
Abstract
Background:
Optic disc oedema (ODE) is an important manifestation in various ocular as well as systemic disorders. Measurement of retinal nerve fibre layer (RNFL) thickness in ODE patients may help in monitoring the progress of the disease and treatment response.
Objective:
To assess the clinical characteristics, aetiology and retinal nerve fibre layer (RNFL) imaging features of optic disc oedema (ODE) patients.
Design:
A retrospective observational study.
Methods:
This hospital-based study included performed for patients presenting with unilateral or bilateral ODE at the ophthalmology outpatient department of a tertiary institute between January 2019 and December 2019. Clinical features of all ODE patients were noted. RNFL thickness was measured by spectral-domain optical coherence tomography (Cirrus 500, Carl Zeiss Meditec, Dublin, CA, USA).
Results:
Sixty-four patients with ODE were seen with female preponderance (56.2%). The mean age of presentation was 36.8 ± 13.8 years. Bilateral ODE was seen in 57.8% patients. The most common cause of bilateral ODE was idiopathic intracranial hypertension (IIH) and vascular papillopathy. Retinal vein occlusion (RVO)-associated ODE was the most common unilateral presentation. Presenting visual acuity was best with IIH and worst with anterior ischaemic optic neuropathy (AION). The mean duration of symptoms was maximum with intracranial space-occupying lesion associated papilloedema and minimum with AION. The mean RNFL thickness was highest in uveitis-associated ODE, followed by compressive ON, and IIH. A positive correlation was noted between clinical ODE severity and RNFL thickness. All aetiological categories (except uveitic and compressive) had maximum RNFL thickening in the inferior quadrant and minimum in the temporal quadrant.
Conclusion:
The current study provides a clinical profile and RNFL measurements of ODE patients at this locality. The clinical severity of ODE correlated positively with RNFL thickness and most of the categories of ODE followed the normative pattern of RNFL thickness (inferior > superior > nasal > temporal) despite thickening.
Keywords
Introduction
Optic disc oedema (ODE) can be a vital manifestation of varied ocular as well as systemic disorders. 1 Some of them are relatively benign, while others may have devastating visual and neurological consequences. ODE is a collective term including ‘papillitis’, that is, disc oedema due to inflammation of optic disc, ‘papilloedema’, that is, disc swelling due to elevated intracranial pressure, and ‘pseudopapilloedema’, that is, the normal physiological variant without any pathological feature. ODE can also result from ischemic optic neuropathy, which results from the infarction of the optic nerve head due to occlusion of the posterior ciliary arteries. 2
Ophthalmologists may be the person whom a patient with ODE consults first and foremost. Thus, ophthalmologists must know how to differentiate among the varied aetiologies based on the history and clinical features. Systemic investigations and radiological imaging should be tailored according to the patient’s provisional diagnosis based upon history and examination. It is the clinician’s role to place the swollen optic disc in the context of the patient’s demographic and clinical profile (age, sex, medical comorbidities and body habitus) and careful neuro-ophthalmic evaluation. 1 A prompt diagnosis and treatment may be sight and life-saving in many of these cases.
Clinical examination on fundoscopy still remains the most preferred investigation to diagnose ODE and differentiate it from cases of pseudopapilloedema. The morphological and vascular signs of disc oedema help an ophthalmologist to diagnose ODE with high accuracy and sensitivity. It includes a combination of four features, that is, swelling, haemorrhage, papilla elevation and peripapillary vessel congestion. The presence of retino-choroidal folds is most specific for true disc oedema. 3
Spectral-domain optical coherence tomography (SD-OCT) of the optic nerve head has recently proved its suitability in identifying and quantifying ODE in limited studies by measuring the retinal nerve fibre layer (RNFL) thickness.4 –6 This is an in vivo quantitative and objective measure that can detect, characterize and monitor axonal swelling associated with ODE. It is also an important tool to differentiate true ODE cases from pseudopapilloedema and also in cases with early ODE, where the clinical examination is inconclusive.5,6 However, there is no definitive evidence yet that OCT can define a particular pattern of ODE.
Recent studies also looked at the OCT angiographic (OCTA) features in patients with papilloedema, papillitis and non-arteritic ischemic neuropathy (NAION). In the acute phase, the clinical picture may not be diagnostic of specific aetiology and quantitative measurement on OCT can be inconclusive. On OCTA, there may be pattern alteration in the peripapillary capillary vessels in cases with NAION and papillitis, whereas surface capillaries can be dilated and tortuous in patients with papilloedema. 7
In the present study, we aimed to look at the demographic profile, presenting symptoms and fundus manifestations among the varied aetiologies of ODE. We also measured the RNFL thickness in various categories and assessed the correlation between the clinical severity of ODE and RNFL thickness.
Materials and methods
This was a hospital-based retrospective observational study performed at a tertiary care institute in North India. A retrospective chart review of all patients with unilateral or bilateral ODE presenting to the ophthalmology outpatient department of this institute from January 2019 to December 2019 was done. Approval from the institutional review board was obtained, and the study followed the tenets of the declarations of Helsinki. Patients with pseudopapilloedema and other ocular disorders likely to affect RNFL thickness (glaucoma, neurodegenerative disorders, previous retinal laser/surgery or any other history of optic nerve disease) were excluded from the study. Demographic data and pertinent clinical history, including chief presenting complaint, duration of symptoms, laterality of the disease and associated systemic complaints (transient ischemic attacks, diplopia, ocular pain, headache, vomiting and others), were recorded. The nature of patient referral (neurologist, general physician, paediatrician, outside ophthalmologist, self-referral or incidental) was also noted. Ocular evaluation details in the form of best-corrected visual acuity (decimal), colour vision (Ishihara chart), intraocular pressure (Goldman applanation tonometry), pupillary reaction, extraocular movements and slit-lamp evaluation of anterior segment were noted. Fundus details on slit-lamp biomicroscopy with 90D lens as well as by indirect ophthalmoscope after pupillary dilatation and posterior pole colour fundus photograph (ZEISS VISUCAM 524 fundus camera) were reviewed in all cases. Disc oedema was graded according to the modified Frisen scale initially and was further categorized into mild (Grade I Frisen), moderate (Grade II/III Frisen) and severe (Grade IV/V Frisen) for the purpose of analysis. 8 OCT optic disc cube 200*200 analysis was done wherever acquired, using Cirrus HD-OCT 500 (Carl Zeiss Meditec, Dublin, CA, USA). OCT scans of signal strength seven or above were only used for analysis. The average RNFL thickness and those of the four principal quadrants (i.e. inferior, superior, nasal and temporal) were analysed. Scans, where the segmentation line did not pass through the actual layers, were not considered. In the case of bilateral involvements, OCT RNFL value of the eye with higher RNFL thickness was considered for analysis. The mean RNFL thickness of both eyes was not taken as the grading of ODE was essentially not the same in each eye in bilateral cases. OCT macular scans had been performed in patients with clinically evident macular involvement on fundoscopy. Visual field analysis was performed by static automated perimetry in patients with mild to moderate visual impairment for possible field defects. Details of systemic evaluation and laboratory investigations were noted wherever applicable. Details of imaging characteristics like magnetic resonance imaging (MRI), contrast-enhanced MRI (CEMRI), computed tomography (CT) and contrast-enhanced computed tomography (CECT) reports were also noted in available cases. Few patients underwent lumbar puncture and complete cerebrospinal fluid (CSF) analysis based on a neurologist’s opinion. The final diagnosis of the aetiology of ODE was made by two experienced ophthalmologists in conjunction with the opinion of neurologist, physician and paediatrician as deemed necessary.
Categorical variables were presented as absolute numbers and their percentages. Quantitative variables were summarized by mean, standard deviation, median and other descriptive statistics. Correlation between RNFL and clinical severity of ODE was performed by Kruskal–Wallis test.
Results
After excluding 10 patients of pseudopapilloedema (optic nerve head drusens: 4; hypermetropia: 3; and myelinated nerve fibre; 3), 64 cases with ODE were eligible for analysis. There were 28 (43.75%) males and 36 (56.25%) females. Among all the patients, 37 (57.81%) had bilateral ODE and 27 (42.19%) had unilateral ODE at presentation. ODE patients were categorized according to the following aetiologies: Vascular papillopathy (11), uveitis (11), retinal vascular occlusion (RVO; 10), idiopathic intracranial hypertension (IIH; 10), papilloedema secondary to intracranial space-occupying lesion (ICSOL) & cerebral venous thrombosis (8), anterior ischaemic optic neuropathy (AION; 5), optic neuritis (ON; 4), toxic ON (3) and compressive optic neuropathy (2). Among the vascular papillopathy group, five were due to diabetic papillopathy and six were associated with hypertensive ODE. Among the 11 patients of uveitic ODE, the distribution was neuroretinitis (3), posterior scleritis (2), Vogt-Koyanagi-Harada disease (1), sympathetic ophthalmitis (1), possible tubercular panuveitis (2), acute retinal necrosis (1) and multifocal choroiditis (1). Among the 10 RVO patients, all had central retinal vein occlusion (CRVO) except one with hemi-CRVO. In the compressive optic neuropathy group, one patient had bilateral ODE due to thyroid-associated ophthalmopathy, and the other had unilateral ODE due to nonspecific orbital inflammation.
We also analysed the common aetiologies of ODE according to age less than 40 years and more than 40 years. In the younger population (<40 years), the common aetiologies were IIH, hypertensive papillopathy, toxic ON, compressive ON and papilloedema secondary to cortical venous thrombosis and cerebellopontine angle tumour. In the older age group (>40 years), the common aetiologies were AION, ON, RVO, diabetic papillopathy and papilloedema secondary to suprasellar mass lesions.
The demographic profile of various aetiologies of ODE is summarized in Table 1. ODE due to vascular papillopathy, uveitis and RVO had male preponderance, while the rest of the aetiologies were more commonly seen in females. The mean age of presentation was least in ODE due to toxic ON followed by IIH, and highest in ODE due to AION followed by RVO. Other than patients with papilloedema, all of the vascular papillopathy and IIH patients had bilateral involvement. As compared to that, all RVO patients had unilateral involvement. ODE due to other aetiologies had either unilateral or bilateral involvement. The presenting visual acuity was best in cases with IIH and worst in cases with ON. Cases with ODE due to uveitis, RVO, AION, ON, toxic ON and compressive ON were diagnosed foremost in ophthalmology OPD. On the other hand, cases with papilloedema, vascular papillopathy and IIH initially presented to neurologist, paediatrician or physician and were subsequently referred to ophthalmology OPD.
Comparative demographic features among varied aetiologies of optic disc oedema (ODE).
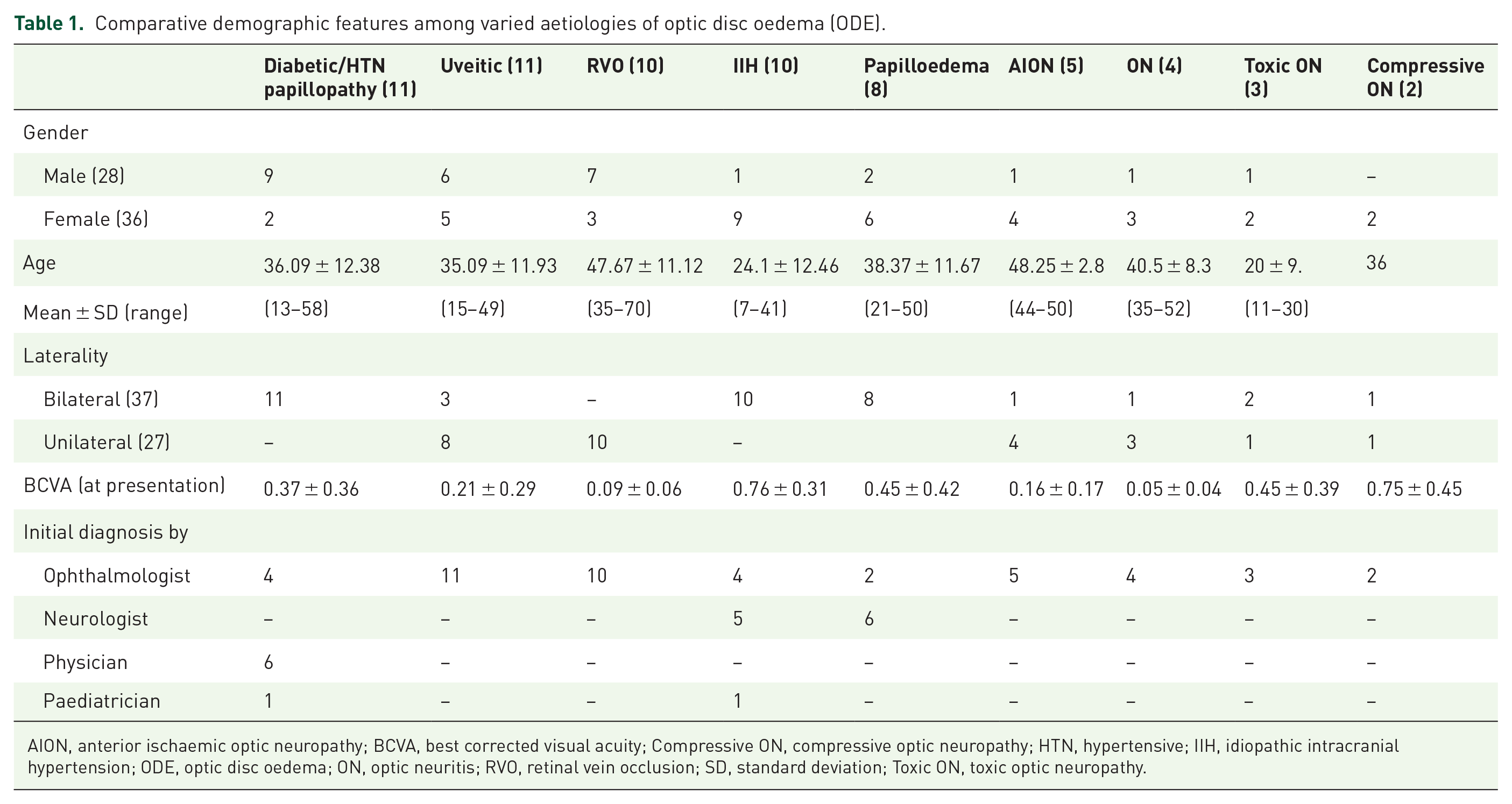
AION, anterior ischaemic optic neuropathy; BCVA, best corrected visual acuity; Compressive ON, compressive optic neuropathy; HTN, hypertensive; IIH, idiopathic intracranial hypertension; ODE, optic disc oedema; ON, optic neuritis; RVO, retinal vein occlusion; SD, standard deviation; Toxic ON, toxic optic neuropathy.
The duration of symptoms at the time of presentation was maximum in cases with papilloedema due to ICSOL and minimum with AION. According to symptomatology, a gradual diminution of vision was the primary presenting symptom in ODE due to vascular papillopathy and papilloedema; conversely, ODE due to AION, ON, RVO and uveitis presented with a sudden decrease in vision. Headache was the chief presenting feature in IIH, whereas ocular pain was most commonly noted in ON patients. Most of the patients with vascular papillopathy, uveitis and AION presented with moderate ODE, whereas most papilloedema and IIH patients had severe ODE. ON and toxic neuropathy presented as mild ODE predominantly. The duration of symptoms, chief presenting complaints, ODE severity and additional fundus features of various aetiologies are summarized in Table 2.
Symptomatology and clinical characteristics in different categories of ODE.
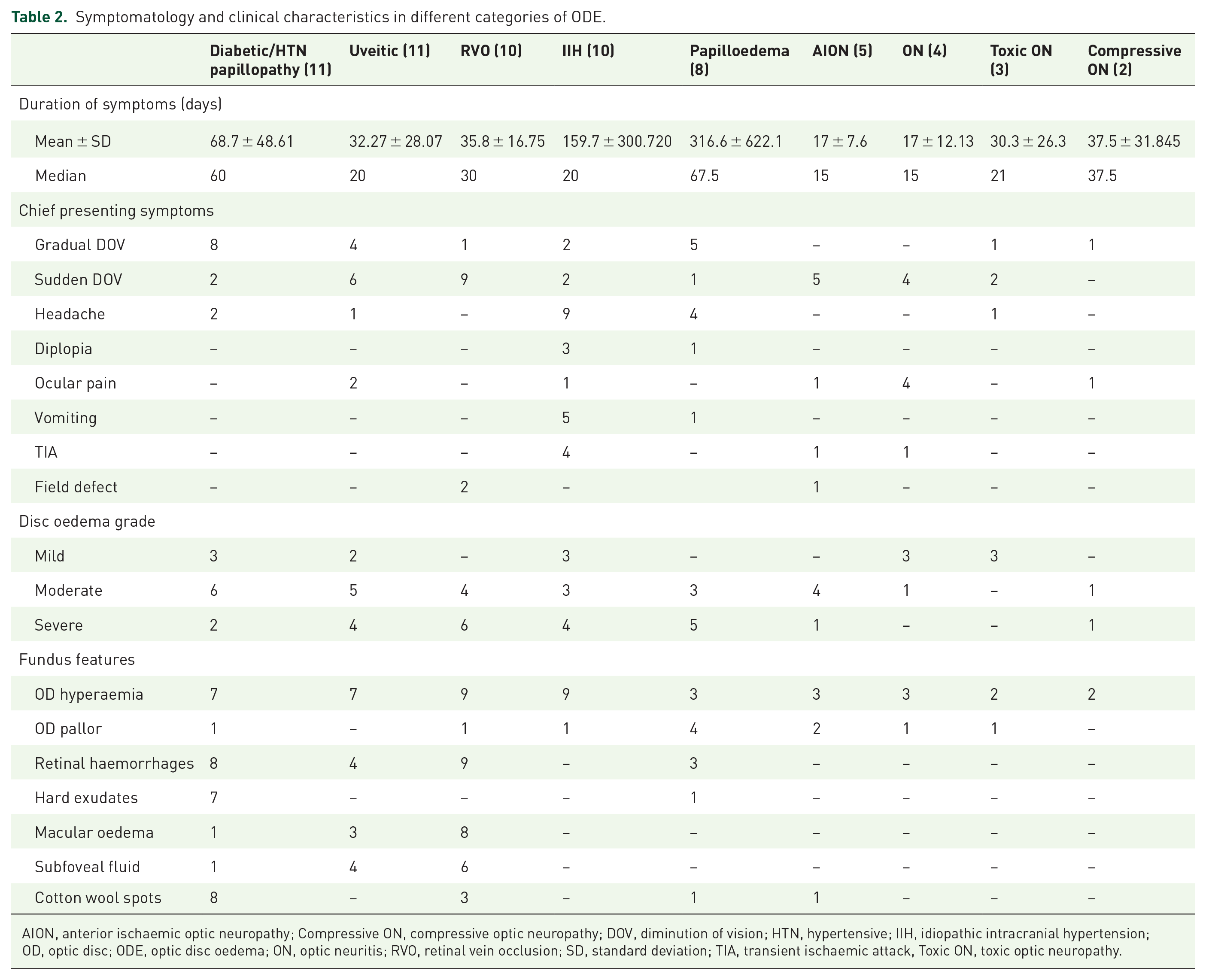
AION, anterior ischaemic optic neuropathy; Compressive ON, compressive optic neuropathy; DOV, diminution of vision; HTN, hypertensive; IIH, idiopathic intracranial hypertension; OD, optic disc; ODE, optic disc oedema; ON, optic neuritis; RVO, retinal vein occlusion; SD, standard deviation; TIA, transient ischaemic attack, Toxic ON, toxic optic neuropathy.
The average retinal nerve fibre layer (RNFL) thickness in various categories of ODE is shown in Table 3 and is also represented in box-plot analysis in Figure 1. As the OCT RNFL was not performed in most RVO patients, this category was excluded for RNFL analysis. In patients with ON and toxic ON, the mean RNFL thickness was less than 150 microns. Conversely, cases with uveitis, IIH, papilloedema, AION and compressive optic neuropathy had a mean RNFL thickness of more than 200 microns. Patients with vascular papillopathy had mean RNFL thickness in between the above ranges. All of the categories had maximum RNFL thickness in the inferior quadrant (except ODE due to uveitic and compressive aetiologies) and minimum RNFL thickness in the temporal quadrant (Table 3). All of the categories except ODE due to uveitic and compressive aetiologies had the same pattern of RNFL thickening (inferior > superior > nasal > temporal, i.e. I > S > N > T). Only uveitic and compressive aetiologies had the slight reversal of the pattern of RNFL thickening involving the vertical quadrants, where the superior quadrant was thicker as compared with the inferior quadrant(S > I > N > T).
Retinal nerve fibre layer (RNFL) thickness in all quadrants in varied aetiologies of ODE.

AION, anterior ischaemic optic neuropathy; HTN, hypertensive; IIH, idiopathic intracranial hypertension; ODE, optic disc oedema; ON, optic neuritis; RNFL, retinal nerve fibre layer; SD, standard deviation.

Box plot analysis of RNFL thickness in different aetiologies. The vertical axis denotes the RNFL thickness (microns) and the horizontal axis denotes the various aetiological causes of disc oedema. In cases with optic neuritis (ON), toxic optic neuropathy (Toxic) and vascular papillopathy (vascular), the median RNFL thickness was less than 200 microns and upper range did not cross 300 microns. Whereas with papilloedema and uveitic causes, the median RNFL thickness was more than 200 microns and had a wider range.
We also correlated the clinical severity of ODE with the RNFL thickness in all four quadrants (Table 4). The average RNFL thickness in mild, moderate and severe disc oedema was 143.2 ± 38.6 microns, 168.8 ± 61.8 microns and 273.8 ± 86.8 microns, respectively. Clinical severity of ODE had a significant positive correlation with RNFL thickness and all grades of clinical severity (mild, moderate and severe) followed the same pattern of RNFL quadrantic thickening (I > S > N > T).
Correlation of disc oedema severity with average and quadrantic RNFL thickness.

DOF, degrees of freedom; ODE, optic disc oedema; RNFL, retinal nerve fibre layer.
H statistics for Kruskal–Wallis test (DOF: degrees of freedom) and p value, significant is taken below 0.05.
Contrast enhanced MRI (CEMRI) was done in all cases with papilloedema (8) and the primary aetiologies diagnosed were four cases of suprasellar mass lesion and one case of each cerebellopontine schwannoma, occipital condylar chondrosarcoma, fourth ventricle choroid plexus papilloma and cerebral venous thrombosis. MRI with magnetic resonance venography (MRV) was performed in cases of IIH. The common neuroimaging findings noted in IIH were vertical tortuosity of the optic nerve, distended parenchymal sheath and flattening of the posterior aspect of the globe in some cases. All of the IIH patients also had increased CSF opening pressure.
Discussion
In the current study, we have presented the clinic-demographic features of cases with unilateral or bilateral ODE, who presented to the ophthalmology outpatient department themselves or were referred from the fellow subspecialties to rule out ophthalmic manifestations of systemic aetiology. According to previously reported studies, the common causes of unilateral ODE are demyelinating ON, non-arteritic AION, RVO and localized compressive aetiology, whereas papilloedema, toxic ON, infiltrative ON and malignant HTN are reported as common causes of bilateral ON.1,9,10 In accordance with the above reports, the most common causes of unilateral ODE in our study were RVO, uveitis, AION and ON. The most common causes of bilateral ODE were hypertensive and diabetic papillopathy, IIH and papilloedema in our series. Diabetic papillopathy has an incidence of around 0.5% and is a diagnosis of exclusion after ruling out inflammation, infection, or other afflictions of the optic nerve and raised intracranial pressure.1,11 Although it may be unilateral or bilateral and may be associated with either non-proliferative or proliferative diabetic retinopathy, all of our patients of diabetic papillopathy were bilateral and associated with non-proliferative disease except one. In another case series, the incidence of bilateral diabetic papillopathy was reported to be 50%. 11 The reason for the high bilaterality of diabetic papillopathy in our series could be merely incidental in a small number of patients.
A study on the Japanese population aimed to identify the causes and prognosis of optic disc swelling in 93 cases with ODE. In that study, AION and ON were the leading causes of unilateral ODE. AION was the leading cause in the more than 50 years age group (15/29) and ON in the less than 50 years (13/31). Complaints of ocular pain or headache were more common in ON than AION cases (70% versus 19%). In bilateral cases, papilloedema was the common cause in both age groups and accounted for 48.5% of all cases. The aetiological association of papilloedema was intracranial mass lesion (7 out of 16 cases), IIH (4 cases) and cerebral venous sinus thrombosis (2 cases). 9
In our study, the leading cause of bilateral ODE in the <40 years age group was IIH, followed by hypertensive papillopathy, and in the >40 years age group, intracranial mass lesion was the leading cause. Among unilateral ODE, RVO and AION were the leading causes in the >40 years age group, and uveitic ODE was the common cause in the <40 years age group. Although the mean age of ON was just above 40 years in our study, this could be due to more elderly and atypical ON patients being referred to us. ON in the younger age group is mostly self-limiting; the majority might not reach us to seek a referral. Similarly, the mean age group of AION is relatively lesser (despite above 40 years) in our study, probably because elderly populations have more chance of being neglected and may have difficulty accessing healthcare facilities. Moreover, the major area that our institute caters to includes a sub-Himalayan difficult geographical terrain. Thus accessing our healthcare facility may be particularly difficult for the elderly explaining the overall decreased mean age of the study population. However, being a tertiary care multispecialty institute, we had a broader aetiological perspective of ODE cases. Such patterns and distribution are expected to vary from different institutes of different geographical locations, especially depending upon the nature of the institute (only ophthalmic institute/ multispecialty institute). This is also the reason why cases with papilloedema, diabetic and hypertensive retinopathy in our study presented to the neurologists and physicians first and were subsequently referred to us for confirmation. Being a teaching tertiary care institute, all patients were thoroughly evaluated through interdepartmental consultation. Early cross-referral also helps in monitoring and managing associated treatable ocular lesions, as all of the diabetic papillopathy patients in our series had concomitant diabetic retinopathy requiring treatment with anti-vascular endothelial growth factor injections or laser photocoagulation.
In a study on the Indian population conducted in a multispecialty tertiary hospital to look for the profile of cases visiting their neuro-ophthalmology clinic, 335 (33%) out of 1020 cases with optic neuropathy had associated ODE. The causes of optic neuropathy with ODE were ischemic ON (37.6%), postpapilloedema (23.2%), papillitis/ neuroretinitis (28.9%), inflammatory optic neuropathy (2.9%) and consecutive optic neuropathy (7.2%). Patients with papillitis had a younger mean age at presentation (32.5 ± 11.8 years) versus ischaemic optic neuropathy (56.7 ± 13.6 years). Common causes of papilloedema/post papilloedema optic neuropathy included idiopathic intracranial hypertension, intracranial tumour, hydrocephalus and cerebral venous sinus thrombosis. 10 In our study, the commonest causes of ODE was papilloedema (28.2% including cases with IIH and ICSOL), followed by uveitis and HTN/DM papillopathy (17.2% each), RVO (15.6%), AION (7.8%) and ON (6.2%) sequentially. The previous study looked into the cases of disc oedema that were referred to the neuro-ophthalmology clinic only. So, cases with uveitis and vascular disorders were not included. Although we looked at fewer cases with ODE, we got a broader perspective of all cases and their presenting features.
The reliability and reproducibility of OCT RNFL thickness measurements have been tested in studies on healthy subjects and patients with glaucoma. 12 Progressive thinning of RNFL is reported in diseases like glaucoma, Alzheimer’s disease and Parkinson’s disease in various studies.13,14 On the other hand, ODE is associated with an increase in RNFL thickness.6,15 In addition to thickening, there is presence of a hyporeflective area beneath the sensory layers and a triangular space at the ONH. 16 In cases with optic nerve drusens, this space has ovoid hyperreflective deposits. Menke et al. 15 also measured the percentage of RNFL (RNFL%) compared with peripapillary total retinal thickness and then evaluated normalized RNFL thickness (nRNFL%) by using the data of corresponding age-matched healthy control subjects. The authors found a significant difference within the averaged nRNFL% values in the ON group (suggesting oedema primarily affecting RNFL) but no such difference in RVO group (suggesting oedema affecting all retinal layers). 15
The present study illustrates the importance of OCT in ODE assessment and found a positive association between the fundoscopic grade of ODE and RNFL thickness. The higher the grading of disc oedema clinically, the more was the RNFL thickness on OCT.
Carta et al. 6 demonstrated the utility of SD-OCT in differentiating patients with papilloedema from pseudo-ODE (PODE). They concluded that the average and any single-quadrant RNFL thickness was significantly higher in the ODE group than the PODE and control groups. The average and the inferior quadrant thicknesses tested the most potent parameters to differentiate ODE from PODE. A cutoff value of 110 μm for the average area or 150 μm for the inferior quadrant was associated with maximal sensitivity and specificity with a positive predictive value greater than 80%. 6 Although we have not included cases with PODE in the current study and OCT-based morphological differentiation between true ODE and PODE is beyond the scope of the current study, it is of paramount importance to differentiate between these two entities to avoid unnecessary neuroimaging in a resource constraint setting.
The probable reason why the inferior quadrant of the optic nerve head is affected more severely is explained by the assumption that the swelling of a true ODE is primarily due to blockage of axoplasmic transport and subsequent intracellular accumulation of organelles. The swelling will be more pronounced in large-calibre axons originating from large retinal ganglion cells typically located at the inferior (due to overcrowding) and nasal quadrant (due to larger size) of the optic nerve head. 17 This is in accordance with the OCT RNFL thickness noted in our study, where all of the aetiological categories (except uveitic and compressive aetiologies) had inferior RNFL thickness more than superior, and nasal RNFL thickness more than the temporal. In uveitic patients, the RNFL gets secondarily involved to other juxtaposed choroidal or retinal lesions. Hence, depending upon the primary area of inflammatory involvement in uveitis, the highest RNFL swelling may be evident in any quadrant. The same explanation holds true for the compressive aetiology as well. Apart from these two categories, the double hump pattern of RNFL thickness (inferior more than superior, nasal more than temporal) was maintained in all other aetiological categories as well as across all severity levels (mild, moderate and severe) of ODE similar to previously reported normative database of RNFL thickness in Indian eyes. 18
Although it is difficult to recommend a specific pattern or cutoff value of RNFL thickness consistent with a particular aetiology based on this limited data, certain clues may still help us in the diagnosis. ODE due to ON and toxic aetiologies generally cause mild oedema with normal macula, whereas disc oedema associated with uveitis, RVO, and vascular papillopathy can have disc oedema of variable severity and may also have associated macular changes (hard exudates, subretinal fluid, cystoid spaces). Although not assessed in the present study, retinal pigment epithelium (RPE) bending anteriorly has been reported in patients with IIH. 19
Our study has a few limitations too. One of them is the small sample size and its retrospective nature. We have also not analysed the RNFL thickness measurements according to separate age groups. Although most of our study population belonged to the age group between 18–50 years, few were beyond this age range. This could have a bearing on the mean RNFL thickness in various categories as they were not age-matched due to the low sample size. RNFL measurements of RVO patients were not available as it was a retrospective review. Patients with retrobulbar ON, optic disc pallor and atrophy were excluded from our study. This might have changed the exact prevalence of various aetiological causes. Finally, being a tertiary institute, we might have referral bias, and our sample might not have reflected true representatives of the general population.
Despite the above limitations, the present study gives an overview of ODE patients in this particular geographical area and provides baseline RNFL measurements in various aetiological categories. RNFL thickness showed a significant positive correlation with all severity of ODE and maintained an identical pattern in most of the categories similar to normative RNFL measurements (I > S > N > T). The RNFL values in mild, moderate and severe ODE may also serve as a reference yardstick for quantitative categorisation of ODE, and future prospective studies with a larger sample size may be designed to validate our initial observations.
Footnotes
Author contributions
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Research ethics and patient consent
The study adhered to the tenets of the Declaration of Helsinki for studies involving human subjects. The study was approved (AIIMS/IEC/20/634) by the institutional Ethics Committee of the All India Institute of Medical Sciences, Rishikesh, India. The need for patient consent was waived as this was a retrospective observational study.