
Abstract
Introduction
Pneumatic retinopexy is a minimally invasive procedure used to repair selected cases of rhegmatogenous retinal detachment (RRD). While generally safe, complications may occur, including misplacement of the intraocular gas bubble. A rare complication is the entrapment of gas in the canal of Petit, which may present as a characteristic “donut” or “sausage-shaped” sign adjacent to the lens. The canal of Petit is a potential space between the postequatorial zonules and the anterior hyaloid face. Prompt recognition and appropriate management are crucial to prevent unnecessary surgical intervention. To our knowledge, this is the first reported case of gas entrapment in the canal of Petit following pneumatic retinopexy documented with ultra-widefield color imaging, including detailed sequential imaging demonstrating posterior migration of the gas bubble into the vitreous cavity with strict prone face-down positioning alone. This case underscores the value of noninvasive management and highlights the role of imaging in guiding clinical decision-making.
Case Report
A 49-year-old woman presented with a new visual field defect in her left eye, with no significant prior ocular history, including surgery, trauma, or significant refractive error. Examination revealed a macula-on RRD extending from 8:30 to 12 o’clock, with a retinal tear at 9 o’clock and an additional tear at 8 o’clock located in the attached retina. No posterior vitreous detachment (PVD) was detected on slitlamp examination on optical coherence tomography. Laser retinopexy was performed to treat the tear in the attached retina before gas injection.
Pneumatic retinopexy was performed, consisting of a 0.2 mL anterior chamber paracentesis, followed by intravitreal (IVT) injection of 0.6 mL sulfur hexafluoride (SF6) gas and a repeat 0.1 mL anterior chamber paracentesis under sterile conditions. The injection was performed in the superotemporal quadrant, 4 mm posterior to the limbus, directed toward the optic disc while the patient maintained inferonasal gaze. Immediately after injection, the gas bubble appeared elongated and “donut-shaped,” encircling the lens in a pattern consistent with entrapment in the canal of Petit (Figure 1). The patient was instructed to maintain strict face-down positioning at approximately 70 to 90 degrees to facilitate posterior migration of the entrapped gas into the vitreous cavity. At the 15-minute mark, the gas bubble began to change configuration, suggesting posterior migration (Figure 2). By 50 minutes, complete migration into the vitreous cavity was confirmed on sequential ultra-widefield imaging (Figure 3). The patient was advised to maintain face-down positioning for 24 hours, followed by left lateral positioning.
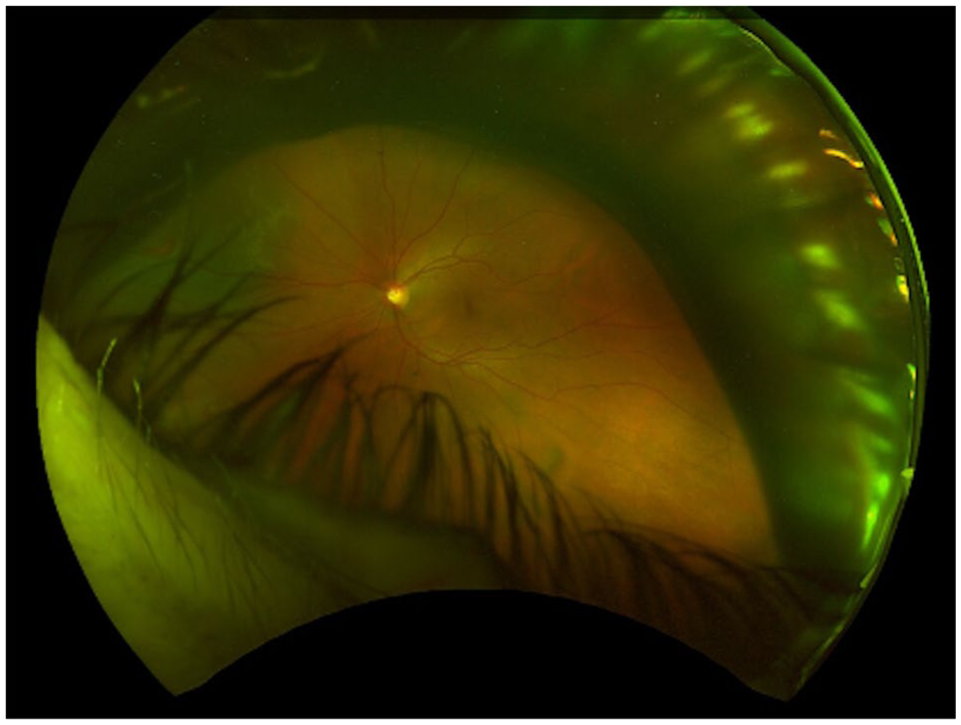
Ultra-widefield image obtained immediately after intravitreal injection of 0.6 mL SF₆ gas, showing an incomplete “donut-shaped” gas bubble encircling the posterior aspect of the lens. This configuration is consistent with gas entrapment in the canal of Petit, a potential space between the posterior lens capsule and the anterior hyaloid face. The associated rhegmatogenous retinal detachment is visualized behind the gas bubble, with an open horseshoe tear located in the superonasal quadrant.
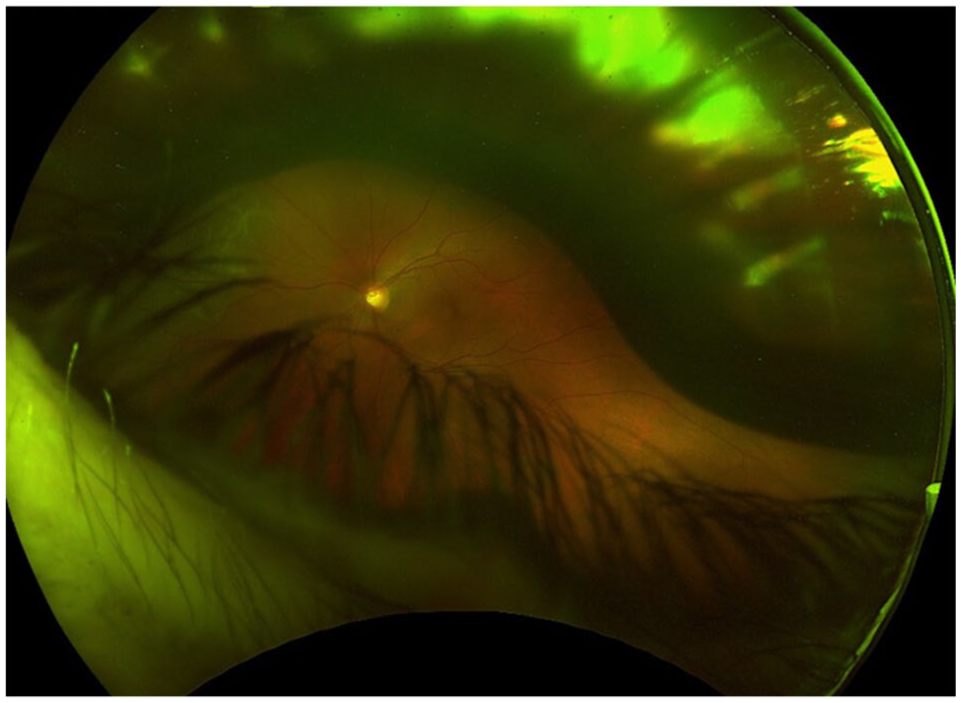
Ultra-widefield image obtained 15 minutes after face-down prone positioning, demonstrating partial posterior migration of the gas bubble from the canal of Petit toward the vitreous cavity. The associated rhegmatogenous retinal detachment is visualized behind the gas bubble.
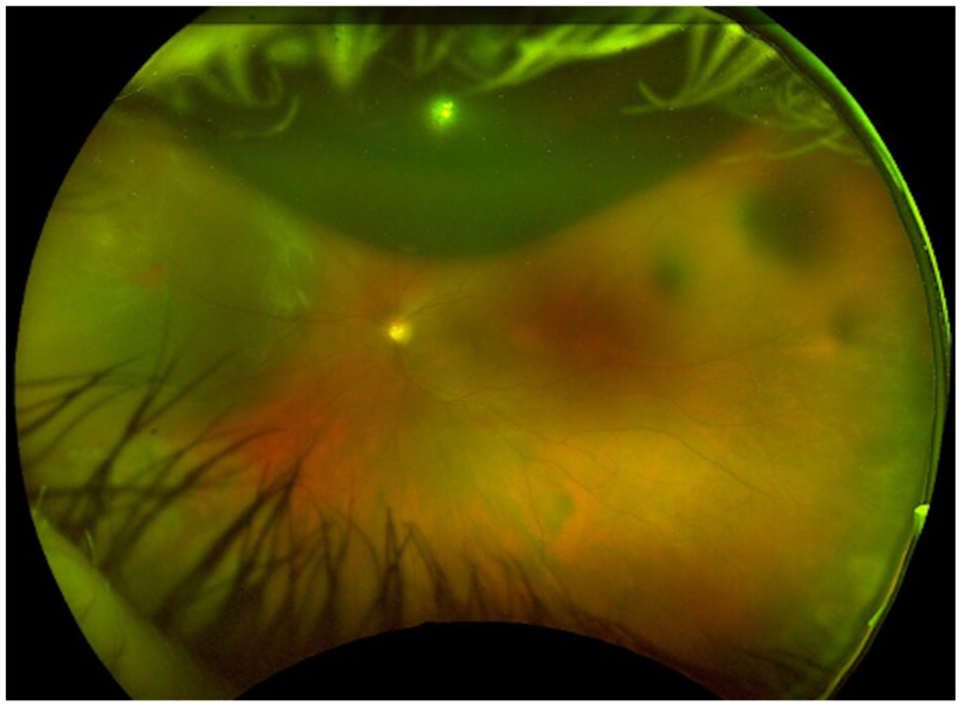
Ultra-widefield image obtained 50 minutes after initiation of prone face-down positioning, demonstrating complete posterior migration of the gas bubble into the vitreous cavity. The prior “donut-shaped” configuration is no longer present, confirming resolution of gas entrapment in the canal of Petit. The associated rhegmatogenous retinal detachment remains visible behind the gas bubble.
At the 2-day follow-up, examination showed that the retina had fully reattached, and the gas bubble was visualized within the vitreous cavity (Figure 4). Laser retinopexy was then performed to treat the tear in the previously detached retina. The visual acuity of the patient remained stable, and the presenting visual field defect resolved completely.
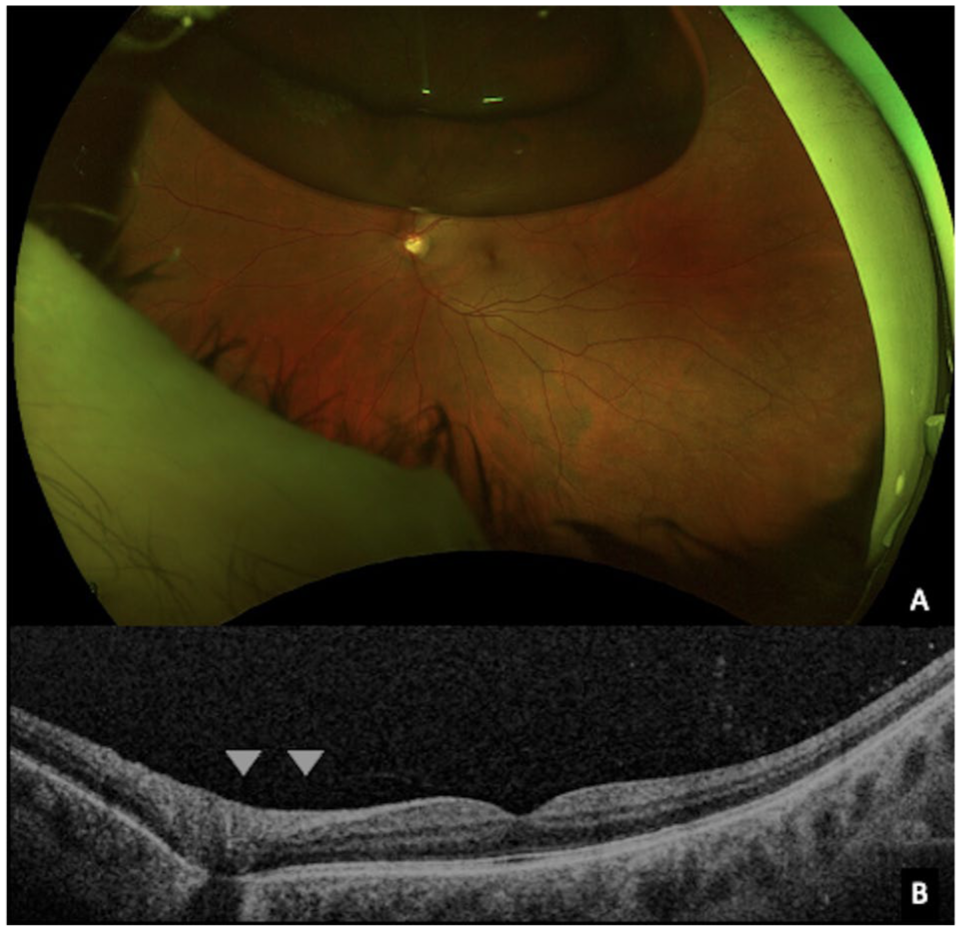
Follow-up ultra-widefield imaging conducted 2 days after the procedure demonstrates (A) complete retinal reattachment, with the gas bubble appropriately positioned in the vitreous cavity. (B) Optical coherence tomography of the left macula demonstrating persistent attachment of the posterior hyaloid at the area of Martegiani (arrowheads), confirming the absence of posterior vitreous detachment.
Conclusions
Gas entrapment in the canal of Petit is an uncommon but clinically distinctive complication of pneumatic retinopexy. This misdirection results in a characteristic “donut”-shaped gas configuration adjacent to the lens, as observed in our patient. 1 In the present case, sequential ultra-widefield imaging demonstrated posterior migration of the entrapped gas into the vitreous cavity within 50 minutes of strict prone face-down positioning, consistent with the principles described by Hilton et al. 2 Once repositioned in the vitreous cavity, the gas bubble effectively tamponaded the retinal breaks, allowing for complete retinal reattachment. To our knowledge, this is the first reported case of gas entrapment in the canal of Petit during pneumatic retinopexy, documented with sequential imaging demonstrating resolution through positioning alone.
In 1726, the French anatomist and surgeon Jean Louis Petit first delineated this anatomical space. 3 His pioneering work involved injecting air into a dissected eye through a slender tube, revealing a circumferential canal around the lens that appeared as a long, silver tube when distended. Notably, when gas is inadvertently injected anteriorly during pneumatic retinopexy, it may expand the potential space between the anterior hyaloid face and the posterior fibers of the equatorial zonules.3,4 This phenomenon mirrors the mechanical principles demonstrated in Petit’s seminal experiment, thereby enhancing our understanding of the dynamics involved in this rare complication of pneumatic retinopexy.
Steinmetz et al reported 2 cases of gas entrapment in the canal of Petit after pneumatic retinopexy, both of which were managed by removing the trapped gas using a 30-gauge needle inserted through the pars plana and vented to the atmosphere. The authors suggested that this complication may result from inadequate penetration of the anterior hyaloid face by the injecting needle. 5 They further proposed several factors that may increase the risk of gas entrapment in the canal of Petit, including a dull needle tip, a rigid anterior hyaloid face, and partial withdrawal of the needle after insertion to prevent the formation of multiple small gas bubbles (“fish eggs”).
The authors concur with the mechanisms proposed by Steinmetz et al. 5 However, in our experience, this complication may occur more frequently in patients without PVD, as observed in our case. In the absence of PVD, the anterior hyaloid face forms a taut, convex surface that can deflect the gas anteriorly during injection. If the needle does not adequately penetrate this membrane, the injected gas may dissect into the canal of Petit, forming a pressurized, encapsulated gas bubble adjacent to the lens that conforms to the shape of the canal. Strict face-down positioning reorients the buoyant force of the gas against the anterior hyaloid face. As gas expands and pressure increases, it may eventually overcome this barrier and migrate into the mid-vitreous cavity, where it can effectively tamponade the retinal break. Therefore, although needle retraction may prevent the formation of multiple small gas bubbles (“fish eggs”), caution is warranted when employing this technique in patients without a complete PVD.
While this complication may raise concerns about treatment failure or the need for surgical intervention, our case demonstrates that conservative management with strict face-down positioning can effectively redirect the gas bubble into the vitreous cavity by harnessing its buoyant properties. Once repositioned, the gas bubble functioned as intended to tamponade the retinal breaks, allowing for complete retinal reattachment. With appropriate positioning, the risk of potential complications associated with gas entrapment in the canal of Petit, such as retinal dialysis, lens dislocation, or cataract, can be significantly reduced. Therefore, premature surgical intervention may be unnecessary and could expose the patient to additional risks associated with more invasive procedures.
Additionally, attempted evacuation of the gas using a 30-gauge needle in the office setting may lead to new breaks due to vitreous traction. Initial observation with strict patient positioning is recommended before considering further surgical intervention. In cases where gas migration does not occur promptly, a trial of up to 48 hours of strict prone positioning with close daily monitoring may be reasonable, provided the retinal detachment remains stable. If posterior migration of the gas does not occur during this period, or if the clinical condition worsens, escalation to surgical management, such as pars plana vitrectomy, should be considered.
Herein, we demonstrate, using fundus imaging, that posterior migration of entrapped gas can occur as a result of buoyant forces alone. However, it remains unclear whether other factors, such as gas expansion, contribute to the breakthrough into the vitreous cavity. Further research is needed to fully understand the mechanisms underlying this process.
In conclusion, prompt recognition of gas entrapment in the canal of Petit during the immediate post-injection assessment of pneumatic retinopexy is essential, as untreated cases may lead to lens- and retina-related complications. Our case represents a valuable contribution to the literature by demonstrating, through sequential ultra-widefield imaging, that conservative management with strict prone face-down positioning can successfully resolve this condition without the need for surgical intervention.
Imaging played a key role in confirming the diagnosis and monitoring the treatment response. When identified early and managed appropriately, this approach can lead to favorable anatomic and visual outcomes.
Footnotes
Authors’ Note
Drs. Tang and Cruz-Pimentel contributed equally to this manuscript and share co-first authorship. All authors attest that they meet the current ICMJE criteria for authorship.
Ethical Approval
This case report was conducted in accordance with the Declaration of Helsinki. Institutional review board/research ethics board approval was not required for a single-patient case report without identifiable information.
Statement of Informed Consent
Informed consent, including permission for publication of all photographs and images included herein, was obtained before the procedure was performed.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.