
Abstract
Objective:
This study aimed to determine the relationship between clinical symptoms and findings of patients diagnosed with conjunctivochalasis in our clinic and the risk factors reported in the literature, to determine new possible etiological factors, and to compare routine tear assessment methods with novel strip meniscometry in these patients.
Materials and Methods:
The study included patients who presented to our clinic between March 2019 and June 2019 and were diagnosed with conjunctivochalasis. The Ocular Surface Disease Index was used to assess ocular surface symptoms. Anterior segment examination included tear break-up time, corneal staining, localization of conjunctivochalasis, and the presence of pinguecula or pterygium. For each patient, tears were measured using both Schirmer and strip meniscometry. Patients with conjunctivochalasis were evaluated as lid-parallel conjunctival folds grade 1, 2, or 3.
Results:
There was a total of 57 participants, including 31 women (54.4%) and 26 men (45.6%). Lid-parallel conjunctival folds grade was found to be statistically significantly associated with dust exposure (p = 0.034). Multiple regression analysis revealed that dust exposure was an independent predictor of being diagnosed with lid-parallel conjunctival folds grade 2 versus lid-parallel conjunctival folds grade 1 (odds ratio = 3.515, p = 0.029). Moreover, Schirmer’s test and strip meniscometry results were positively correlated in patients with conjunctivochalasis (r = 0.302 and p = 0.022).
Conclusion:
We conclude that external factors are prominent in patients with conjunctivochalasis, especially dust exposure. In addition, strip meniscometry may be preferred as a more practical and noninvasive alternative to investigate dry eye symptoms in patients with conjunctivochalasis.
Introduction
Conjunctivochalasis (CCH) occurs due to excess folds of loose conjunctival skin that accumulate between the ocular surface and the lower eyelid and consequently disrupt the distribution of tears on the ocular surface. 1 CCH often affects the eyes bilaterally and is more common in the elderly population. 2 Excess conjunctival tissue may not cause any symptoms, or it may result in ocular irritation. 3 Symptoms include epiphora, blurred vision, foreign body sensation, dry eyes, subconjunctival hemorrhage, and Dellen.4–6 CCH is a common but often overlooked conjunctival disease. 7 Diagnosis is based on clinical examination and patients may be asymptomatic; 8 therefore, a careful examination is crucial to diagnose CCH. 9
The etiopathogenesis of CCH is not fully elucidated, but various theories have been proposed. The mechanical theory suggests that age-related changes in the conjunctival tissue cause chronic lymphatic obstruction, and the subsequent lymphatic dilatation leads to CCH.10,11 The inflammatory theory suggests that the disrupted tear distribution results in the degradation of the extracellular matrix, leading to the accumulation of degrading enzymes in tears and, consequently, inflammatory changes that result in conjunctival laxity. 12
Patients with CCH often describe dry eyes. 13 Schirmer’s test is widely used to determine concomitant dry eyes in patients with CCH. 14 Recently, strip meniscometry was proposed as a more practical, rapid, and noninvasive alternative for tear measurement. 15 Hence, we hypothesized that strip meniscometry could be useful in patients with CCH.
The literature describes numerous etiological risk factors related to CCH, but we believe that there may be further underlying causes. Therefore, our study aimed to determine new risk factors in addition to known etiological causes by reviewing the clinical symptoms and findings of patients diagnosed with CCH. We also aimed to compare Schirmer’s test and tear break-up time (BUT) measurements, both commonly used tear assessment methods, with strip meniscometry among patients with CCH.
Materials and methods
This prospective observational study included patients who presented to the Meram Faculty of Medicine Hospital’s Ophthalmology Outpatient Clinic between March 2019 and June 2019 who were diagnosed with CCH. This study was granted ethical approval by the Necmettin Erbakan University Meram Medical Faculty’s Medical, Surgical, and Pharmaceutical Research Ethics Committee (No: 2019/1845).
The study included 57 eyes of 57 patients aged 18 and over who were diagnosed with CCH. All patients gave written consent before the study participation. The patients underwent routine ophthalmological examination. Patients’ age, gender, occupation, known systemic diseases, smoking status, and used medications were recorded. Patients were asked to evaluate dust exposure in their respective work environments as ‘very often’, ‘often’, ‘sometimes’, or ‘never’. Any eyelid disorders were recorded.
Refractive error was measured using an autorefractometer (Topcon® KR 8100 Auto Kerato-Refractometer). Axial length was measured using an optical biometer (IOL Master ZEISS®). The anterior segment was examined with a biomicroscope to determine corneal staining and localization of CCH. Corneal staining was evaluated using fluorescein eye stain-containing paper, which was touched to the surface of the eye, and a slit-lamp biomicroscope. Positive corneal and conjunctival fluorescein staining was graded according to the OXFORD scale. 16
CCH was graded according to the LIPCOF (lid-parallel conjunctival folds) classification proposed by Höh and colleagues. 17 Accordingly, the participants were divided into three groups as LIPCOF grade 1, 2, and 3. We also evaluated the number of conjunctival folds and their positions relative to the tear meniscus. Localization of CCH was noted as central, inferior, nasal, temporal, and mix regions. 11
Tear volume was also measured with strip meniscometry using nitrocellulose membrane filter paper strips (SM Tube® Strip Meniscometry Tube). 15 The meniscometry strip was briefly inserted for 5 s into the lateral lower one-third of the tear meniscus without touching the ocular surface. The length of the stained tear column in the central membrane ditch was read with the aid of the scale marks printed on the strip and results were recorded in millimeters (mm). The cutoff value of the Strip meniscometry was used as ⩽4 mm.15,18
Tear BUT was determined using fluorescein eye stain and a BUT of <10 s was evaluated as abnormal. Schirmer’s test was performed without anesthesia to measure reflex tear secretion and the results were evaluated along with tear BUT in the dry eye examination. 19
The Ocular Surface Disease Index (OSDI) was applied to determine the severity of dry eye disease. 20 The OSDI consists of 12 items and evaluates patients’ dry eye complaints (ocular symptoms, vision-related function, and environmental triggers) over the last 2 weeks. The items are scored from 0 (‘none of the time’) to 4 (‘all of the time’), and the total OSDI score is calculated as follows:

The maximum OSDI score is 100 and the minimum is 0.
Statistical analysis
The normality of continuous data distribution was evaluated using the Kolmogorov–Smirnov test. The homogeneity of variance assumption was evaluated using Levene’s test. Descriptive statistics were expressed as mean ± standard deviation and median [interquartile range (IQR)] for numerical variables and as numbers (%) for categorical variables. For continuous numerical variables where parametric assumptions were met, the significance of the difference between the groups was examined using one-way analysis of variance (ANOVA). For ordinal variables and for numerical variables where parametric assumptions were not met, the significance of the difference between the groups was examined using the Kruskal–Wallis test. If the Kruskal–Wallis test results were statistically significant, the Dunn–Bonferroni multiple comparison test was performed to determine the group(s) that caused the difference. Categorical variables were evaluated using Pearson’s chi-square or likelihood ratio tests. Any statistically significant relationship between continuous numerical variables was investigated using Spearman’s correlation test. The combined effects of all possible factors that could distinguish the LIPCOF grade 1 group from the grade 2 or grade 3 groups were examined using multinomial logistic regression analysis. Variables with a p-value of less than 0.1, as determined by univariate analysis, were included in the multivariable model as candidate variables. Moreover, odds ratios (ORs), 95% confidence intervals, and Wald statistics were calculated for each variable. Data were analyzed using SPSS version 22.0 (IBM Corp.®, Armonk, NY, USA). Values of p <0.05 were considered statistically significant unless otherwise indicated.
Results
There was a total of 57 participants, including 31 women (54.4%) and 26 men (45.6%). The mean age of the participants was 59.7 ± 12.3 years. Among the participants, 27 (47.4%) were housewives, 10 (17.6%) were civil servants, 8 (14.0%) were blue-collar workers, 8 (14.0%) were farmers, and 4 (7.0%) were self-employed. Forty-one participants (71.9%) indicated working indoors and 16 (28.1%) indicated working outdoors. Twenty-three participants (40.4%) had no concomitant systemic diseases, while 17 (29.8%) had hypertension, 16 (28.1%) diabetes, and 3 (5.3%) coronary artery disease. Fourteen (24.6%) participants had a history of smoking (Table 1).
Demographic and clinical characteristics of the patients.

BUT, break-up time; LIPCOF, lid-parallel conjunctival folds; OSDI, Ocular Surface Disease Index.
The comparison of participants’ demographic and clinical characteristics according to LIPCOF grades is presented in Table 2. There were no statistically significant differences between the groups in terms of average age, gender, smoking history, eye rubbing, or axial length (p > 0.05). LIPCOF grade was found to be significantly associated with dust exposure (p = 0.034). Multiple regression analysis revealed that dust exposure was an independent predictor of being diagnosed with LIPCOF grade 2 versus LIPCOF grade 1 (OR = 3.515, p = 0.029). Dust exposure was higher among grade 3 patients compared with the grade 1 group, but this finding was not statistically significant (p = 0.118) (Table 3).
Demographic and clinical characteristics of the patients according to the LIPCOF classification.

ANOVA, analysis of variance; LIPCOF, lid-parallel conjunctival folds.
One-way ANOVA.
Pearson’s chi-square test.
Kruskal–Wallis test.
Values given in bold indicate statistically significant results (p < 0.05).
Logistic regression analysis of covariates with the LIPCOF classification.
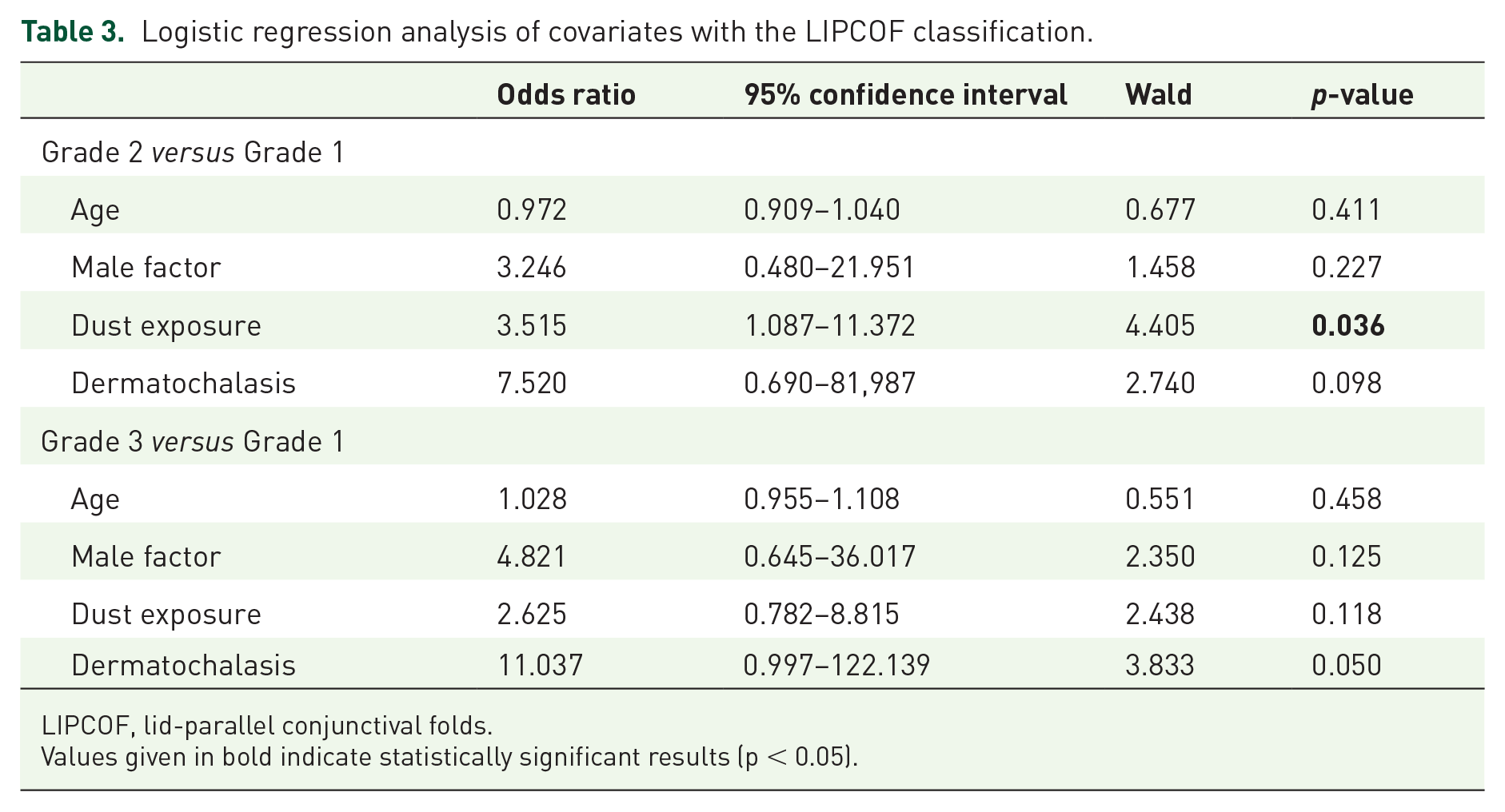
LIPCOF, lid-parallel conjunctival folds.Values given in bold indicate statistically significant results (p < 0.05).
The correlation coefficients between BUT, Schirmer’s test, strip meniscometry, and OSDI scores and their significance are given in Table 4. BUT was significantly positively correlated with Schirmer’s test results (r = 0.382 and p = 0.003) but was not correlated with strip meniscometry or OSDI (p = 0.402 and p = 0.131, respectively). Schirmer’s test results were significantly positively correlated with strip meniscometry results (r = 0.302 and p = 0.022). However, OSDI was not found to be statistically correlated with Schirmer’s test (p = 0.616) or strip meniscometry (p = 0.221).
Correlation coefficients and significance levels between BUT, Schirmer, Strip meniscometry, and OSDI scores.

BUT, break-up time; OSDI, Ocular Surface Disease Index.
Spearman’s correlation test.
Values given in bold indicate statistically significant results (p < 0.05).
Discussion
We found that external factors are prominent in patients with CCH, especially dust exposure. In addition, strip meniscometry is a noninvasive, rapid, and reliable alternative for the assessment of dry eye findings in patients with CCH. To the best of our knowledge, our study is the first in the literature to investigate these parameters.
As is known, CCH can affect young people, but it most often affects the older population. Zhang and colleagues 21 studied 2110 Chinese individuals aged 60 years or older and found the prevalence of CCH as 44.08% in this population. A Japanese study reported that increased age was associated with increased CCH prevalence. 22 Similarly, our subjects primarily included elderly individuals.
Environmental factors such as dust exposure, ultraviolet light, dryness, and heat are thought to play a role in the formation of pterygium and pinguecula. 23 That said, in our review of the literature, we did not come across any publication that mentioned a direct relationship between CCH and dust exposure. In our study, we found that participants with LIPCOF grade 2 CCH were more likely to be subject to dust exposure than those with grade 1 CCH. It is well established that environmental dust is associated with increased foreign body exposure in the orbit, and the subsequent ocular irritation can trigger inflammation in the eye. 24 The frequent triggering of inflammation due to chronic dust exposure can lead to CCH development. However, when grade 3 CCH was compared with the control group, it was not reaching statistical significance. Disparities in our research findings on the potential association between dust exposure and CCH can be explained, at least in part, by a variety of confounding factors that would be more dominant in the later stage. Although further research on a causal relationship is required in a later stage of CCH, our study provides an opportunity to reveal the link between CCH and dust exposure in an earlier phase of the disease.
Numerous studies report that dry eye disease and CCH are often observed together.17,25 However, the relationship between CCH and dry eye has not been fully elucidated. The current opinion is that CCH does not cause dry eye but produces dry eye symptoms. 13 In addition, the shared risk factors in dry eye disease and CCH, such as aging and female gender, may explain their high comorbid occurrence. 26 Similar to previous studies, we found that dry eyes and CCH were often comorbid. However, further studies are needed to demonstrate any causal relationship between these two conditions.
Schirmer’s test is considered the gold standard for assessing tear volume.19,27 However, it can result in complaints such as pain, stinging due to irritation, and reflex tear secretion. 28 Dogru and colleagues 15 proposed the rapid strip meniscometry method as an alternative to Schirmer’s test. This novel method is a simple and noninvasive option that can measure tear meniscus volume, and it can be used for the diagnosis, screening, and assessment of dry eye disease.18,29 In addition, in a previous study, it was demonstrated that the sensitivity and specificity of strip meniscometry were determined as 83.5% and 58.1%, respectively, and specificity significantly increased when combined with Schimer’s test. 18 In our study, strip meniscometry was also positively correlated with Schirmer’s test results. In light of this information, we can say that strip meniscometry can be used as an alternative to Schirmer’s test.
The limitations of our study include its small sample size and the single-center design. Also, due to the cross-sectional design, we were not able to evaluate the effects of the duration of CCH or its changes over time. The strengths of our study are having taken detailed anamnesis and measurements and meticulously determining CCH symptoms and findings. In addition, this is the first study to investigate the utility of the novel strip meniscometry method of tear measurement in patients with CCH.
We conclude that external factors are prominent in patients with CCH, especially dust exposure. Strip meniscometry may be preferred as a more practical and noninvasive alternative to investigate dry eye symptoms in patients with CCH.
Footnotes
Acknowledgements
This article was written using the data from the specialty thesis called ‘Clinical Signs and Symptoms of Patients with Conjunctivochalasis’ submitted to Meram Faculty of Medicine.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.