application was 1.2 ± 0.12 days (with a range of 1–3 days). Age, gender, preoperative best corrected visual acuity (BCVA), intraocular pressure (IOP), lens condition, axial length, number of tears, tear location, tear width, detachment site, macular involvement, tamponade material used, and postoperative laser status were noted. Additionally, BCVA, intraocular pressure, and surgical intervention in the postoperative first day, first week, first month, third month, and sixth month were compared. The follow-up period was the time since the last operation (e.g. if the second surgery was performed, the duration of the follow-up was the time since the second surgery).
According to the results of a previous study on PR, the procedure was considered unsuccessful when sufficient gas volume was completely reduced in the presence of persistent subretinal fluid that prevented effective laser photocoagulation 4 weeks after PR. 11 Therefore, for the subgroup analysis, group 1 was comprised of the PR responders who achieved anatomical success in a single operation, and group 2 included the PR non-responders who required a second surgical intervention because the first attempt was unsuccessful.
The BCVA was measured using the Snellen chart and was then converted to logarithm of the minimum angle of resolution (logMAR) for statistical analysis.
Surgery
After obtaining consent, all patients underwent the same method of PR in sterile conditions and under topical anesthesia. Before the gas injection, an anterior chamber paracentesis of 0.1–0.2 cm3 was performed under a microscope with the patient lying down, and then tamponade material such as perfluoropropane (C3F8) or sulfur hexafluoride (SF6) was injected to the eye with a 30-G injector from the pars plana (at a 3.5–4 mm distance from the limbus) into the vitreous cavity. Afterward, the patient was placed in an appropriate head position. In the postoperative period, the surgery site was monitored daily for 3 days, then weekly for a month to determine its success. In unsuccessful cases, a second PR or other vitreoretinal surgery was performed according to the clinical condition of the patients. Since there was no cryotherapy device in our hospital, the barrage laser photocoagulation was applied to all patients around the tear or within 360° of the retinal periphery at 3 day postoperation.
Statistical analysis
Statistics for continuous variables were expressed as mean ± standard deviation for those with normal distribution. Median (minimum–maximum) values were used for those variables outside a normal distribution. Descriptive statistics for categorical variables were given as numbers and percentages.
The conformity of continuous variables to normal distribution was evaluated using the Shapiro–Wilk test. According to these results, the differences between the two independent groups were examined using the t-test or the Mann–Whitney U-test. In the evaluation of repeated measurements, the conformity to the normal distribution was examined and a Friedman test was performed in accordance with the distribution structure. Pairwise comparisons were made using the Wilcoxon paired-sample test, and the Bonferroni correction was used. Relationships between categorical variables were examined with chi-square tests. Additionally, multivariate logistic regression analysis was performed to determine the relationship between surgical success and preoperative presentations.
Statistical analyses were performed using IBM SPSS Statistics (Version 27). The resulting 95% confidence level and p ⩽ 0.05 were considered statistically significant.
Results
One hundred eighty-nine patients were screened, and 67 eyes of 67 patients who came to regular control meetings, whose records were kept and who met the inclusion criteria were included in the study. The ages of the patients in this study ranged from 21 to 40, with a median age of 35. The summarized clinical data of the study group are shown in Table 1. The patient’s BCVA ranged from 0 logMAR to 3.1 logMAR, with a median of 0.7 logMAR at presentation. Before treatment, 85.1% of the patients were phakic, and 74.6% had a single tear. Thirteen patients (19.4%) had posterior vitreous detachment (PVD) of which four (30.8%) patients had high myopia (axial length > 26 mm) and nine patients (69.2%) had a history of trauma. The tear location was mostly (53.7%) in the superior region. Lattice degeneration was present in 18 of the patients (26.9%), and 10 (55.6%) of them had accompanying tears.
Demographic and clinical data of study group.
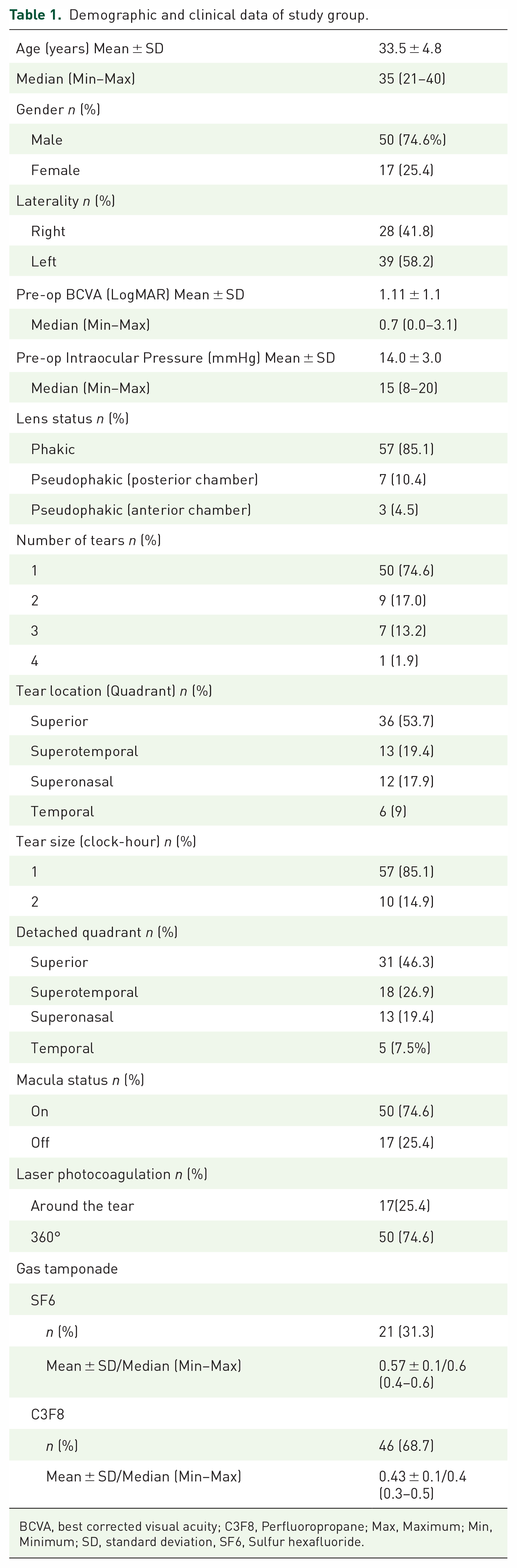
BCVA, best corrected visual acuity; C3F8, Perfluoropropane; Max, Maximum; Min, Minimum; SD, standard deviation, SF6, Sulfur hexafluoride.
During the PR procedure, perfluoropropane (C3F8) was applied to 46 eyes (68.7%), and sulfur hexafluoride (SF6) was applied to 21 eyes (31.3%). The average amount of gas used was 0.43 ± 0.1 mL for C3F8 and 0.57 ± 0.1 for SF6 mL.
While 61.2% of patients who underwent PR experienced successful surgeries at one time, 38.8% of the surgeries failed. For unsuccessful surgeries, the second intervention was performed (shown in Table 2). The type of the second procedure was determined by the patient’s clinical condition. When the characteristics of patients who achieved anatomical success after PR with a single intervention were compared with those who had a second surgery in which PR was insufficient. It was found that the tear location, its axial length, and volumes of the gases used were statistically different (p = 0.04, p < 0.001, p = 0.02, respectively; Table 3). Those with tears in the superior quadrant and an adequate amount of gas used and those without longer axial lengths were associated with better outcomes.
Surgical procedures applied in case of unsuccessful PR (n: 26).

PPV, pars plana vitrectomy; PR, pneumatic retinopexy; SB, scleral buckling.
Comparison of parameters between patients who were successful in a single surgery and patients who had a second surgery.
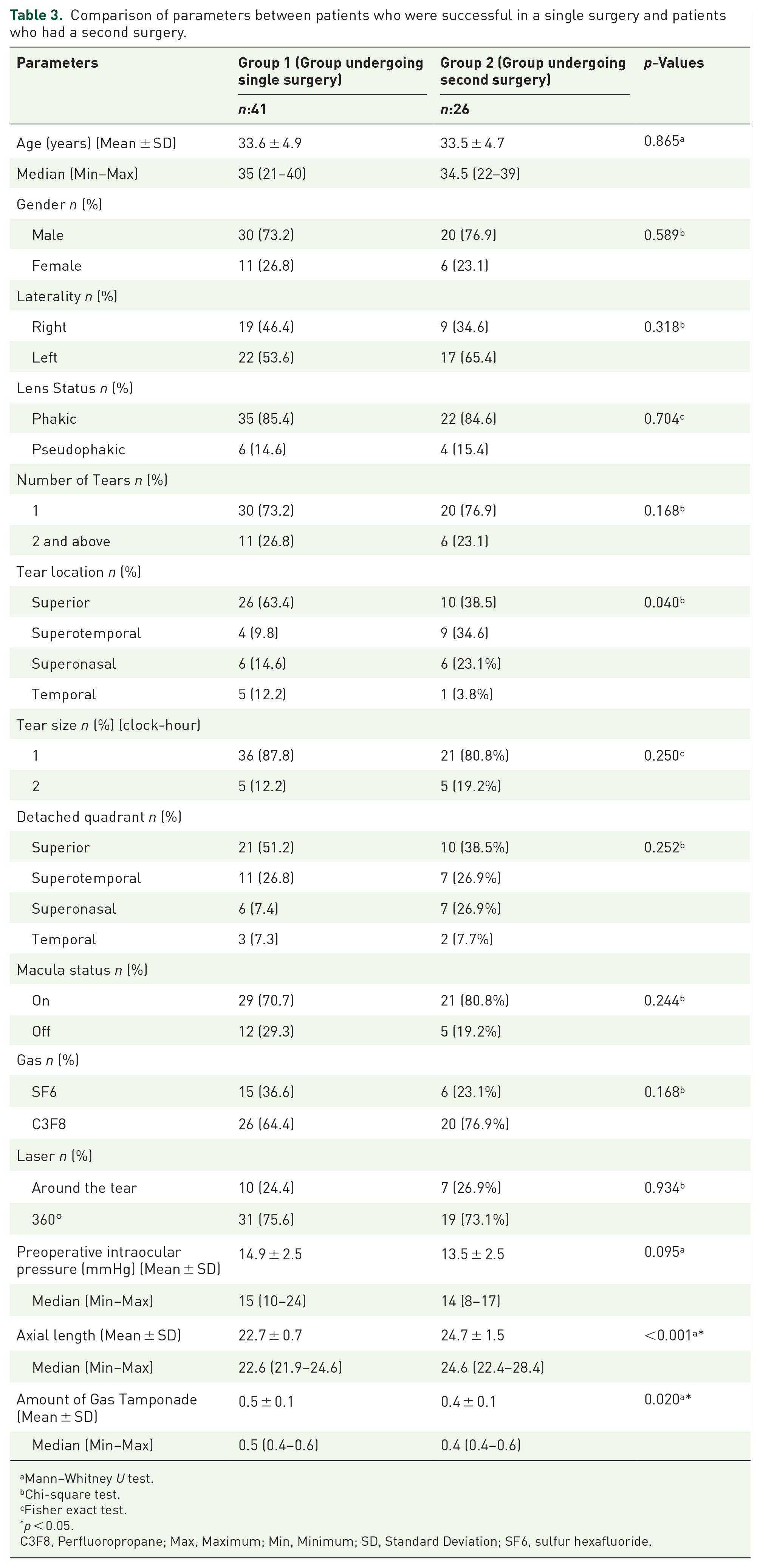
Mann–Whitney U test.
Chi-square test.
Fisher exact test.
p < 0.05.
C3F8, Perfluoropropane; Max, Maximum; Min, Minimum; SD, Standard Deviation; SF6, sulfur hexafluoride.
The distribution of visual acuity before and after the surgical procedure in the patients included in the study, both those who had a single surgery (PR responders) and those who had a second surgery (PR non-responders), are given in Figure 1. All eyes (100%) had complete retinal attachment at the final follow-up appointment.

Comparison of visual acuity before and after surgery in Group 1 (PR responders) and Group 2 (PR non-responders).
Repeated measurements of visual acuity before and after surgery were examined, and a significant difference was found between the measurements among the PR responders (Group 1) (Friedman χ2 = 40.051, p < 0.001).
A significant difference was observed between the groups in terms of BCVA at 1, 3, and 6 months postoperation (p = 0.036, p = 0.001, p < 0.001, respectively; Table 4).
Best corrected visual acuity comparison of Group 1 and Group 2.

Mann–Whitney U test.
p < 0.05.
logMAR, Logarithm of the Minimum Angle of Resolution; Max, Maximum; Min, Minimum; SD, standard deviation.
Regarding intraocular pressure, there was no statistically significant difference between the groups (p > 0.05, Table 5). In addition, there was no glaucoma developed in any patient during the follow-up period.
Intraocular pressure comparison of Group 1 and Group 2.

Mann–Whitney U test.
t Test.
Max, maximum; Min, minimum; SD, standard deviation.
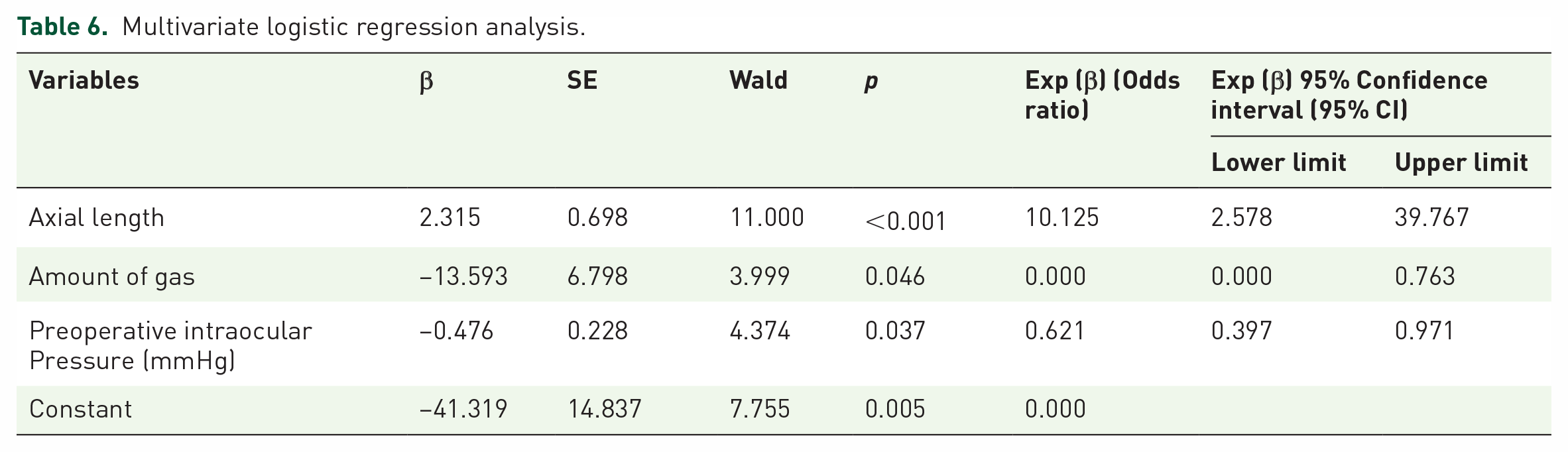
According to the results of the logistic regression analysis depicted in Table 6, the relationship between axial length, amount of gas, preoperative intraocular pressure and the surgical success rate is stable (p < 0.05). When the axial length increases by one unit, the risk of surgical failure increases by 10% (p < 0.001), and when the preoperative intraocular pressure value increases by one unit, the risk of failure decreases by 37.9% (p = 0.037).
Multivariate logistic regression analysis.
Complications
Of 26 eyes that failed after a single PR surgery, 30.8% (or eight eyes) presented new or missing retinal tears, 7.7% (two eyes) had proliferative vitreoretinopathy (PVR), and the rest had no identifiable cause. The whole study group had no endophthalmitis. We did not observe cataract formation in the patients’ follow-up period.
Discussion
We evaluated the factors affecting the results and success rates of PR in young adults. For this study, the anatomical success rate of a single operation was 61.2% in patients who underwent PR due to primary RRD. Additionally, five patients who failed PR underwent a second PR and achieved complete anatomical success. Thus, this success rate increased to 68.7% for young adults in accordance with previous studies in the literature ranging from 45% to 93.3% for all age groups.12 –14
In studies conducted since 2015, the success rate of PR is higher than in previous studies (82% vs 59%). 15 The reasons for such variation have yet to be determined. However, the success rate of our study is lower than the studies conducted in recent years. This may be due to the fact that we included young adults in our patient group, and they exhibited 19.4% PVD. In addition, young patients might find it difficult to maintain a fixed head position for a longer period of time.
Using the chandelier-assisted PR for RRD repair technique initially described by Habib et al. 16 in 12 young adults, the success rate was 91.7% with a single surgery and 100% with a second surgery. Habib et al. mentioned this technique aims to detect small, overlooked tears and prevent intraoperative complications such as lens injury. Their single success rate was better than our study (91.7% vs 61.2%, respectively). On the one hand, the small, overlooked peripheral tears might affect our success rate. On the other, the small number of patients, one of the study’s limitations, may contribute to its higher success rate. Additionally, the high myopic and pseudophakic patients included in our study may have caused our success rate to be lower than Habib et al.’s.
PR is a safe, minimally invasive, relatively easy-to-learn, cost-effective procedure for repairing primary RRD. It is expected that PR can restore 40% of all RRDs. 17
In a prospective randomized, controlled study (PIVOT) by Hillier et al. 18 , patients undergoing PR for primary RRD achieved superior visual acuity, less vertical metamorphopsia, and reduced morbidity compared with those undergoing primer PPV. However, there were several comprehensive studies that reported that better anatomical success rates for SB and PPV in single surgery.12,19
Although we did not evaluate displacement in our study, there are valuable studies recently published on this subject. Relatively high rates of retinal displacement following PPV in comparison to PR have been reported.15,20 –22 Muni et al. 22 considered photoreceptor integrity between PR and PPV at 12 months postoperative on spectral-domain-optical coherence tomography (SD-OCT) in a subset of patients of the PIVOT study. In 3 mm (foveal) and 6 mm (foveal and nonfoveal) scans, the ellipsoid zone discontinuity and external limiting membrane discontinuity were found to be significantly higher in patients who underwent PPV compared to PR patients. As a result, PR was found to be superior to PPV in terms of photoreceptor integrity and the absence of retinal displacement.
In addition, the status of the posterior vitreous may affect the success rate of retinal detachment surgery in young adults. 23 Chen and Hwang 24 suggested that in young patients without PVD, the intravitreal air bubble is properly situated, and there is little traction on the other parts of the retina. Thus, there is little chance of the formation of a new break. In patients with PVD, however, residual vitreous traction may occur in some focal equatorial or peripheral parts of the retina, and new break formation may develop accordingly. Similarly, PR failed on the first attempt in 61.5% of eyes with PVD in our study.
However, scleral buckle is an effective treatment method in young patients with retinal detachment without PVD. Noori et al. 25 had a success rate of 91.1% in patients who underwent a scleral buckle due to primary retinal detachment without PVD.
The relatively low success of PR in one attempt was attributed to factors such as pseudophakia, aphakia, wide RRD coverage, increased tears production, vitreous hemorrhage, and tamponade used.26,27
In the current study, there was no statistical difference in the lens status, the number of tears, or the extent of retinal detachment in the 26 (38.8%) cases requiring a second intervention compared to the group that was successful in the first attempt. None of the patients had a vitreous hemorrhage. On the other hand, axial length and the amount of gas used were the main factors affecting the success of a single PR. While no significant difference was observed in terms of which gas was used in our study, the amount of gas used was found to be significantly higher in the group that had a single surgery compared to the group that had a second surgery. For PR to be effective, the gas used must be large enough to cover the tear. In the group requiring a second surgery, the axial length was significantly higher than in the single surgery group. Also, based on the multivariate logistic regression, when the axial length increased by one unit, the risk of failure of the surgery increased by 10%. We think that the underlying cause may be insufficient gas with a longer axial length rather than overlooked or new tears.
The largest case series examining PR included 422 eyes with a single-operation success rate of 60.7%. In this study, factors such as pseudophakia/aphakia and number of retinal tears, as well as being male, adversely affected the result. 28 However, we did not find any correlation between complete failure of PR and gender. Similarly, Rahat et al. 29 stated that the gender distribution did not affect PR success rates.
The literature reports no association between PR results and duration of detachment, macular status, or the number of retinal fractures.28,30 Our study was consistent with these studies regarding tear location, macular condition, and detached quadrant.
In PR, laser photocoagulation can only be applied around the tear or 360 between the vitreous base and the ora serrata. Peripheral retinopexy can be performed before or after gas injection. It has been reported that this application significantly increases the success rate of a single surgery when performed in 360. 26 The laser photocoagulation state of the eye was not a statistically significant factor in determining the effectiveness of the PR in our study.
Patients with failed PR, the procedure had been repeated or surgically repaired with a scleral buckle, PPV, or both in our study. Notably, preoperative BCVA was similar in the single and second surgery groups, with a trend for improved postoperative vision in both groups. However, there was a statistically significant increase in visual acuity from the first month postoperative in the group who enjoyed reattachment with the first PR. Postoperative visual gains may be limited because detachment after an unsuccessful PR extends until the second operation. Another possible cause of poor visual acuity may be surgical trauma to the retina. Therefore, an unsuccessful PR may be an important indicator of poor postoperative visual outcomes.
Mougharbel et al. 6 showed that PR was not related to permanent changes in lens transparency at the 24-month follow-up in their study. Similarly, we did not observe increased nuclear opacities in phakic eyes. At baseline, there was no significant difference in mean IOP between the successful and unsuccessful groups, and compared with baseline, the mean IOP remained statistically stable in both groups during the follow-up appointments in our study.
Also, we did not encounter any complications, other than recurrence, in our patients. However, in a previously published meta-analysis study comparing PPV and SB, PPV was associated with a higher risk of cataract and iatrogenic breaks, and SB was associated with a higher risk of choroidal hemorrhage, choroidal detachment, and residual subretinal fluid. 31
One limitation of this study is that it was conducted in a retrospective fashion. Additionally, the efficacy of primary PPV and/or scleral buckle in young adults cannot be compared with PR. Another limitation was the small sample size.
In conclusion, PR can be considered to be the first line of treatment in young adults, as it is a minimally invasive and cost-effective method that provides rapid visual rehabilitation when used in appropriate cases. The presence of PVD is one of the main factors influencing successful treatment of RRD. Patient compliance should be evaluated even if the patient’s eye is suitable for PR. If the patient is non-compliant and cannot maintain the head position, the chances of success may decrease. In cases of recurrence, the chance of success can be increased with a timely second surgery. Additionally, to avoid a second surgery, injecting the appropriate amount of gas to increase the likelihood of first-treatment success can be essential. A prospective randomized study with more patients may be required to verify our current findings and enhance understanding of the indications and outcomes of PR.