
Abstract
Background
The exact pathophysiology of cluster headache (CH) is still not fully clarified. Various studies confirmed changes in ocular blood flow during CH attacks. Furthermore, vasoconstricting medication influences blood supply to the eye. We investigated the retina of CH patients for structural retinal alterations with optical coherence tomography (OCT), and how these changes correlate to headache characteristics, oxygen use and impaired visual function.
Methods
Spectral domain OCT of 107 CH patients – 67 episodic, 35 chronic, five former chronic sufferers – were compared to OCT from 65 healthy individuals. Visual function tests with Sloan charts and a substantial ophthalmologic examination were engaged.
Results
Reduction of temporal and temporal-inferior retinal nerve fibre layer (RNFL) thickness was found in both eyes for CH patients with a predominant thinning on the headache side in the temporal-inferior area. Chronic CH patients revealed thinning of the macula compared to episodic suffers and healthy individuals. Bilateral thinning of temporal RNFL was also found in users of 100% oxygen compared to non-users and healthy controls. Visual function did not differ between patients and controls.
Discussion
Our OCT findings show a systemic effect causing temporal retinal thinning in both eyes of CH patients possibly due to attack-inherent or medication-induced frequent bilateral vessel diameter changes. The temporal retina with its thinly myelinated parvo-cellular axons and its more susceptible vessels for the vasoconstricting influence of oxygen inhalation seems to be predisposed for tissue damage-causing processes related to CH.
Keywords
Introduction
Cluster headache (CH) is the most frequent trigemino-autonomic headache with severe unilateral pain and with a high impact on quality of life. Rhythm of bouts, hypothalamus-associated behavioural symptoms such as aggressiveness and restlessness (1) and hormone level changes (2) led to the suspicion that the hypothalamus has a triggering role. This hypothesis could be underlined by positron-emission tomography (PET) (3) and voxel-based morphometry findings (4) in the ipsilateral inferior posterior hypothalamic grey matter and by the effectiveness of locally implanted deep brain stimulators (5). Additionally, the retino-hypothalamic-pineal axis might be involved (6).
This pathophysiological explanation has superseded the vascular theory (1) based on an increased venous load in the inflamed cavernous sinus (7). Nevertheless, vascular changes detected in CH could be a secondary effect of hypothalamic dysregulation.
Several studies indicate disturbed ocular conditions during attacks: Elevated intraocular pressure and corneal indentation pulse amplitudes (particularly ipsilateral to the pain) were attributed to an intraocular vasodilatation leading to an increase of volume of the intraocular vascular bed (8). Pathological orbital phlebograms were recorded, mostly showing partial or complete narrowing of the superior ophthalmic vein ipsilateral to the pain or even bilateral (9). Magnetic resonance (MR) angiography revealed dilated ophthalmic arteries ipsilateral to the pain (10). Arterial dilatation of the internal carotid artery (ICA) and its branches from the cavernous level were explained by inhibition of sympathetic vasocontractile fibres (7) or an unspecific pain-induced ‘trigeminal-autonomic neurogenic vasodilator mechanism’ (11).
In most cases, efficient medications for acute attacks as well as prophylactic treatment are attended by manipulation of vessel diameter – again affecting blood supply to the eye:
Triptans have vasoconstricting effects via the serotonin 1B receptors (12). Furthermore, inhalation of 100% oxygen at atmospheric pressure causes vasoconstriction, which in turn reduces retinal blood flow by 30% (13) to 60% (14) depending on the acquisition method – a finding which was recently confirmed by dual-beam bidirectional Doppler Fourier-domain optical coherence tomography (FD-OCT) examination (15). Otherwise, increased oxygen saturation after oxygen inhalation (16) might have a preventive effect in the retina of oxygen users.
Although the attack-inherent and the medication-induced vascular changes are only transient phenomena, the frequent occurrence of the disease, a temporary or permanent high frequency of attacks as well as the treatment of the disease itself might cause microvascular and structural abnormalities in the retina, since the retina tissue, among other human tissues, has the highest metabolic activity and thus the highest sensitivity to reduced oxygen supply (17). Frequent intake of prophylactic medication might have protective effects on retinal integrity.
As a tool for measuring retinal thickness, spectral domain OCT was applied, an innovative, fast applicable and non-invasive examination tool producing high-quality three-dimensional retinal images with an optical axial resolution of 7 µm and digital resolution of 3.9 µm, respectively, by interferometry at near-infrared wavelength. OCT has been established for an evaluation of axonal cell loss in the retina of multiple sclerosis patients (18,19) and in the meantime has come to be widely used as a tool inter alia for assessing the retinal degeneration process associated with a broad spectrum of neurodegenerative diseases (20). Modern spectral-domain technique, in particular, reaches a high degree of reproducibility and validity in retinal thickness measurements (21,22) with high interpersonal agreement (23).
Our aim was to investigate structural abnormalities in the retina of CH patients in comparison to healthy age-matched controls and how they correlate to visual function (visual acuity, low-contrast letter acuity, colour vision and visual field), headache characteristics (headache duration, attack rate, actually being in or out of bout and time interval since last bout) and medication use (oxygen, sumatriptan and verapamil).
Methods
Patients and controls
We performed OCT examination of 110 CH patients diagnosed according to the International Classification of Headache Disorders, second edition (ICHD-II) (24), of whom 107 (mean age 48.2 ± 9.9 years, 85% males) were included after ophthalmologic examination and review of OCT images. Sixty-seven suffered from episodic CH, 35 were primary or secondary chronic CH patients, and five were former chronic sufferers who underwent a change to the episodic type. Patients were recruited from the outpatient headache clinic of the University Hospital of Münster. The control group consisted of 65 healthy participants (mean age 46.17 ± 11.04 years, 74% males), 44 recruited from the Department of Neurology in Münster, and 21 from the NeuroCure Clinical Research Center at the Charité Berlin. To rule out other causes of retinal changes, exclusion criteria were spherical equivalent refractive error of more than ± 6 dioptres, ocular and non-ocular diseases like glaucoma, retinal degeneration, diabetic retinopathy, multiple sclerosis, cancer and neurodegenerative diseases.
Both eyes of the CH patients were factored into the analysis, differentiated ipsilateral and contralateral to the pain side with due consideration of the correlation between both eyes whereas only one eye of every healthy control was randomly selected.
The study was approved by the local ethics committee of the Charité – Universitätsmedizin Berlin and was conducted in accordance with the Declaration of Helsinki in its currently applicable version. All participants gave informed written consent.
Visual function testing
Binocular colour vision was studied using Ishihara tables, and Snellen visual acuity was assessed bi- and monocularly at 2 m, at first uncorrected, and then, with glasses, if appropriate. Low-contrast letter acuity was tested bi- and monocularly at 2 m for 2.5% and 1.25% contrast levels if corrected visual acuity amounted to at least 20/20. All healthy controls of the cohort from Münster and 53% of CH patients underwent an additional ophthalmological examination in the ophthalmologic department including standard automated perimetry using a 30-2 central threshold test (Humphrey 740i, Zeiss Meditec, Jena, Germany), refraction by autorefractor, best-corrected visual acuity and fundoscopy. Results of visual function tests, ophthalmologic examination and the OCT images were additionally judged by two versed ophthalmologists (FA, CC). Controls from Berlin had no relevant ophthalmologic diseases and their OCT images were substantially reviewed. They were not subjected to examination with Sloan charts.
OCT imaging
Analyses were performed using a spectral-domain OCT (Heidelberg Spectralis SD-OCT, Heidelberg Engineering, Germany, Spectralis acquisition module 5.4.7.0 and viewing module 5.5.0.5, HEYEX 1.7.0.0) based on an FD detector producing high-resolution three-dimensional retinal images. The same OCT device model was used in Münster and Berlin.
For both eyes of each patient, two analyses each were performed:
Retinal nerve fibre layer (RNFL) thickness (1 circular B-scan, 12 degrees (approximately 3.45 mm), 1536 A-scans, high-resolution mode). Mean number of averaging frames (automatic real-time (ART)) was 91.07, mean quality amounted to 32.05 (ranges from 0 (poor quality) to 40 (excellent quality)). Posterior pole (P.Pole) volume scans of the macula (768 A-scans, high-speed mode, ART: nine frames, scanning angle 30 degrees × 25 degrees, 120 µm distance between sections, 61 sections, scanning rate: 8.8/seconds, scan direction: 7 degrees).
Sectorial analysis of mean RNFL thickness is illustrated in Figure 1(a) and (b). Figure 2 shows examination of macular region of a patient affected by CH.
(a) RNFL measurement of the right eye of a male 48-year-old cluster headache (CH) patient with 30 years of disease duration, primarily right-sided episodic CH, since four years left-sided. Mean RNFL thickness (G) as well as six separate areas (temporal (T), temporal-inferior (TI), temporal-superior (TS), nasal (N), nasal-inferior (NI), nasal-superior (NS)) and the thickness of the papillo-macular bundle (PMB) are given. (b) RNFL measurement of the left eye of the patient described in Figure 1(a). RNFL: retinal nerve fibre layer. Examination of the macular region of the patient described in Figure 1(a). After the macular thickness map was obtained, the ETDRS grid 1,3,6 was applied to the map. Only the value of total macular volume without the calculated thickness parameters of the nine single EDTRS areas was included into our analyses. ETDRS: Early Treatment Diabetic Retinopathy Study.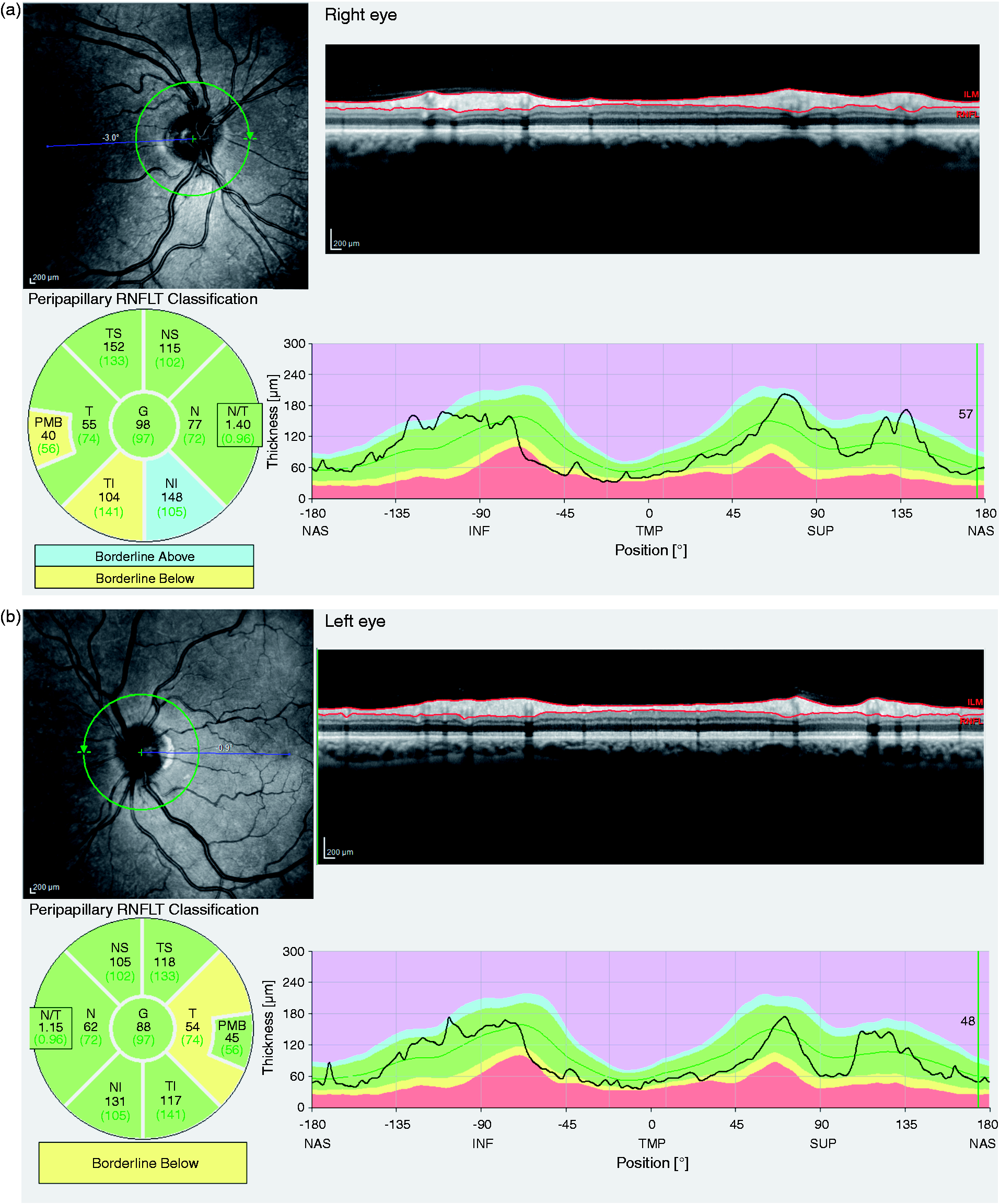

Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics Software Release 20.0 (2011, SPSS Inc, Chicago, IL, USA). Categorical variables were expressed as frequency and percentage, whereas continuous variables were presented as mean ± SD.
Student’s t-test was used to compare OCT parameters of the healthy controls examined in Berlin and Münster. It also helped to compare the mean age of the CH patients vs. healthy controls, while Chi-square-test was used for the comparison of gender proportion in these groups.
A univariate analysis of variance (ANOVA) was performed to evaluate the differences between retinal thickness parameters in the patients’ headache side, the non-affected side and the retinal thickness of healthy controls. After checking normality of the data using the Kolmogorov-Smirnov test and homogeneity of variance using Levene’s test, post hoc comparisons were applied to determine differences between groups in case of variance homogeneity using Bonferroni’s test, otherwise with the Games-Howell’s procedure. Paired t-test was used to compare two dependent groups (headache side vs. headache-free side).
The same procedures were employed for comparison of visual function results in these subgroups and for the three-group-comparison of retinal thickness parameters and visual function results of the eye on the headache side of chronic CH patients as well as episodic sufferers and healthy controls.
Student’s t-test was carried out to examine differences in OCT parameters, age and attack frequency of different subgroups of patients: users and non-users of different medication types, patients with ≤10 years and >10 years of manifest disease, patients actually being in and out of bout as well as patients with time intervals of <2 years and ≥2 years since last bout.
Within the subgroups of oxygen users and non-users, Chi-square-test and Fisher’s-exact test helped to evaluate differences in headache characteristics (percentages within the subgroups being in and out of bout, having chronic or episodic type of CH). The Pearson correlation coefficient was used to evaluate the relationship between two continuous variables: retinal thickness parameters with headache characteristics, the total amount of inhaled oxygen and visual function results. To measure the relationship between the total amount of oxygen use and retinal thickness parameters, simple linear regression analyses were conducted.
All tests except the primary endpoint (temporal RNFL) should be understood as constituting exploratory data analysis in such a way that no previous power calculation and adjustments for multiple testing were made. Differences were considered significant at p < 0.05.
Results
Three of 110 patients were excluded for glaucoma, retinal degeneration or monocular congenital blindness with abnormalities on the contralateral retina. In four patients, only one eye could be investigated because of traumatic lesion, retinal detachment, epiretinal gliosis and reduced quality of OCT images in the fellow eye. In the group of healthy controls, three of 68 examined people were excluded because of glaucomatous optic disc damage and epiretinal gliosis.
We statistically ensured that no effect of the study centre existed between the OCT parameters of the controls examined in Berlin and Münster. Patients and controls did not differ significantly in age and gender proportion.
Population and headache characteristics.

CH: cluster headache. Five patients with episodic, former chronic CH are not included in the group of episodic nor in the group of chronic sufferers.
Retinal thickness measurements
Comparison between both eyes of headache patients and controls for RNFL thickness parameters.

Significant (p < 0.05). We did not factor patients with former side shift of headache (n = 19) into this analysis. Figure 1 illustrates the six separately measured areas around the optic nerve head (temporal (T), temporal-inferior (TI), temporal-superior (TS), nasal (N), nasal-inferior (NI), nasal-superior (NS)) for which mean retinal thickness is given. Inferior (I) and superior (S) area were additionally calculated (I=½×(NI+TI); S=½× (NS+TS)). RNFL: retinal nerve fibre layer; PMB: papillo-macular bundle; ANOVA: analysis of variance.
Comparison between headache side of episodic CH patients, chronic CH patients and controls for RNFL thickness parameters and macular volume.

Significant (p < 0.05). bDifferent unit: not µm but mm3. Patients with history of side shift of headache were factored with recently affected side of head. Figure 1 illustrates the six separately measured areas around the optic nerve head (temporal (T), temporal-inferior (TI), temporal-superior (TS), nasal (N), nasal-inferior (NI), nasal-superior (NS)) for which mean retinal thickness is given. Inferior (I) and superior (S) area were additionally calculated (I = ½ ×(NI+TI); S = ½ ×(NS+TS)). Eleven of 21 healthy controls of the cohort of Berlin were not subjected to examination of macular region. Data of 54 healthy controls was used to compare macular volume parameters. CH: cluster headache; CHP: cluster headache patient; PMB: papillo-macular bundle; RNFL: retinal nerve fibre layer; ANOVA: analysis of variance.
Influence of headache characteristics
None of the examined headache features (headache duration ≤ or >10 years, attack rate per year in episodic sufferers, actually being in or out of bout and time interval since last bout < or ≥2 years) showed a correlation to OCT results.
Influence of oxygen inhalation and medication
We analysed the influence of oxygen inhalation on retinal integrity in the subgroup of episodic sufferers because the entire cohort of oxygen users contained all chronic sufferers and showed a significant age difference compared with non-users.
Comparison of selected RNFL thickness parameters between oxygen users and non-users among episodic sufferers and between oxygen users and healthy controls.
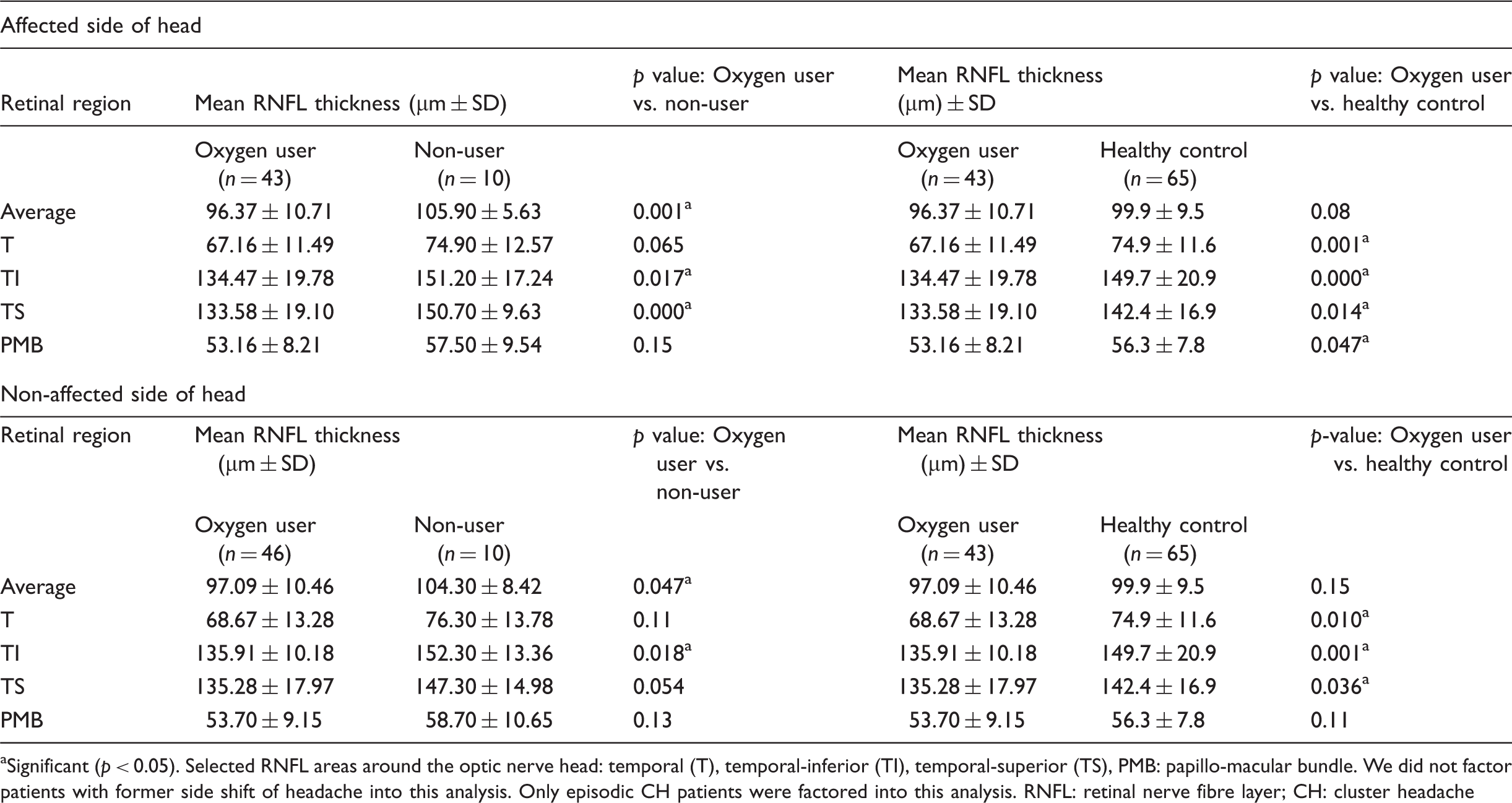
Significant (p < 0.05). Selected RNFL areas around the optic nerve head: temporal (T), temporal-inferior (TI), temporal-superior (TS), PMB: papillo-macular bundle. We did not factor patients with former side shift of headache into this analysis. Only episodic CH patients were factored into this analysis. RNFL: retinal nerve fibre layer; CH: cluster headache
In the analysis of the linear relationship between the retinal thickness parameters and the total amount of oxygen use among all oxygen consumers, the r2 value was ≤0.15 for RNFL parameters and 0.07 for macular volume, i.e. the reduction of retinal thickness was related to the total amount of inhaled oxygen in only 15%/7% of eyes, but our correlation analyses showed that the relationship was statistically significant for four RNFL areas (Table 5). Figure 3 illustrates three corresponding linear regression lines.
Relation between three RNFL thickness parameters on the headache side of 63 oxygen users and the total amount of oxygen use shown by linear regression lines. The total amount of oxygen use (l) was calculated as the product of the total frequency of oxygen use, the flow rate (l/min) and the mean duration of oxygen inhalation (min). r: Pearson correlation coefficient, r2: coefficient of determination, b1: slope of the linear regression line, i.e. the difference of RNFL thickness parameter (µm) and macular volume parameter (mm3), respectively, per 1000 litres of inhaled oxygen, * : significant (p < 0.05). RNFL: retinal nerve fibre layer. Analysis of correlation and linear relationship between RNFL thickness parameters as well as macular volume on headache side of 63 oxygen users and the total amount of oxygen use. Significant (p < 0.05). bb1: slope of the linear regression line, i.e. the difference of RNFL thickness parameter (µm) and macular volume parameter (mm3), respectively per 1000 litres of inhaled oxygen. The total amount of inhaled oxygen (l) was calculated as the product of total frequency of oxygen inhalation, the flow rate (l/min) and the mean duration of oxygen inhalation (min). RNFL: retinal nerve fibre layer; PMB: papillo-macular bundle; T: temporal; TI: temporal-inferior; TS: temporal-superior; N: nasal; NI: nasal-inferior; NS: nasal-superior.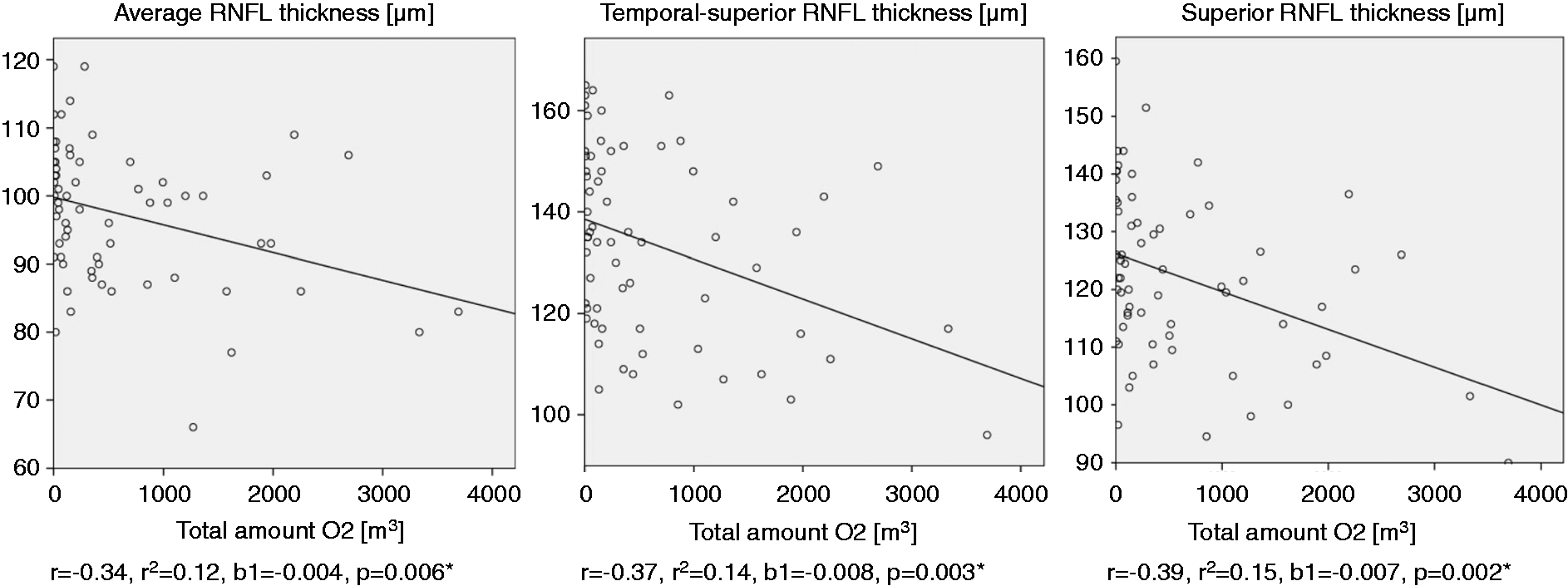

Neither frequent usage of sumatriptan subcutaneously (s.c.) nor verapamil (as frequent prophylactic medication or as medication on examination day) influenced OCT results significantly.
Visual function
Comparison of scores achieved in visual function tests for each eye of headache patients and healthy controls.

Only eyes of patients with best corrected visual acuity of at least 20/20 were included in our analysis of low-contrast letter acuity. Berlin controls were not subjected to examination with Sloan charts. ETDRS: Early Treatment Diabetic Retinopathy Study.
Discussion
A total of 107 CH patients were examined with OCT and compared to 65 healthy controls. RNFL thickness was reduced in the temporal quadrant in both eyes of CH patients compared to healthy controls with predominant thinning in the temporal-inferior area on the headache side.
Temporal retinal thinning affects both eyes of CH patients in spite of strictly unilateral pain and accompanying symptoms in the analysed subgroup without side shifts of headache, which suggests a systemic effect causing these retinal alterations. Studies showing an increase of intraocular pressure, corneal temperature, intraocular blood flow or changes of vessel diameter of eye supplying and draining vessels during headache attacks in most cases found these changes in both eyes but with emphasis on the pain side (8–10). PET and magnetic resonance imaging (MRI) examination during attacks proved bilateral dilatation of ICA and basilar arteries and were interpreted as unspecific pain-induced neurogenic vasoreaction (11). Trigeminovascular activation with delivery of vasodilatating substances like calcitonin gene-related peptide (CGRP) and vasoactive intestinal peptide (VIP) into the bloodstream during CH attacks (25) supposedly also bilaterally influences ocular blood supply. Tissue hyperperfusion of this type might subsequently cause microvascular and thereby tissue damage in the retina. Our finding of higher RNFL parameters in the nasal-inferior and less pronounced also in the nasal-superior area in both eyes of headache patients (Table 2) might be attributed to an inter-attack vasodilatation: Retinal vessels normally contribute to the shape of RNFL, in general, the four local maxima of the RNFL thickness profile correspond to the localisation of the main branches of the blood-supplying vessels. These local maxima show high inter-individual variability (26) and in CH patients, the possible inter-attack vasodilatation influenced particularly nasal-inferior and nasal-superior RNFL area because vessels crossing the peripapillary ring for the RNFL measurement often showed more branches in these very areas. However, programs to analyse and quantify vessel calibre in OCT images are still in the process of development and data are rare.
On the other hand, bilateral retinal alteration may be explained by vasoconstricting medication: Oxygen users showed bilateral thinning in all temporal RNFL areas in comparison to healthy controls (Table 4) with a significant relationship between retinal thickness reduction and the total amount of inhaled oxygen for some retinal areas (Table 5). The considerable thickness reduction of oxygen users vs. non-users must be regarded with reservation considering the small number of non-users (n = 10) and the non-significant (except for nasal-inferior area) but noticeable thickness elevation of non-users vs. healthy controls in most retinal areas for which we found no pathophysiologic explanation.
Multiple studies have affirmed vasoconstriction of retinal vessels in the course of 100% oxygen breathing with reports on the amount of blood flow reduction ranging between 30% (13) and 60% (14). Typical duration of oxygen inhalation of CH patients approximates 20 minutes and Kiss et al. could affirm that retinal vasoconstriction due to oxygen inhalation stays stable over 20 minutes. Over this whole span of time, microcirculation in the retina is altered, showing a pronounced effect of building “trains” of red blood cells with increase of vascular resistance (27).
Moreover, the response to hyperoxia reveals regional differences in retinal tissue: Temporal vessels react with more vasoconstriction than nasal vessels probably owing to a more critical oxygen demand (27) with stricter control of autoregulatory response to changes in local metabolites in the higher metabolic active macula (28). These regional variances in responsiveness to hyperoxia might account for higher susceptibility of the central retina to frequent oxygen inhalation, which can be linked with our finding that especially temporal parts of RNFL are reduced in oxygen users but is not in line with non-altered macular parameters of oxygen users vs. healthy controls and a rather poor coefficient of determination for the relationship between macular thickness and total amount of oxygen use (r2 = 0.07).
In view of the coefficients of determination (r2, Table 5), we can neither act on the assumption that high degree of oxygen usage is harmful in any case nor define a critical value so that some counterarguments to a possible harmful effect of hyperoxia-induced vasoconstriction should be elucidated:
A rise in partial oxygen pressure (pO2) in the periarterial retinal tissue precedes vasoconstriction (29). In addition, delivery of normo- or especially hyperbaric oxygen are therapeutic options in the central retinal artery or vein occlusions, these effects remaining controversial (30,31). The rationale behind this therapeutic intervention is an increase of plasma-dissolved oxygen in the choroidal circulation which lacks strong autoregulation, leading to a higher proportion of the retina being oxygenated by choroidal vessels. It is controversial whether normobaric oxygen delivery – as in CH patients – is sufficient to create a choroidal oxygen supply for the whole retinal thickness (32,33) and in an OCT exam, the innermost retinal layer (RNFL) with greatest distance to the choroid and the layers where the retina shows greatest thickness (close to the posterior pole, macular region) are examined. It is assumed that at 80% oxygen at 1 atm, nearly the whole retinal thickness can be oxygenated by the choroid with the exception of the posterior pole (33), which nevertheless showed no significant thinning in oxygen users vs. healthy controls and no correlation between tissue alteration and the total amount of oxygen use.
Temporally emphasised RNFL thinning can be found in various diseases with optic nerve atrophy (ONA), e.g. post-neuritic optic atrophy in multiple sclerosis (34), toxic and hereditary optic atrophies (35), and might reveal an early state of ONA (36). Boiardi et al. found normal latency and morphology of visual-evoked potentials in CH patients, but P100 amplitude was significantly decreased on the pain side (37), possibly hinting at partial axonal damage in the optic nerve.
Selective temporal RNFL thinning was attributed to a differential vulnerability of the smaller and more thinly myelinated parvo-cellular axons from the papillo-macular bundle building up the temporal RNFL to oxidative stress and energy depletion (35,36).
Illness duration or severity did not determine the degree of retinal structure alterations, similar to the finding of Gipponi et al. concerning retinal thickness reduction in migraine patients (38): They suggested that alternating vasoconstriction and -dilatation of trigeminally innervated retinal vessels accompanying migraine attacks might be responsible for falling below a critical ischemic threshold with consequential ganglionic cell death. This threshold is thought to be genetically determined, which might also be the case for CH patients.
The thinning process seems to be irreversible, as no difference was found between patients with time intervals of more and less than two years since the last bout.
The macular region with its solely diffusion-based blood supply seems to be less resistant to the centrally generated (39) and ongoing processes potentially involved in the chronic type of CH, whereas episodic CH rather tends to affect temporal parts of the RNFL (Table 3).
No decline of visual function was detected in either the whole cohort of CH patients nor in oxygen users. Retinal alterations were not as marked and extensive as for example in MS patients, in whom a good correlation of RNFL thickness as a structural biomarker and visual function measured by Sloan low-contrast letter charts could be affirmed (40,41). Regarding the relatively small, yet significant, reduction in the temporal RNFL, it is no surprise to see no effect in perimetry. Previous studies showed that 30% to 50% of retinal ganglion cells may be lost before an abnormality appears on standard perimetry (42,43).
The prevailing OCT measurements suggest an extension of the pathological process involved in CH to the eye as a region of maximum pain for a high percentage of CH patients, but further investigations will be needed before we can make a statement on the meaning, long-term value and clinical correlates of temporal retinal thinning. A segmentation of retinal sublayers should be initiated in view of their differential oxygen consumption and the differential sensitivity to hyperoxia of their supplying vessels. In addition, an examination of attack-inherent changes of retinal vessel diameter and blood flow should be engaged in by examining patients during attacks with dual-beam bidirectional Doppler FD-OCT if possible.
Clinical implications
We found bilateral temporal retinal nerve fibre loss in cluster headache (CH) patients without correlation to disease severity, duration or visual function decline. Our results might indicate possible harmful potential of frequent oxygen inhalation on retinal integrity which could have greater clinical relevance regarding the wide field of application of 100% oxygen breathing.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interests
C. Ewering, N. Hasal, E.M. Kadas, H. Zimmermann, A. U. Brandt, T. Oberwahrenbrock, and N. Osada have nothing to declare. F. Paul reports support by Bayer (research funding, travel grants, speaker honoraria), BiogenIdec (speaker honoraria, consultancy agreement), Teva (research funding, travel grants, speaker honoraria), SanofiGenzyme (Advisory Board, speaker honoraria), Merck (research funding, travel grants, speaker honoraria), Novartis (Steering Committee, research funding, travel grants, speaker honoraria), MedImmune: Steering committee; supported by German Research Foundation (DFG Exc 257), German Ministry for Education and Research (BMBF Competence Network Multiple Sclerosis). M. Marziniak reports support by Bayer (travel grants, speaker honoraria), BiogenIdec (research funding, speaker honoraria, consultancy agreement), Teva (research funding, travel grants, speaker honoraria), SanofiGenzyme (Advisory Board, speaker honoraria), Merck (research funding, travel grants), and Novartis (Advisory Board, research funding, travel grants, speaker honoraria).
F. Alten: Novartis (Advisory Board), Bayer (travel grant), Allergan (Advisory Board).
C.R. Clemens: Heidelberg Engineering (speaker honoraria), Novartis (funding investigator initiated trial), Bayer (funding investigator initiated trial), Allergan (Advisory Board).
N. Eter: Novartis (research funding, speaker honoraria, Advisory Board), Bayer (research funding, speaker honoraria, Advisory Board), Allergan (research funding, speaker honoraria, Advisory Board), Heidelberg Engineering (speaker honoraria), Bausch and Lomb (Advisory Board), Alimera (Advisory Board).