
Abstract
Purpose:
The purpose of this report is to quantify how pressure applied to the human cornea, either physiological or intentional, affects its curvature. In particular, how pneumatic procedures flatten the central cornea and keep it flat over time, thereby decreasing the patient’s myopia.
Methods:
A viscoelastic model is developed for plastic deformation which gives us the basic governing equations of the elastic and plastic strain of corneal stroma. The model is applied to data from corneas of six patients who underwent pneumatic keratology (NEumatica Keratologia) to reduce their myopia.
Results:
The model shows corneal dimensional stability for long periods of time after NEumatica Keratologia that decay with an exponential time constant. Separate equations are developed that relate corneal plastic strain to the pressure applied and its duration ε = σ0 t1/η1, to change in refraction ε = 2 × ΔRefr, to keratometry radius increase ε = ΔR/R, and to corneal thinning ε = sqr (Δh/h). The average values obtained for ε from the patients’ data are 3%, 3.2%, 3%, and 2.6%, respectively, all in remarkable agreement. The average refraction change is found to remain stable at ΔRefr = +1.67D ± 5.2%. Clinical data yield good agreement of theory and treatment results.
Conclusions:
The model proposed is a good description of NEumatica Keratologia outcomes. Practical applications include the long-term stable correction of myopia with refractive procedures. High myopia subjects can benefit from this procedure because NEumatica Keratologia corrects and protects the central cornea radius by stretching the peripheral cornea.
Introduction
The current myopia epidemic is a serious problem, which will only subside when its cause is met. In short, it is now apparent that while the initial, usually low myopia of individuals with natural accommodation is probably a matter of inherited properties, 1 progressive myopia is caused by the continuous feedback effect of negative lenses. 2 An immediate way to focus the myopic blurred retinal image is achieved with corrective lenses or various refractive procedures, laser-assisted in situ keratomileusis (LASIK) being the most widely used at present.3,4
Many types of procedures involve changing the central radius of curvature of the cornea to bring to focus the image in an eye with refractive error, usually myopia. Most notable of these procedures include LASIK, orthokeratology (OK), and the pneumatic keratology [NEumatica Keratologia (NEK)] procedure discussed in this article. It is of prime importance to maintain dimensional stability of the cornea for long periods of time after these various types of procedures that change its anatomy. We show here that NEK produces myopia reduction stable over time.
Pneumatic keratology is a procedure to flatten the cornea noninvasively. Medina 5 applied a vacuum force for 5 min to flatten the central part of the cornea by distending the stressed peripheral areas where a vacuum is applied. Unlike LASIK, NEK does not remove any tissue but relies on the mechanical properties of the cornea to deform it plastically. The NEK procedure stretches the cornea circumferentially, the same as radial keratotomy (RK) incisions extend the cornea perpendicular to the axis of the incisions. The NEK instrument is portable and its effect is permanent myopia correction. Because of its simplicity, portability, and low cost, NEK is superior for use in remote areas and in the world.
Refractive surgery is dependent on the mechanical properties of the cornea. The collagen in the corneal stroma is a complex biomaterial that exhibits viscoelasticity, plasticity, and creep under stress, whether external or physiological. Any attempt to modify the cornea and predict its stability afterward requires knowledge of its mechanical properties. Classical texts by Fung 6 and Ferry 7 provide basic equations and examples of the viscoelastic biomaterials. Nash and colleagues 8 present viscoelastic data for human and rabbit cornea, showing creep strain rates of 0.6% per hour at slightly elevated temperature and stress level. Nash and colleagues 8 and Ku and Greene 9 present data of the stress of the cornea and the sclera and resulting creep strain-rate. Rand and colleagues 10 model the mechanical effects of RK surgery on the cornea using thin-shell theory. Andreassen and colleagues 11 measure the high-stress Young’s modulus for human cornea. Models of the elastic properties of the cornea have been proposed by Glass and colleagues. 12 McMonnies and Schief 13 show how midperipheral external forces can change the curvature of the central cornea.
The purpose of this article is to integrate its reversible and irreversible mechanical properties into a cornea model. The model can be useful to predict the temporary and permanent corneal deformation after intentionally applied stress, such as from NEK and nonintentional stress, such as post-LASIK.
The corneal collagen is a fibrous protein with an organization similar to polymer fibers. Model corneas have been fabricated using polymers. 14 After removal of stress to the cornea, the stretched and distorted collagen fibers between cross-link points act like springs that tend to cause the prior deformation to partially recover (regress) with time. Some recoverable (reversible) viscous deformation occurs in addition to the nonrecoverable (irreversible) portion as shown in Figure 1. This partial recovery is more complex than simple viscous behavior. The simplest rheological model of the cornea that combines elastic, creep, and transient viscoelastic recovery is proposed here. This minimum-complexity model of the cornea accounts for both its elastic and plastic properties. A similar model has been proposed to approximate the behavior of polymers. 15

NEK applied corneal stress σ0 of duration (t1 − t0) = 5 min (lower trace). Resulting strain ε(t) as a function of time t, as observed and predicted by our model, showing elastic ε0 and plastic εplastic. strain (upper trace).
Materials and methods
Six human eyes were treated with the NEK device, which evacuated air in front of the cornea for 5 min thereby plastically deforming the cornea to a flatter radius. The vacuum stresses the region of the cornea in contact with the vacuum chamber with a transmural pressure of 775 mmHg. Central corneal radii R were recorded with a topographic keratometer (Zeiss 9000 Series) at three points in time (1 day, 2 months, and 2 years) after the procedure. Subjective and objective refraction and visual acuity were recorded from each patient before the procedure and 1 day, 2 months, and 2 years after the procedure. Corneal thickness was measured with a pachymeter accurate within <1%. Because the NEK device increases the volume of the anterior chamber during application, the intraocular pressure (IOP) did not increase intraoperative. Consistently, the patients, who had usable vision through the device window, did not experience vision blackout that could have been the result of high IOP. The window in the device was used to align the device with the pupil. The pre-op and post-op IOP was not significantly different and was within the normal range. Protocol details can be found in Medina. 5 This report includes data from an additional patient who underwent NEK after 2017. The room temperature during the procedure for all six patients was 25°C, refraction and corneal radii were obtained twice and their values averaged. The ages of the patients were 30, 31, 37, 42, 46, and 50 years. Corneal thickness was measured with a pachymeter in the center of the cornea and in the midperiphery, nasal, temporal, superior, and inferior quadrants; the four peripheral values were averaged and reported here as the peripheral thickness. Central corneal thickness for all patients was 0.49–0.67 mm, average 0.58 mm pre-op and 0.47–0.61 mm, average 0.54 mm post-op. The peripheral corneal thickness for all patients was 0.56–0.70 mm, average 0.62 mm pre-op and 0.48–0.65 mm, average 0.56 mm post-op. All procedures performed in this study were in accordance with the ethical standards of the institutional review board of the Hospital de la Cruz Roja in Barcelona, IRB approval number 5148, and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study. Drs Fariza and Medina performed the NEK procedures. For purposes of this report, approval was waived in as much as it involves analysis of data collected in a previously approved and reported study. 5
The cornea was subjected to a pulse stress σ0. The expected viscoelastic response of the cornea subjected to a NEK stress pulse is shown in Figure 1. As any viscoelastic material, it experienced a time-dependent increase in strain. This phenomenon is known as viscoelastic creep. At time t0, a circumferential ring of the cornea is loaded with a tangential constant stress σ(t0) = σ0 from a vacuum. The treated corneal ring responds to the stress with a circumferential strain ε(t) that increases as shown in Figure 1 until t1, when the vacuum is removed. The applied pulse had a duration (t1 – t0) of 5 min.
After t1, the cornea slowly recovers some of its original shape until reaching a permanently deformed larger ring of residual strain εplastic, the plastic strain that is reported here for our subjects. The elastic strain ε0 is reversed (recovered) immediately upon the removal of vacuum at t1, whereas the transient strain
The strain of any portion of the cornea under a chamber of the NEK device has a circumferential and a polar component as shown in Figure 2, when subjected to the transmural pressure. The circumferential strain ϵϴ results in an accumulated strain for the whole circumference of approximately equal value when considering all chambers. We show here that this strain flattens the cornea. We will refer here to ϵϴ simply as ϵ, the strain of interest.

Polar (along a corneal meridian) and circumferential (along the circle of latitude of the peripheral cornea treated) strains ϵϴ and ϵφ, respectively, on a trapezoidal portion of the cornea treated with NEK corresponding to a chamber of the device. Several adjacent chambers in the device cover and stretch the entire circle of latitude.
Figure 3 shows the model for viscoelastic deformation of the cornea during and after NEK that can provide the observed response in Figure 1. After the vacuum and therefore stress is removed at t1, the elastic strain
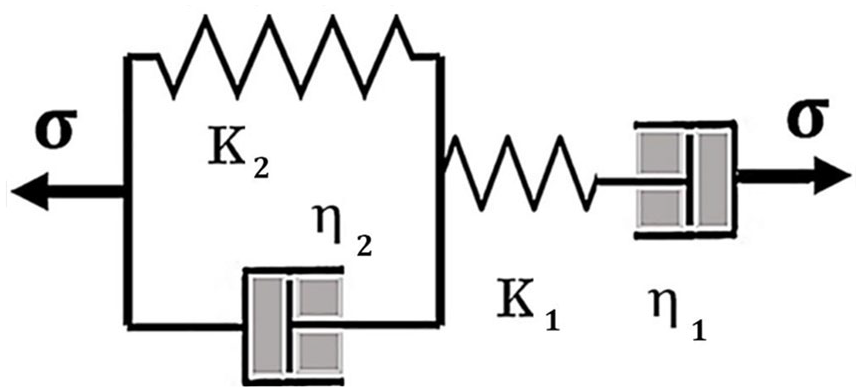
Model for cornea elastic-plastic deformation, elastic springs of moduli K1 and K2, dashpots of viscosities η1 and η2.
We used the model in Figure 3 to analyze the data and obtain the resulting values for the elements of the model. Once the elements are known, we can predict how the cornea will respond to NEK and to other corneal procedures.
The model can be reduced to two equations for strain after application of NEK:

where ηeq = (η1 η2)/(η1 + η2).

where εplastic = σ0 t1/η1 and τ = η2/K2.
Equations (1a) and (1b) are obtained in derivation I in the Supplemental Material. The corneal stability factor after treatment is quantified as viscoelastic strain (equation (1b)). This strain stabilizes with time constant τ.
The model does not include a friction element for simplicity and because it is negligible compared with the stress applied by NEK. A friction element prevents the continuous strain of the cornea under low, physiological stress.
Results
During and after the NEK procedure, the cornea was strained circumferentially along the vacuum chambers of the device as predicted. Immediately after NEK the residual strain is about 2–10%, as estimated theoretically and measured experimentally (see derivation II in the Supplemental Material). The stressing force reduced the thickness of the cornea. The thickness of the cornea was reduced by an average of 7.1% in the center and 9.8% in the midperiphery 1 day after the procedure.
Subsequent to NEK procedures, the cornea remained dimensionally stable during the follow-up period of 2 years. The mean corneal radius for our subjects (N = 6) was <R> = 7.6 mm before the procedure and increased <ΔR> = 0.23 mm as measured 2 years after the procedure. Table 1 displays the spherical refraction value for each patient rather than the spherical equivalent because the cylindrical component was small (1D or less) and remained essentially unchanged after the procedure. 5 The change in the spherical component assesses the treatment efficacy under those circumstances. Only corrected acuity is displayed; uncorrected acuity was not measured. Because the patients’ myopia ranged from about 3D to 20D, their uncorrected acuity was very low and it was not feasible to obtain a measure with a Snellen chart. Corrected distance visual acuity (CDVA) after the procedure was equal or better than before it. CDVA, in decimal notation, remained constant at post-op, or improved with respect to pre-op values at CDVA = 0.98 ± 0.14 SEM (see Table 1). The average effect of the NEK procedure measured by clinical refraction was a reduction in myopic refraction <ΔRefr> = 1.67D 1 day after the procedure and regressed less than 0.37D after 2 years as shown in Figure 4.
Pre- and Posttreatment Corneal Radii, Spherical Refraction, and Snellen Corrected Distance Visual Acuity.

CDVA, corrected distance visual acuity; SEM, standard error of the mean.
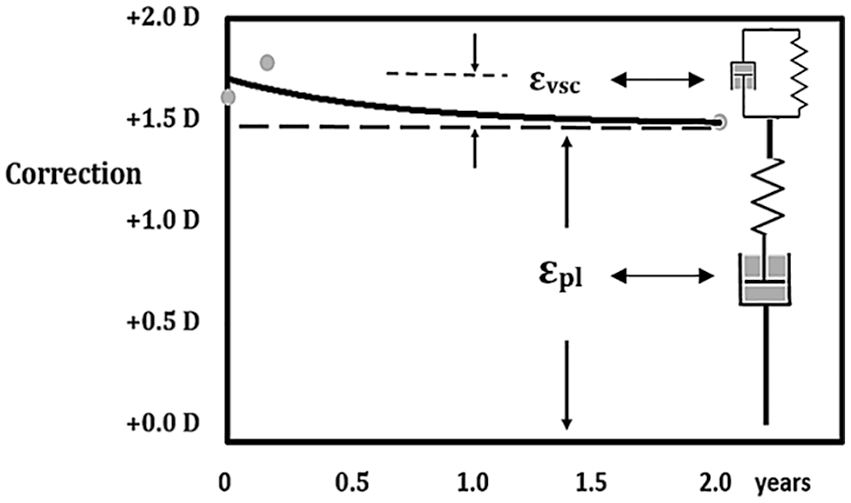
Slow exponential regression of myopia correction has a time constant τ = 0.56 years after NEK for human eyes with moderate and high myopia (r = 0.96, p < 0.001, N = 5).
Table 2 presents data from N = 6 human subjects and the calculated σ0, εpl, η1, τ, K2, and η2 from average data using our model. In Table 2, equation (T1) is Laplace’s law, which allows calculation of stress for a spherical membrane of radius R and thickness h under pressure P. Equation (T2) relates corneal strain to changes in corneal radius (derivation II). Similarly, equation (T3) relates corneal strain to changes in thickness (derivation I). Equation (T4) allows calculation of corneal strain, as a function of refractive change (derivation II). Equation (T5) obtained in derivation I gives the strain from the pressure and duration of the vacuum. Equation (T6), derived empirically relates the Kelvin and Maxwell viscosity coefficients. Equation (T7), obtained in derivation I, allows calculation of Kelvin elastic modulus, from the phase II time constant and the Kelvin viscosity coefficient (Figures 5 and 6).
Mechanical Constants for Human Corneas In Vivo.
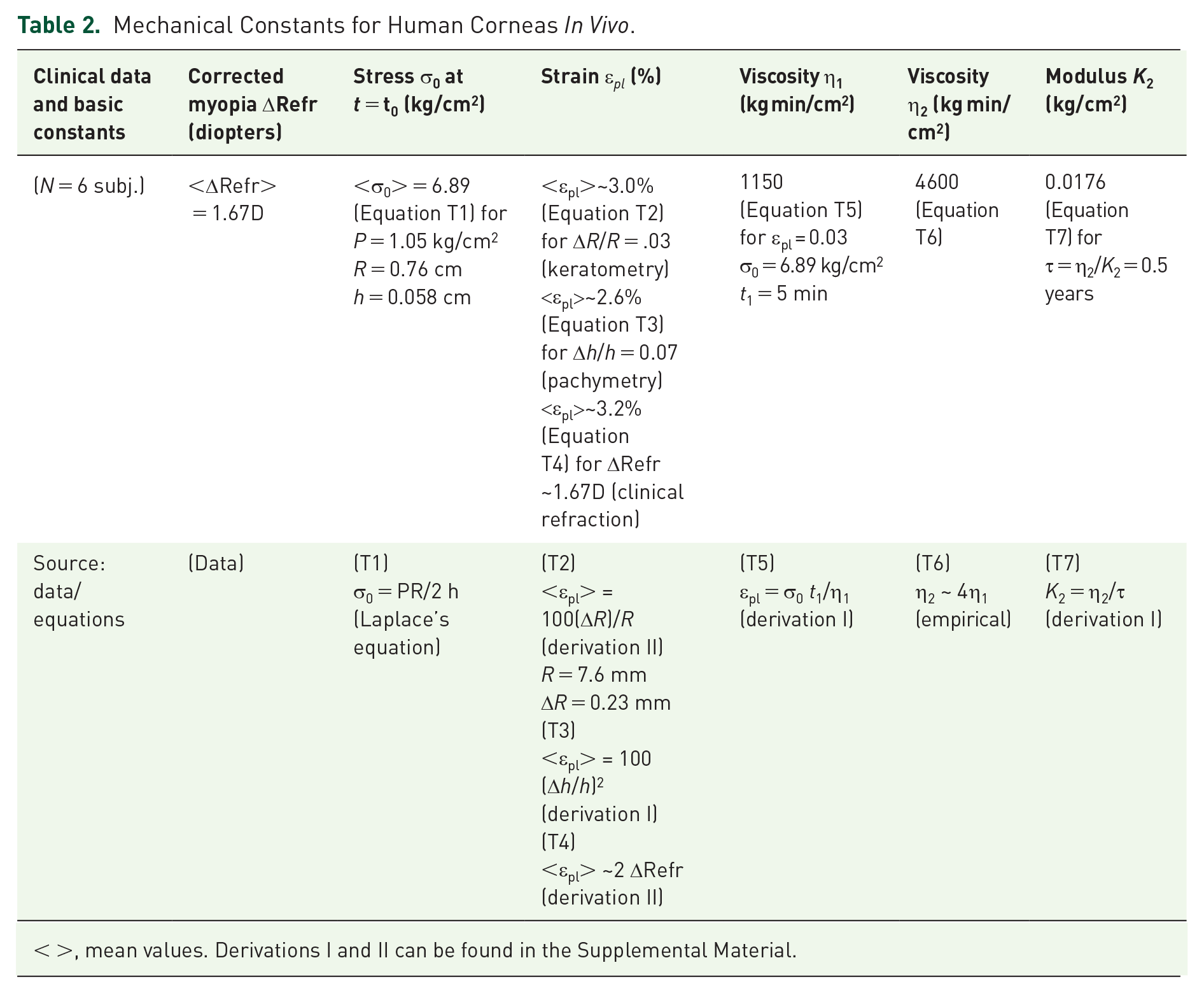
< >, mean values. Derivations I and II can be found in the Supplemental Material.

During the 5-min vacuum stretch, only the components of constants K1, η1, and η2 are considered, so the four-component system reduces to the familiar Maxwell model.
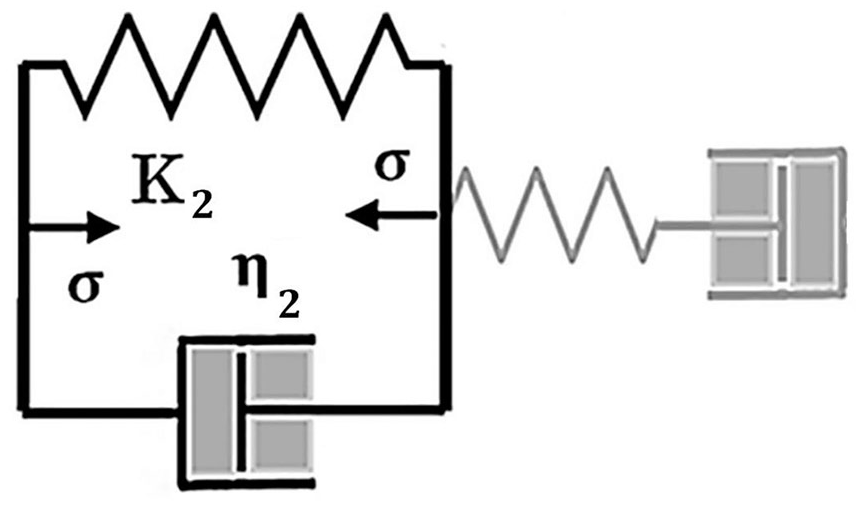
During phase II, the vacuum stress is absent, with only the Kelvin viscoelastic components K2 and η2 responding with slow recovery.
Discussion
To date, the NEK procedure can achieve myopia reversal and correction of 1–5 diopters in 5 min. The model indicates that additional correction will be proportional to the duration and magnitude of applied pneumatic stress as observed in rabbits. 5 We can confirm that the NEK procedure flattens the corneal curvature without increasing the anterior-posterior length of the eye (direction z in Figure 2) because the strain derived from refraction is about the same as measured by keratometry and pachymetry.
The strain calculated and measured by three different methods, as described in Table 2, are all in remarkable agreement. The strain numbers and constants calculated here nevertheless must be taken with caution because of the relatively high stress that NEK applies to the cornea. The cornea was subjected to pressure that is greater than normal IOP by a factor of 50×. Some of the formulation we relied upon has never been applied to high levels of plastic strain.
As reported, the NEK plastic strain technique has achieved up to 5 diopters of myopia improvement per treatment, whereas LASIK is normally used for up to 10 diopters (LASIK, however, is not intended for repeated procedures). In addition, while remaining essentially stable for a period of 2 years following treatment, there is some observed regression after NEK. This result indicates long-term stability, showing that the treated region of the cornea does not continue stretching after NEK. Other procedures like RK and LASIK have resulted on occasion in a post-op progressive stretch, evidenced as development of hyperopia and ectasia, respectively. Ectasia is a serious LASIK complication with prevalence of <0.6%. 16 It is caused by creep of the cornea after it is thinned by LASIK. Early LASIK models and algorithms assumed a rigid structure for the cornea disregarding the biomechanical response of the cornea to the ablation. 17 They were, therefore, unable to predict ectasia. The stressing pressure that causes ectasia is the continuous post-op IOP. NEK does not have this complication because the strength of the cornea is not mechanically compromised as in RK and LASIK. The observed thinning of the cornea after NEK (7%) is insignificant compared with LASIK (15–50% including flap). A percent of tissue altered >40% at the time of LASIK is significantly associated with the development of ectasia. 18 The analysis of creep in this report during NEK is applicable to ectasia and could provide a better and individualized prediction of ectasia risk.
Limitations
Some potential limitations of NEK and this study should be mentioned. Each diopter of myopia improvement requires approximately 2% plastic strain of the circumferential cornea, as determined in derivation II. More work remains to be done to accurately find the safety limit and to achieve plastic strain within this limit. Results from other experiments confirm that increased temperature, duration, or pressure as well as repeat treatment can at least triple the corrective effect reported here. Although no fundus changes were observed after the NEK procedure, increased exposures to the pneumatic stress (in duration or pressure) for augmented response may entail additional safety hazards. The possibility of inducing retinal tears must be considered in those cases requiring large corrections, which intrinsically have a risk of retinal tears. No correlation was observed between age and treatment effectiveness, but the number of patients is small to arrive at firm conclusions. It was however clear that the refractive change depended on the degree of myopia, probably due to the combined effect of the reduced corneal thickness and longer size of the eye, characteristic of higher myopia. See equations (T1) and (T7). The highest correction that can be safely accomplished with NEK is not addressed in this study.
Knowledge of basic corneal viscoelastic parameters may prove fundamentally important to evaluate long-term patient tolerance and the successful outcome of various refractive procedures. An important result of the NEK procedure is the determination of each patient’s viscoelastic parameters, notably viscosity η1. That knowledge could also be used to plan refined repeat treatment with NEK.
In general terms, the series elastic element K1 corresponds to the collagen fiber elasticity, while the parallel elastic element K2 corresponds to the proteoglycan matrix elasticity. The dashpots η1 and η2 quantify the relative slippage of the fibers with respect to each other and with respect to the matrix. Prior knowledge of these viscoelastic parameters will help determine the eligibility of the patient for this type of procedure, the recommended NEK pulse duration (t1–t0), and the applied pressure amplitude ΔP required to achieve a given refractive improvement ΔRefr and the likelihood of dimensional stability into the future.
Some clinical considerations are notable. The relatively new NEK procedure is compared with other more conventional types of corneal refractive surgery (e.g. LASIK). NEK is basically a noninvasive operation; its procedure requires a minimum of clinical personnel and can be administered by an ophthalmologist or optometrist with minimal training and using equipment no more complicated than a tonometer.
The patients’ response to the NEK procedure was uneventful. None of the six subjects as detailed here reported any complications or adverse effects from the 5-min NEK vacuum procedure. None reported any physical irritation, dry eye syndrome, excessive tear film, halos, starbursts, night vision glare and problems often associated with other types of refractive surgery. Visual examination of the corneal surface using a slit-lamp revealed only minor surface imperfections, which quickly return to normal over the course of a few days. Perhaps most importantly, none of the subjects had their visual acuity degraded; CDVA remained the same or improved with respect to pre-op values.
Perhaps the most significant feature of the NEK procedure is that it is quite cost-effective compared with other types of refractive surgery (comparable in cost with Ortho-K) in terms of initial capital outlay for equipment, number of subsequent patient visits, and overall cost for each procedure. NEK may serve as a cost-effective, permanent, and portable method of myopia correction.
The model we propose explains the plastic deformation of the cornea after stress and subsequent partial recovery, features that other models 19 cannot explain. The basic utility of the model is that it provides a structural framework for understanding and predicting the patient’s corneal response to various applied loads. In particular, there can be large intersubject differences in their elastic and viscoplastic parameters. The model is a valuable tool to evaluate a patient’s tolerance and response to various types of refractive surgery.
Supplemental Material
Supplementary_Material – Supplemental material for Plastic modification of human cornea in vivo: applications to clinical refractive procedures
Supplemental material, Supplementary_Material for Plastic modification of human cornea in vivo: applications to clinical refractive procedures by Antonio Medina and Peter R. Greene in Therapeutic Advances in Ophthalmology
Footnotes
Appendix 1
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.