
Abstract
Purpose:
To evaluate the analgesic effect of topical 0.1% nepafenac solution during intravitreal Ozurdex injection.
Methods:
This prospective, randomized, double-blind placebo-controlled study included 59 patients who were diagnosed with retinal vein occlusion or pseudophakic cystoid macular edema and were selected to receive intravitreal Ozurdex injection. The patients were divided into two groups. Group 1, consisting of 31 eyes of 31 patients, received topical 0.1% nepafenac with topical anesthesia (0.5% proparacaine HCl, Alcaine; Alcon, TX, USA), and group 2, consisting of 28 eyes of 28 patients, received placebo with topical anesthesia.
Results:
There were 14 (45.2%) men and 17 (54.8%) women in group 1 and 16 (57.1%) men and 12 (42.9%) women in group 2. The mean age of the subjects was 64.42 ± 5.51 years in group 1 and 62.32 ± 7.54 years in group 2. The median visual analog scale pain score was 2 (1–3) in group 1 and 4 (1–6) in group 2. The visual analog scale pain score was significantly lower in group 1 than in group 2 (p < 0.001).
Conclusion:
Topical 0.1% nepafenac has an additive analgesic effect when combined with topical anesthesia for intravitreal Ozurdex injection.
Introduction
Intravitreal injection (IVI) is commonly used to treat ocular pathologies that require effective drug supply to the back of the eye. Although IVI has been used for years for intraocular delivery of antibiotics to treat endophthalmitis, 1 nowadays they are used to inject steroids for intraocular inflammation 2 and antivascular endothelial growth factor agents for macular edema in diabetic retinopathy, 3 retinal vein occlusion (RVO), 4 and neovascularization in age-related macular degeneration. 5
IVIs may be the most performed procedure in ophthalmology. Numerous studies have reported the rate of pain related to IVI.6,7 Some of them evaluated the pain related to a single injection, whereas others evaluated the pain associated with repeated injections. Therefore, it requires anesthesia like other ophthalmic procedures. Usually, more than one injection is required in most patients, and it may cause anxiety and discomfort, which may also increase the risk of complications. This worrisome condition decreases the treatment compliance of patients who require more than one injection, as in diabetic macular edema and age-related macular degeneration.
Ozurdex (Allergan Inc., Irvine, CA, USA) is a dexamethasone drug delivery system. It is an intravitreal device of 6 mm in length and 0.46 mm in diameter that contains 0.7 mg of dexamethasone and is inserted into the vitreous cavity with a 22-gauge needle. It is used to treat macular edema secondary to RVO as well as diabetic retinopathy, noninfectious uveitis, and pseudophakic cystoid macular edema (PCME; Irvine–Gass syndrome).8–10
Nepafenac ophthalmic suspension is a topical ocular nonsteroidal anti-inflammatory drug (NSAID). Although it is approved to treat inflammation and pain after cataract surgery, it has also been used to treat exudative age-related macular degeneration, prevent cystoid macular edema, and reduce diabetic macular edema.11–13 It is metabolized into its active form, amfenac, because it is a prodrug. Studies have shown that nepafenac had greater inhibition of prostaglandin synthesis, longer duration, and greater corneal penetration than diclofenac. 14 Nepafenac is a more potent at inhibiting COX-2 than bromfenac and ketorolac. 15
Today, there is still controversy regarding the most effective procedure of anesthesia for lessening disruption and pain during IVI. Previously, several local anesthetic techniques for IVIs have been compared, including topical eye drops, gel, peribulbar injection, and subconjunctival injection.7,16–18
In this study, we aimed to evaluate the analgesic effect of topical 0.1% nepafenac in patients undergoing intravitreal Ozurdex injection.
Materials and methods
This prospective, randomized, double-blind placebo-controlled study included 59 patients who were diagnosed with RVO or PCME and were selected to have intravitreal Ozurdex injections. The research was confirmed by Institutional Review Board and all concerned patients had provided informed consent in keeping with the Helsinki Declaration.
Patients with a major psychiatric disorder, dementia, or other neurological diseases affecting memory and cognitive function; diabetic patients with known peripheral neuropathy; or a previously known allergic reaction to the agents to be used were excluded.
Patients were randomized by Y. Ölmez using the block randomization method. The patients were distributed into two groups. Group 1, consisting of 31 eyes of 31 patients, received topical 0.1% nepafenac with topical anesthesia (0.5% proparacaine HCl, Alcaine; Alcon, TX, USA), and group 2, consisting of 28 eyes of 28 patients, received placebo (sterile saline solution) with topical anesthesia. All injections were performed by the same specialist (T. Ogurel).
Topical 0.1% nepafenac was used half an hour and again 5 min just before the injection in group 1, and placebo was used in group 2. Both topical agents were given in camouflaged bottles with trial-specific tags to hide the identity of the test agent and were placed in a tamper-evident box. One of two nurses who had been accustomed to the technique was administered the agents. Two drops of proparacaine, 0.1% nepafenac, and placebo were applied each time.
One drop of 10% povidone-iodine was supplied to each patient before the IVI. Injections were performed at 4.0 mm site from the limbus for phakic patients and at 3.5 mm site from the limbus for pseudophakic patients in the superotemporal quadrant of each eye. Immediately following the injection, the visual analog scale (VAS) was explained to the patients for pain, and they were tested to categorize their pain from 0 to 10, with 0 = no pain/no distress and 10 = worst possible pain/unbearable distress (Figure 1). Also, the Wong-Baker Faces Pain Rating Scale was evaluated as an observer scale (0 = no hurt, 1–2 = hurts a little bit, 3–4 = hurts a little more, 5–6 = hurts even more, 7–8 = hurts a whole lot, and 9–10 = hurts the worst) (Figure 2). All patients were injected with Ozurdex for the first time. Ofloxacin, a third-generation fluoroquinolone, was prescribed to all patients for 3–5 days as a postinjection antibiotic.

Visual analog scale.

Wong-Baker Faces scores.
All data analyses were performed using a statistical package (version 20.0, IBM), and software was used for the power analyses. The determined effect size was 1.13; considering a type I error (α) of 0.05 and accepting a power of 95%, a minimum sample size was calculated. The power calculation analysis revealed that the minimum required sample size was 19 patients for each group estimation based on the VAS pain score according to the data from a previous study. 19 The Kolmogorov–Smirnov test was used to examine whether the data fit a normal distribution. The independent samples t test and Mann–Whitney U test were used to compare variables. Comparisons of nominal data were evaluated with chi-square test. Spearman’s Rho correlation test was used to check the correlation between quantitative variables. In all analyses, a value of p < 0.05 was considered statistically significant.
Results
There were 14 (45.2%) men and 17 (54.8%) women in group 1 and 16 (57.1%) men and 12 (42.9%) women in group 2. The mean age of the patients was 64.42 ± 5.51 years in group 1 and 62.32 ± 7.54 years in group 2. There was no significant difference between the two groups in terms of sex and age (p = 0.411 and p = 0.284). Table 1 shows the demographic data of groups. The number of subjects with RVO and PCME was 25 and 6, respectively, in group 1 and 20 and 8, respectively, in group 2.
Demographic characteristics and VAS score of two groups.

PCME, pseudophakic cystoid macular edema; RVO, retinal vein occlusion; VAS, Visual Analog Scale.
Independent t test.
Chi-square test.
Mann–Whitney U test.
The median VAS pain score was 2 (1–3) in group 1 and 4 (1–6) in group 2. The VAS pain score was significantly lower in group 1 compared with group 2 (p < 0.001) (Figure 3). The Wong-Baker Faces scores were statistically reduced in group 1 (p < 0.001). Figure 4 shows the number of patients according to their Wong-Baker Faces scores in both groups.
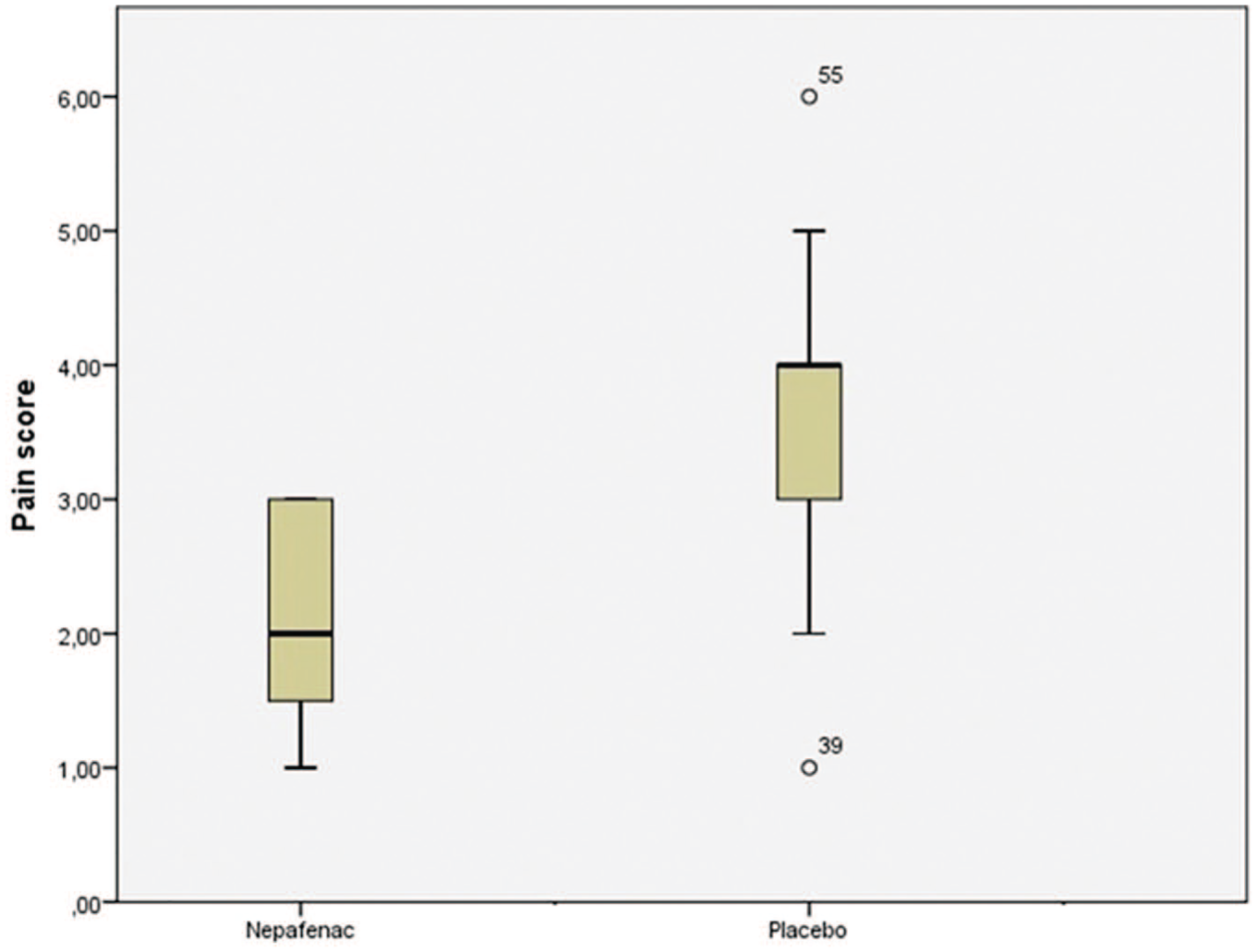
Nonparametric box plots for the distribution of VAS pain scores are shown (horizontal lines are medians and quartiles, and circles indicate outliers and extreme values, respectively, with more than two to three times deviation of the interquartile range from the upper quartile).

The number of patients according to the Wong-Baker Faces scores in both groups.
There was no correlation between VAS pain score and sex, age, or underlying disease (p > 0.05; Table 2)
Correlation with VAS score and age, sex, and ocular disease.

VAS, Visual Analog Scale.
No eyes experienced complications during the injections.
Discussion
This study found that the analgesic effect of 0.1% nepafenac reduces the pain of patients during intravitreal Ozurdex injection.
IVI is an effective procedure to deliver the desired concentration of drugs or pharmacologic agents into the eye. As most of the topical and periocular drugs used in ophthalmology have lower penetrance and, therefore, reduced effectiveness in the back of the eye, they are not as effective as IVIs for targeted treatment. Today, there are several new treatment agents for retinal diseases, especially for diabetic retinopathy and age-related macular degeneration. Moreover, numerous intravitreal pharmacologic agents have become available with continued delivery systems. Many patients may necessitate as frequently as once-a-month injections, possibly for years.
Like other procedures in ophthalmology, IVIs cause pain at the site of injection and raise the concerns of patients. This pain can be associated with age, sex, anxiety, or number of injections.6,20,21 The views on this matter are, however, controversial. While some authors reported that women and older patients perceived more pain, 6 other authors claimed opposite views. 19 This situation causes distress for patients and reduces treatment compliance, especially in patients who need multiple injections to attain and sustain a treatment effect. Therefore, performing the procedure as painlessly as possible will make the patient more comfortable and agreeable.
Ozurdex is an intravitreal implant in an applicator. The applicator is a disposable injection device that contains a rod-shaped implant which is not visible and has a relatively large 22-gauge needle compared with other needles. The implant is approximately 0.46 mm in diameter and 6 mm in length. Therefore, patients may experience more pain than other procedures with a smaller size needle (27.5–32 gauges). 22
Standard application of an IVI is to perform it under topical anesthesia. There are some studies which compared the effectiveness of various anesthetic methods or agents for IVIs.23–25 Still, no anesthesia technique for this procedure has been proven to eliminate pain completely.
Rifkin and Schaal 23 compared the analgesic efficacy of Tetravisc, proparacaine, and tetracaine and reported that patients receiving tetracaine had lower pain score than patients receiving proparacaine or Tetravisc. Blaha and colleagues 24 showed that topical anesthesia is a more effective method for reducing pain related to IVI than lidocaine-applied pledget. In another study, Cintra and colleagues 18 compared three different anesthetic methods for IVI of bevacizumab, including topical, subconjunctival, and peribulbar anesthesia, and found that peribulbar anesthesia was more effective in limiting injection-related pain but was associated with minimum effectiveness in reducing entire procedure pain. Also, there is a study that evaluated anesthetic methods for intravitreal Ozurdex injection. Karabaş and colleagues 25 compared topical proparacaine drops and lidocaine-applied pledget with subconjunctival lidocaine injection and found that there was no difference in pain scores.
Topical NSAIDs have been used in ophthalmology to control postoperative inflammation, prevent PCME, 25 maintain intraoperative mydriasis, 26 and, in the last years, reduce pain after ocular surgery. 27 In this study, 0.1% nepafenac combined with topical anesthesia was used to control injection-related pain.
Modi and colleagues 28 found that nepafenac 0.3% used once-daily was as effective as three times daily nepafenac 0.1% for treatment and prevention of ocular pain and inflammation after cataract surgery in their multicenter study.
In the present study, the VAS pain scores were significantly lower in patients who received 0.1% nepafenac compared with placebo. Also, the Wong-Baker Faces scores were statistically significantly reduced. That means, 0.1% nepafenac has clinically significant analgesic effect during intravitreal Ozurdex injection. We think that these results may enhance patient comfort and improve compliance with treatment because pain is the most important factor affecting the patients’ adherence to treatment. 29 Makri and colleagues 30 reported that a single drop of nepafenac before IVI was effective in reducing IVI-related pain immediately and up to 6 h after the injection. In another study, Georgakopoulos and colleagues 19 compared nepafenac 0.1% and 0.3% with placebo in patients undergoing IVI, and they found that immediately after IVI, the VAS pain scores were statistically significantly lower in patients treated with nepafenac 0.1% and 0.3% compared with placebo. These studies support the findings of the present study because intravitreal Ozurdex injection is one type of IVI.
In the present study, VAS scores were relatively higher than in previous studies.7,31 We think that this is due to the patient group in our study that received Ozurdex injections for the first time.
The limitation of this study is the absence of an objective test to assess the pain sensitivity of patients before injection. Unfortunately, there is currently no test that can assess the pain sensitivity of subjects.
In this study, the analgesic effectiveness and patient satisfaction with 0.1% nepafenac were evaluated with the VAS and Wong-Baker Faces scores. The VAS used in this study has been shown to be a reproducible and dependable method for evaluating a patient’s pain level.32,33 Previous studies have demonstrated the effectiveness of nepafenac in pain reduction after cataract surgery and IVIs. To our knowledge, this is the first study evaluating the analgesic effect of nepafenac on injection-related pain during intravitreal Ozurdex injection. Topical anesthesia is used as a standard anesthetic technique for IVIs, but it may not always provide complete analgesia.
The present study has shown that 0.1% nepafenac combined with topical anesthesia may improve patient comfort and is more effective than topical anesthesia alone in preventing pain during intravitreal Ozurdex injection. This effective method of analgesia could make intravitreal Ozurdex injections more tolerable. Application of a single drop of 0.1% nepafenac before an Ozurdex injection appears to lessen injection-related pain. This low-cost application may also solve treatment compliance problems that may be caused by pain in some patients.