
Abstract
Background:
Cataract usually occurs due to age and diabetes, but the mechanisms of cataract formation have not yet been fully elucidated. In this study, the relationship between cataract and oxidative stress was evaluated by examining the aqueous humor reflecting lens metabolism.
Objective:
In this study, the effect of oxidative stress on the etiopathogenesis of cataract was investigated through the total oxidant status (TOS), total antioxidant status (TAS), oxidative stress index (OSI), and arylesterase (ARE) levels in aqueous humor samples of patients with cataract.
Design:
A prospective cohort study.
Methods:
This study was conducted on patients who were scheduled for cataract surgery between June 2020 and March 2021. The patients were divided into four groups according to their cataract density as grades 1, 2, 3, and 4. TOS, TAS, and ARE levels of aqueous humor samples were measured spectrophotometrically, and comparisons were made between groups.
Results:
A total of 100 eyes of 100 patients were included in this study. TAS levels were found significantly higher in the grade 2 group compared with the grade 4 group (p = 0.006). In addition, a significant negative correlation was present between cataract grade and TAS level (r = −0.237; p = 0.018). There was no significant difference between diabetic and nondiabetic patients in terms of TAS, TOS, OSI, and ARE levels.
Conclusion:
The aqueous humor of patients with a high degree of cataract is characterized by low antioxidant capacity. Decreased antioxidant capacity has a role in cataract formation and progression.
Introduction
Cataract is one of the leading causes of visual impairment and treatable blindness worldwide and is simply defined as the loss of transparency of the crystalline lens.1,2 The most common symptoms are visual impairment, decreased contrast sensitivity, color disturbance, and glare . Some of the most common causes of cataracts in adults are advanced age, diabetes mellitus (DM), steroid usage, family history, and trauma. 3 DM is the leading chronic disease affecting the cataract process. There are numerous studies that assessed the relationship between cataract formation and DM. These studies have shown that cataract formation has early onset and is more progressive in DM patients as against the nondiabetic patients.4,5
As a multifactorial disease, the cataract formation mechanism is under debate. 6 Among various causes, oxidative stress is thought to play a crucial role in the molecular mechanism of cataract formation. 7 Oxidative stress takes place when reactive compounds such as superoxide anion, hydroxyl radicals, and hydrogen peroxide cannot be counteracted by antioxidant enzymes such as catalase, superoxide dismutase (SOD), and glutathione peroxidase (GPx). Increased reactive oxygen derivatives affect nucleic acids, proteins, and lipids in the lens leading to mutations and cell apoptosis. 3 Therefore, in addition to the development of cataract, oxidative stress also has a vital role in the formation and progression of various ocular diseases such as diabetic retinopathy, glaucoma, age-related macular degeneration, autoimmune uveitis, and pseudoexfoliation syndrome. 8
Among various parameters, the total oxidant status (TOS) and total antioxidant status (TAS) are reliable markers used to evaluate oxidative stress status. It has been reported that the measurement of only one or more of the oxidant molecules together does not fully reflect the total oxidant levels of the patients and that the oxidant molecules have additive effects upon each other. Therefore, the measurement of TOS levels is more accurate, as it is not practical to measure individual oxidant molecules, which is time-consuming, labor-intensive, and resource-wasting. It has also been indicated that TAS level measurement reflects the total antioxidant capacity of all antioxidant molecules.9,10 Paraoxonase 1 (PON1) and arylesterase (ARE) are enzymes in the esterase group encoded by the same gene and have similar active centers. PON1’s antioxidant functions are due to its capacity to protect low-density lipoprotein (LDL) from oxidation and neutralize other radicals, including hydrogen peroxide. Besides, the common properties of PON1 and ARE to hydrolyze organophosphates, aryl, and alkyl halides are well known. Although it is known that PON1 shows polymorphic changes, ARE enzyme is accepted as the indicator of the main protein that does not reveal polymorphic genetic modification. 11
In this study, we aimed to investigate the effect of oxidative damage on the etiopathogenesis of cataract by examining the humor aqueous TAS, TOS, oxidative stress index (OSI), and ARE levels of cataract patients.
Methods
Patient selection
Patients admitted to Kırıkkale University Faculty of Medicine, Department of Ophthalmology between June 2020 and March 2021 who diagnosed with cataract and recommended surgical treatment were included in the study. A total of 45 patients who were non-DM at the time of admission were stated as group 1, and 55 patients with DM were noted as group 2. Detailed anamnesis was taken from the patients. Their systemic and ocular diseases and the drugs they used were recorded. Visual acuity, intraocular pressure measurement with air-puff tonometry, biomicroscopic anterior segment, and fundus inspections were performed for patients’ eye examinations. Cataract classification and grading were performed according to the Age-Related Eye Disease Study (AREDS) clinical lens grading system, with dilated ophthalmological examination and images taken in the operating room. 12 According to the cataract type, the patients were divided into nuclear, posterior subcapsular, mixed, and graded as grades 2, 3, and 4. There was no pure cortical cataract or grade 1 cataract patient. The patients were grouped as mature and immature cataract according to their cataract maturity.
Patients with any thyroid, kidney, and liver dysfunction, a history of smoking and alcohol use within the last year, patients with a history of acute infection, acute myocardial infarction, ocular surgery, and patients with traumatic and toxic cataracts were not included in the study. The procedures to be performed were explained to the patients participating in the study, and informed consent forms were obtained from all patients.
Collection and storage of samples
At the beginning of standard cataract surgery, approximately 0.1 cc aqueous humor was aspirated from the anterior chamber with a 27-gauge cannula connected to an insulin syringe through the corneal side entrance, which is routinely applied with an MVR (microvitreoretinal) blade, and was poured into the Eppendorf microtube. Samples were stored at −80°C until analysis. Aqueous humor TOS, TAS levels, and ARE enzyme activities (Rel Assay Diagnostics kit, Baran Medikal, Ankara, Turkey) were measured using an automated measurement method with Mindray BS400 autoanalyzer.
TOS measurement
In the new method, oxidants present in the sample oxidized the ferrous ion-o-dianisidine complex to ferric ion. The oxidation reaction was enhanced by glycerol molecules abundantly present in the reaction medium. The ferric ion produced a colored complex with xylenol orange in an acidic medium. The color intensity, which could be measured spectrophotometrically, was related to the total amount of oxidant molecules present in the sample. The assay was calibrated with hydrogen peroxide, and the results were expressed in terms of micromolar hydrogen peroxide equivalent per liter (μmol H2O2 equivalent/l). 10
TAS measurement
The novel automated method is based on the bleaching of characteristic color of a more stable ABTS (2,2’-Azino-bis(3-ethylbenzothiazoline-6-sulfonic acid)) radical cation by antioxidants. The assay has excellent precision values, which are lower than 3%. The results were expressed as mmol Trolox equivalent/l. 13
Oxidative stress index
The ratio of TOS to TAS was accepted as OSI. For calculation, the resulting TAS unit was converted to μmol/l, and the OSI value was calculated according to the formula 14

ARE enzyme activity measurement
Phenylacetate was used as the substrate to measure ARE activity. The enzymatic activity was calculated as 1310 M−1 cm−1 from the molar absorption coefficient of the produced phenol. One unit of ARE activity was defined as 1 µmol of phenol produced per minute under the above conditions. A standard curve was used to calculate ARE enzyme activity, and ARE test was studied by making 1/1 dilution.
Statistical analysis
Statistical analyzes were performed with IBM SPSS Statistics, Version 23.0 (SPSS Inc., Chicago, IL, USA). Difference analysis in terms of continuous variables between the two groups was performed using the Student’s t-test, in which the mean values were compared for those with normal distribution, and the Mann–Whitney U test, in which the median values were compared for those who did not. In the analysis of dependent variables with more than two groups, the one-way analysis of variance (ANOVA) test was used for those with normal distribution and the Kruskal–Wallis test for those who did not. To examine the relationship between the groups, the Pearson and Spearman correlation analyzes were performed, and the correlation coefficients were reported. The limit of significance was accepted as p < 0.05.
Results
The mean age of the patients was 65.63 ± 8.85. In this study, which included 100 eyes of 100 patients, 52 volunteers were male (52%) while 48 volunteers were female (48%). The OSI score was 0.396 in men and 0.386 in women, which has not a significant difference (p = 0.741). Also, there was no significant difference between sex in terms of TAS, TOS, and ARE levels (p > 0.05) (Table 1).
TAS, TOS, OSI, and ARE values by sex.

ARE, arylesterase; OSI, oxidative stress index; SD, standard deviation; TAS, total antioxidant status; TOS, total oxidant status.
When the patients were grouped as immature (n = 72) and mature (n = 28) according to cataract maturity, TAS, TOS, OSI, and ARE levels were similar. As there was no grade 1 patient in this study, TOS, OSI, and ARE levels were similar among grade subgroups. TAS level was significantly higher in the grade 2 group compared with the grade 4 group (p = 0.023) (Table 2).
TAS, TOS, OSI, and ARE levels by grade subgroups.

ARE, arylesterase; OSI, oxidative stress index; SD, standard deviation; TAS, total antioxidant status; TOS, total oxidant status.
One-way ANOVA/Kruskal–Wallis test.
There was no correlation between grade and TOS, OSI, and ARE levels. There was a significant low negative correlation between cataract grade and TAS level (r = −0.237; p = 0.018).
The patients were classified as nuclear (n = 20), posterior subcapsular (n = 28), and mixed (n = 52) according to the clinical type of cataract. When evaluated according to morphological subtypes, there was no significant difference between the groups regarding TAS, TOS, OSI, and ARE levels.
Patients were also divided into two groups as non-DM (n = 45) and DM (n = 55). The mean age of the patients was 66.82 years in the non-DM group and 64.65 years in the DM group, and there was no statistically significant difference between the groups in terms of age (p = 0.225). Of those in the non-DM group, 28 (62.2%) were male and 17 (37.8%) were female, and 24 (43.6%) of the DM group were male and 31 (56.4%) were female. There was no statistically significant difference between the groups in terms of sex (p = 0.064). In addition, there was no difference between the non-DM and DM groups in terms of hypertension, presence of coronary artery disease, and aspirin use (Table 3).
Demographic, clinical, and biochemical characteristics of patients.

ASA, acetylsalicylic acid; CAD, coronary artery disease; DM, diabetes mellitus; HbA1c: hemoglobin A1c; HT, hypertension.
p < 0.05.
There was no significant difference between non-DM and DM patients in terms of TAS, TOS, OSI, and ARE levels. It was found a significant negative correlation between HbA1c level and TAS level (r = −0.205; p = 0.041). Similarly, a statistically significant negative correlation between age and TAS level was available (r = −0.203; p = 0.043). There was no correlation between HbA1c and age and TOS, OSI, and ARE (Table 4).
Correlation coefficients and p-values between patients’ HbA1c and age and variables.
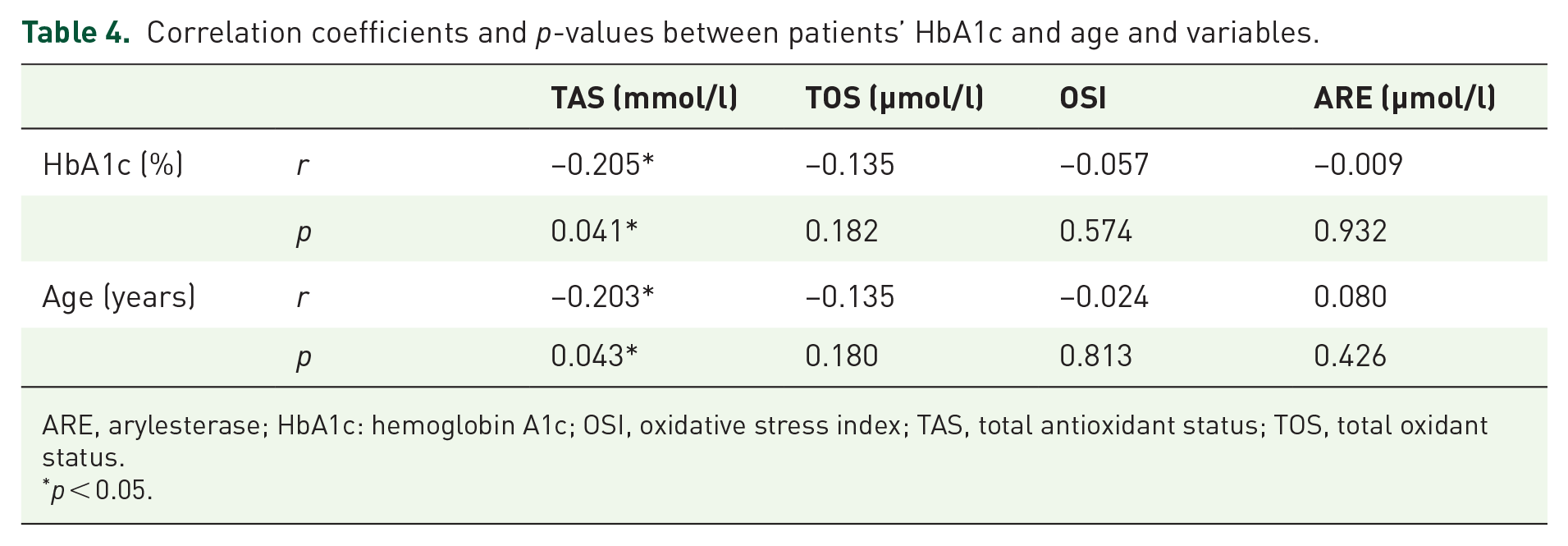
ARE, arylesterase; HbA1c: hemoglobin A1c; OSI, oxidative stress index; TAS, total antioxidant status; TOS, total oxidant status.
p < 0.05.
There was no statistically significant difference between the presence of hypertension and TAS, TOS, OSI, and ARE levels.
Discussion
In line with the increasing number and age of the world population, the health and economic burden of cataracts on people will increase, particularly in developing countries in which cataracts occur at an earlier age and cataract surgery is often inaccessible. Although cataract surgery is an effective treatment, investigating etiological factors and pathomechanism to delay or prevent cataract development is very important for the 21st Century. 15 Free radicals can contribute to cataract development by oxidizing lens proteins and forming disulfide bonds. Thus, the solubility of proteins can be reduced, and ion balance in the lens epithelium can be disrupted secondary to damage to the sodium–potassium ATPase (Na/K-ATPase) pump by free radicals. Membrane stability can be impaired due to the peroxidation of membrane lipids by these free radicals. 16
Miric et al. 17 showed that serum xanthine oxidase (XOD), a pro-oxidant enzyme that plays a role in diabetic lens damage and senile cataract formation, and malondialdehyde (MDA) levels increase. In contrast, lens SOD, GPx, and glutathione levels decrease with age. In a study by Maurya et al., 18 it was observed that the mean serum levels of SOD and catalase decreased as age increased. Similarly, in our research, we found that the level of aqueous humor TAS decreased with age. The decrease in antioxidant capacity with age may explain why cataracts are more common in the elderly population. On the contrary, Sawada et al. 19 did not detect any significant age-related difference in aqueous humor SOD and catalase levels.
In another study by Miric et al., 20 which aimed to evaluate the relationship between cataract maturity and lipid peroxidation markers and enzymatic antioxidants in aqueous humor, SOD decreased in mature cataracts, while catalase activity remained unchanged. On the contrary, Türk et al. 21 reported decreased TAS and increased TOS and OSI levels in the aqueous humor in patients with mature cataracts and suggested that oxidative stress may be associated with the maturation of senile cataracts. In this study, TOS, OSI, and ARE levels were similar in immature and mature cataract groups. Although the mean TAS value was low in mature cataracts, the difference did not reach statistical significance. Also, the TAS level was found to be significantly higher in the grade 2 group than the grade 4 group, and there was a significant negative correlation between the cataract grade and the TAS level. As the degree of cataract increases, the decrease in antioxidant capacity may reflect the rise in cataract development and oxidative events and the consumption of antioxidants to protect lens transparency. Zoric et al. 22 found a significant negative correlation between the degree of cataract and the induced percentage of MDA. It has been stated that with the progression of cataract, the glutathione level decreases, and significant changes appear in the activity of enzymes that regulate glutathione metabolism. 23
Cataract occurs primarily with advanced age but is also common in DM, in which superoxide in the mitochondria is elevated due to hyperglycemia. 24 In the study of Beyazyıldız et al., 25 it was determined that the level of aqueous humor TOS was significantly higher in diabetic patients than in patients with only cataracts. Aqueous humor TAS level was higher in diabetic patients with accompanying retinopathy but decreased in all diabetic patients. In the study published by Kırboğa et al., 26 no significant difference was found for serum TAS levels between diabetic retinopathy patients and healthy control groups, while TOS levels were found to be significantly higher in the diabetic retinopathy group. There was no significant difference in terms of TAS and TOS in the aqueous humor samples of the two groups. In the study conducted by Caner et al., 27 serum TAS values were found to be lower and TOS values higher in the diabetic retinopathy group compared with the diabetic group without retinopathy and the group without other systemic diseases except for the diagnosis of cataract. Also, no statistically significant difference was reported between the diabetic group and the control group in terms of aqueous humor TAS and TOS levels. In this study, there was no significant difference between the aqueous humor TAS, TOS, and OSI levels between diabetic and nondiabetic cataract patients.
In the study conducted by Hashim and Zarina 28 to investigate the relationship between aging and diabetes and oxidative stress with cataract, ARE level was found to be significantly lower in the senile cataract group than the control group. In the study conducted by Caner et al., 27 however, no significant difference was found between the groups in terms of aqueous humor ARE value. This result was consistent with the result of this study.
Chronic hyperglycemia is an essential factor in the development of secondary complications of diabetes, including diabetic cataract. Studies have shown that hyperglycemia and the duration of diabetes increase the risk of developing cataracts. 29 As the approximate erythrocyte lifespan is 120 days, HbA1c levels are a good indicator of circulating blood sugar level for the last 4 months. 30 In a study investigating whether there is a correlation between HbA1c values and oxidant and antioxidant parameters, a significant negative correlation was found between HbA1c values and plasma SOD, catalase, GPx, and glutathione levels, and also a significant positive correlation with MDA level. 31 In the study of Miric et al., 17 HbA1c concentration showed a positive correlation with lens and serum XOD activity. We also found a significant negative correlation between HbA1c level and TAS level. These results suggest that poor glycemic control may regulate ocular oxidative activities, possibly contributing to earlier cataract onset. In a supporting study, TAS levels in the aqueous humor of alloxan-induced hyperglycemic rabbits decreased by 66% compared with control animals, and TAS levels in rabbits treated with oral antidiabetic were increased above control values. 32
In conclusion, aqueous humor samples of patients with a high degree of cataract are characterized by low antioxidant capacity. This study shows that decreased antioxidant capacity in parallel with other studies has a role in the pathogenesis and progression of cataracts. In addition, as age and serum HbA1c level increase, the aqueous humor antioxidant level decreases. It can be suggested that serum HbA1c level in diabetic patients may be an indicator for the risk and progression of cataract development, and blood sugar regulation may prevent or delay cataract development. The limited number of the study population is the weakness of this study, however. More studies examining the relationship between cataract maturity and serum blood glucose level and oxidative stress are needed to confirm the results.