
Abstract
Purpose:
To report outcome of trabeculectomy performed by single scleral suture in Indian eyes.
Methods:
Non-randomized, non-masked, retrospective cohort analysis. Medical records of all consecutive patients who underwent trabeculectomy between 1 January 2011 and 31 December 2016 at CL Gupta Eye Institute, Moradabad (India), were reviewed and analyzed. Trabeculectomy was performed using single scleral suture for flap closure. The suture knot was buried inside sclera. The laser lysis of scleral suture was not done. Success was defined as complete success if an intraocular pressure (IOP) was >5 and ⩽21 mmHg without any glaucoma medications or re-surgery. Qualified success was defined as IOP ⩽21 mmHg with or without antiglaucoma medications.
Results:
Data of 98 patients was analyzed. A total of 61 (62.2%) of them underwent trabeculectomy, and 37 (37.7%) underwent phacotrabeculectomy. The probability of complete success in patient underwent phacotrabeculectomy was 86% at 3 years, and in-patient underwent only trabeculectomy was 95% at 3 years. The probability of qualified success in patient undergone phacotrabeculectomy was 91% at 3 years, and in patient undergone only trabeculectomy was 97% at 3 years.
Conclusion:
The mean postoperative IOP was significantly less then mean preoperative IOP, at all follow-up visits. This simplified technique also resulted in high midterm success probabilities with low complication rates.
Introduction
It has estimated that India has about 20% of the world glaucoma population by 2020.1,2 Trabeculectomy has been considered as gold standard for medically uncontrolled glaucoma. It is a guarded partial-thickness filtering procedure performed by the removal of a block of peripheral corneal tissue beneath a scleral flap. It improves aqueous outflow in glaucomatous eyes. The long-term successful control of intraocular pressure (IOP) has been ranged from 48% to 98%.3–10 In comparison to other treatment modalities, studies have reported that optimal IOP lowering and better diurnal control can be achieved by surgical intervention.11–18 Suture adjustment and bleb interventions are frequently necessary after trabeculectomy.3,19,20 Several modifications of trabeculectomy have been described, suggesting variation in shapes and sizes of the scleral flap, use of antimetabolites, and use of laserable, releasable, or adjustable sutures.20–24 Releasable sutures placed at the time of surgery and their sequential release in the postoperative period is a useful technique. A variety of suturing techniques have been described.25–27 Laser suture lysis has become a common practice in the postoperative management of trabeculectomy. 28 Both techniques can be associated with complications such as flat anterior chamber and wound leaks. 29 However, the outcome of trabeculectomy performed by single scleral suture without its laser lysis has not been reported yet. The aim of this study was to report the reduction in IOP after trabeculectomy performed using single scleral suture in Indian eyes.
Methods
This study included consecutive patients with medically uncontrolled glaucoma who underwent trabeculectomy or phacotrabeculectomy (Phaco + Trab) between January 2011 and December 2016 at CL Gupta Eye Institute, Moradabad (India). Retrospective review of the medical records was performed. This study was approved by the Institutional Review Board (Approval Number: IRB/18/08) and adhered to the tenets of Declaration of Helsinki. Individual consent from patients was waived, as it was a retrospective study. The study subjects included individuals ⩾18 years of age with medically uncontrolled primary open-angle glaucoma (POAG) or primary angle-closure glaucoma (PACG) with no previous intraocular surgery. The exclusion criteria were secondary etiology such as traumatic, neovascular, exfoliative, pigmentary, congenital, and uveitic glaucoma. Re-trabeculectomy surgery done during study period was not included in the analysis.
The IOP was measured using Goldmann Applanation Tonometer, and gonioscopy was performed using a Sussmann’s four mirror gonioscope under appropriate testing conditions. Glaucomatous optic disk changes were focal or diffuse neuroretinal rim thinning, localized notching, or nerve fiber layer defects. Visual field defects has been considered glaucomatous if at least two of the three Anderson’s criteria (three or more non-edged points in a cluster depressed to p < 5% and one of which is depressed to p < 1%, Glaucoma Hemifield Test outside normal limits and Pattern Standard Deviation depressed to p < 5%) were fulfilled.
Age, gender, type of glaucoma, presence of systemic diseases (diabetes mellitus and systemic hypertension in particular), presenting IOP, highest recorded IOP, number of antiglaucoma medications, and visual field parameters were recorded. All the surgeries were performed by single glaucoma surgeon.
Surgical technique
Under peribulbar anesthesia (bupivacaine 0.5% + xylocaine 2%), a superior rectus bridle suture was used for better exposure for fornix-based flap. The trabeculectomy has been positioned at 12 o’clock. A fornix-based conjunctiva was dissected along the limbus 5 mm in length (Figure 1(a)). A 3- to 4-mm length triangular half-thickness scleral flap was created (Figure 1(b)). Paracentesis site was made at 9 o’clock with ophthalmic microsurgical knife 20 gauge microvitreoretinal (MVR) blade. The sclerostomy was created as a cut block with the use of aophthalmic microsurgical knife 20 gauge MVR blade (Figure 1(c)). An iridectomy was performed to reduce the risk of iris occluding the sclerostomy, especially in phakic eyes, and to prevent pupillary block. Only one single 10-0 nylon suture was used to close scleral flap, and conjunctiva was secured with four 8-0 Vicryl sutures (Figure 1(d)).
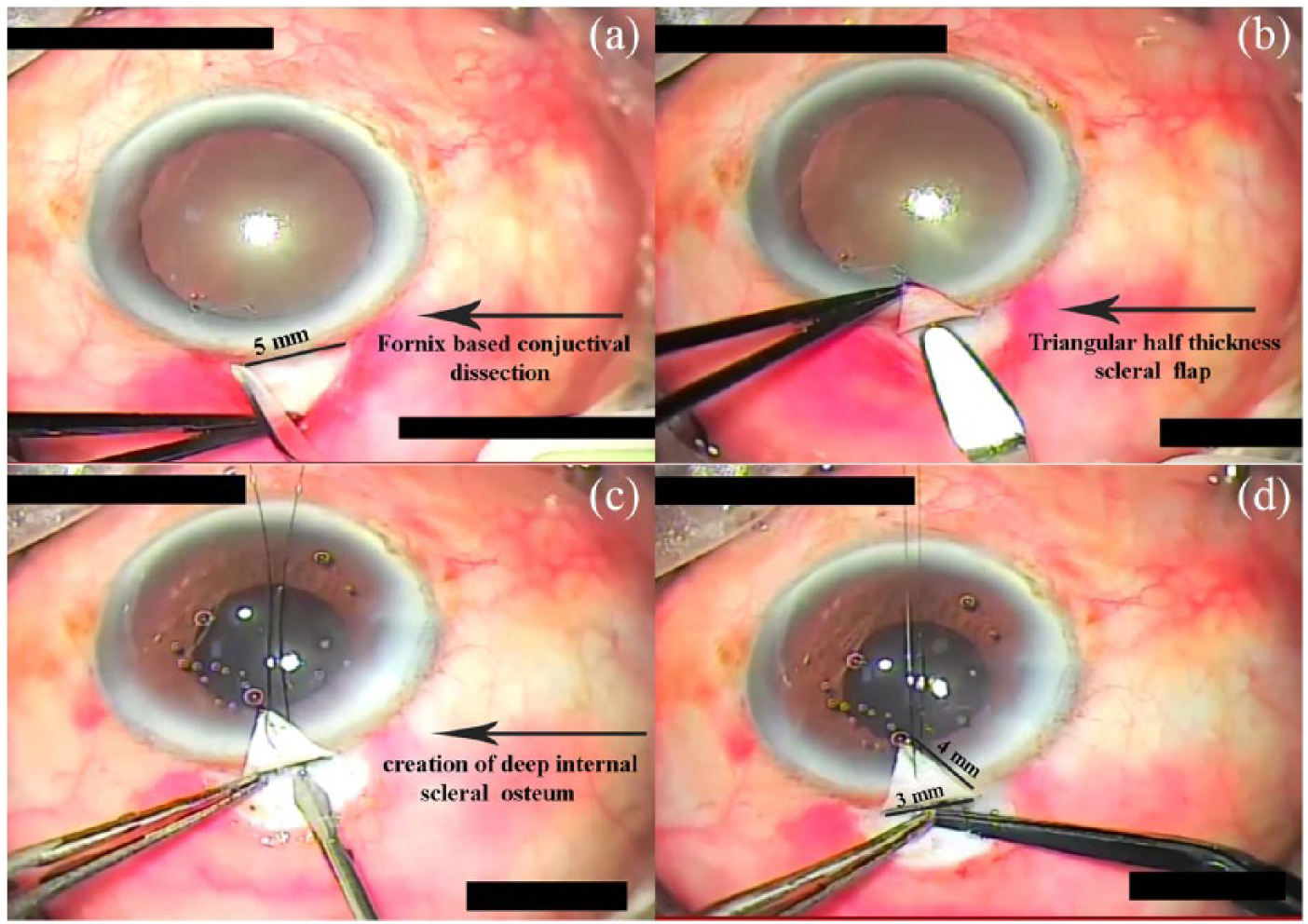
Single suture technique. a) Fornix based conjuctival dissection; b) Creation of triangular half thickness scleral flap; c) Creation of deep internal scleral osteum; d) Single suture closure of scleral flap and conjunctiva.
The patients were followed up at 1 day, 1 week, 1, 3, 6, 12, 18, 24, and 36 months. Postoperatively, all patients received topical steroid (prednisolone acetate 1%) in tapering dose for 6 weeks, and topical antibiotic (moxifloxacin 0.5%) for 6 weeks. Antiglaucoma medications were prescribed if progression was noticed on Humphrey Visual Field (HVF) perimetry during follow-up visits. Bleb in early, intermediate and late follow-up period with this technique was shown in Figure 2.

a) Preoperative photograph; b) Immediate postoperative photograph; c) Intermediate postoperative photograph; d) Late postoperative photograph.
Statistical analysis
Statistical analysis was performed using SPSS software. Significance was defined as p < 0.05. Demographics and baseline characteristics were summarized using descriptive statistics. Categorical variable were summarized using frequencies and percentages. Kaplan–Meier survival analysis was performed for the time to complete and qualified and failed success rates. Success was defined as complete success if an IOP was >5 and ⩽21 mmHg without any glaucoma medications or re-surgery. Qualified success was defined as IOP ⩽ 21 mmHg with or without antiglaucoma medications. A binary logistic regression was performed to ascertain the effects of age, gender, type of surgery (Phaco/Phaco + Trab), and systemic disease present or not, family history of glaucoma, central corneal thickness, preoperative IOP on the likelihood that patient had qualified surgical outcome. All the variables were used as covariates in a binary logistic regression model with forced inclusion. The primary outcome measure was success and failure of surgery based on predefined criteria. A Hosmer–Lemeshow test was used to test the goodness of fit of the model.
Results
Medical records of 98 eyes of 98 patients who underwent trabeculectomy or phacotrabeculectomy procedure during the study period were reviewed. Re-trabeculectomy surgery was performed in 20 eyes during this period. Data of these patients were not included in the analysis. A total of 56 (57.1%) of them were men. Mean age of patients was 53.5 ± 13.2 years. Table 1 presents baseline clinical features of enrolled patients. Preoperative baseline mean IOP was 31.5 ± 6.02 mmHg. The mean postoperative IOP at day 1 was 16.6 ± 6.2 mmHg [p = 0.001; 95% confidence interval (CI): 13.153–16.647], at week 1; 15.4 ± 6.8 mmHg (p = 0.001; 95% CI: 14.267–17.933), at 1 month; 16.9 ± 7.2 mmHg (p = 0.001; 95% CI: 12.707–16.493), at 6 month; 15.8 ± 5.22 mmHg (p = 0.001; 95% CI: 14.0853–17.3147), at 2 years 16.1 ± 3.1 mmHg (p = 0.001; 95% CI: 14.019–16.781), and at 3 years 18.1 ± 2.5 mmHg (p = 0.001; 95% CI: 12.068–14.732; Figure 3). The mean IOP was significantly lower than mean preoperative IOP (31.5 ± 6.2 mmHg) at every follow-up visit.
Baseline characteristics.

POAG: primary open-angle glaucoma; PACG: primary angle-closure glaucoma; CCT: central corneal thickness.
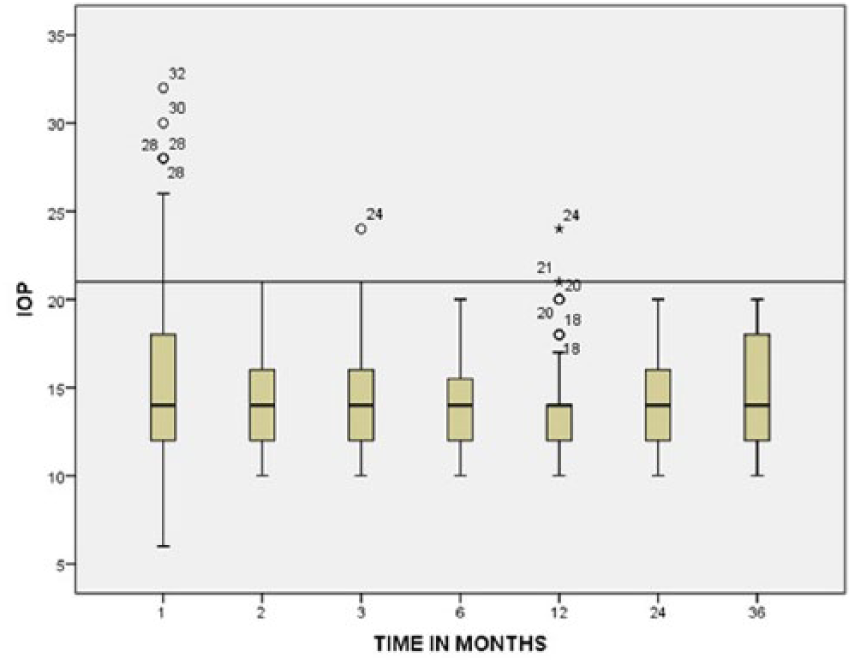
Box plot showing distribution of IOP at different follow-up visits.
The probability of complete success in patient underwent phacotrabeculectomy was 86% at 3 years, and in patient underwent only trabeculectomy was 95% at 3 years. The probability of qualified success in patient undergone phacotrabeculectomy was 91% at 3 years, and in patient undergone only trabeculectomy was 97% at 3 years. (Figures 4 and 5)
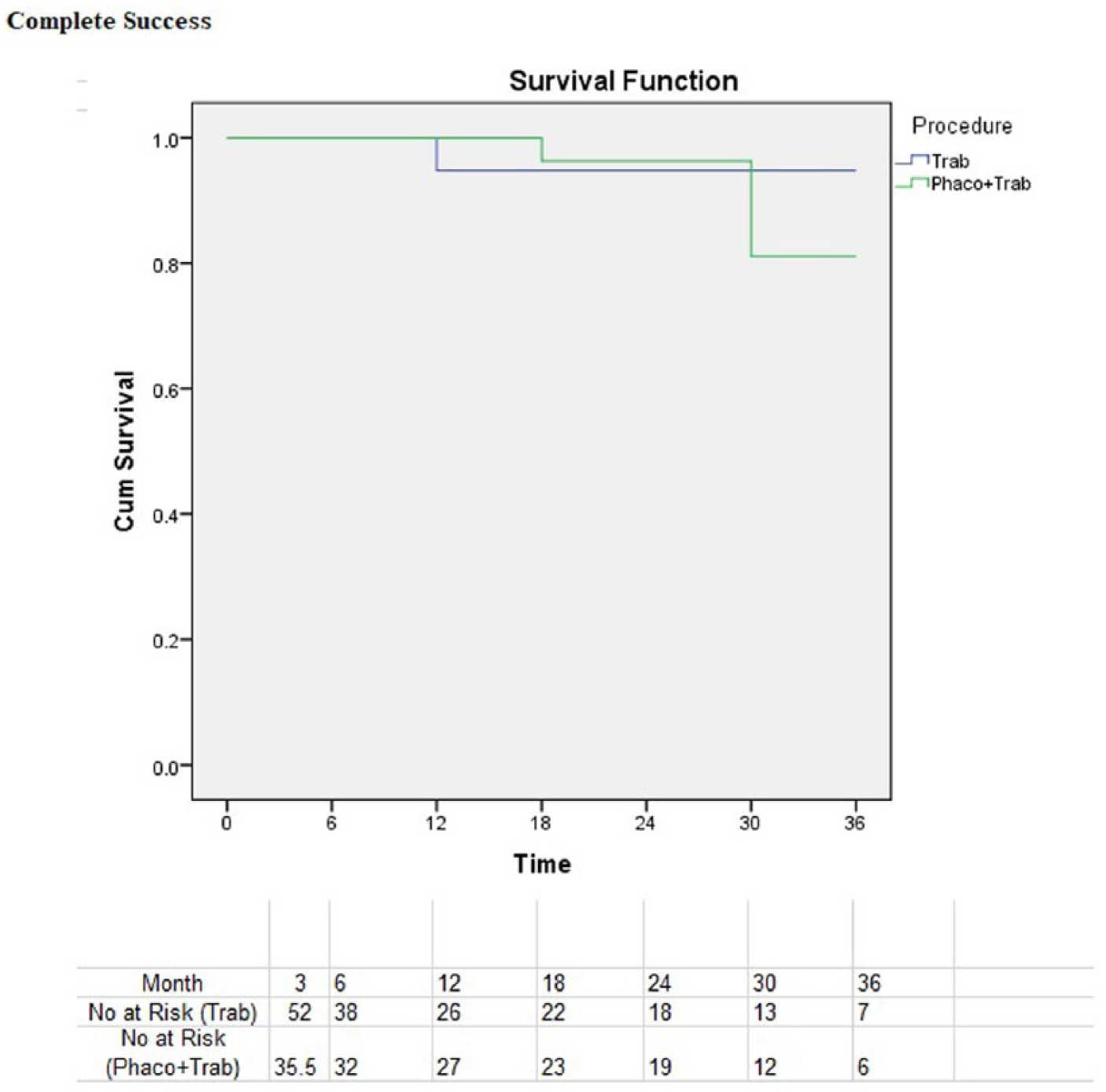
Kaplan–Meier survival plot showing probabilities of complete success.

Kaplan–Meier survival plot showing probabilities of qualified success.
Postoperative complications were bleb leak in two patients, shallow anterior chamber in one patient, and hypotony in three patients. Binary logistic regression analysis showed that there is no effect of any variable on success of surgery once other covariates were taken into consideration. Results of the binary logistic regression model evaluating the associations between failure and the baseline characteristics are shown in Table 2. A Hosmer–Lemeshow goodness of fit test showed that the binary model was a good fit to the data (p = 0.13). The model explained 13.8% (Nagelkerke R2) of the variance in success of surgery and correctly classified 94.9% of cases.
Results of binary logistic regression model.

CCT: Central corneal thickness; IOP: Intra ocular pressure.
Discussion
The mean postoperative IOP was significantly less then mean preoperative IOP at all postoperative follow-up visits. There was 42.1% reduction in mean preoperative IOP till 3 years. In this study, the probability of complete success was 87% at 3 years and of qualified success was 94% at 3 years. The success probability in patients who underwent trabeculectomy was higher than in patient who underwent phacotrabeculectomy. This was because of more postoperative inflammation in phacotrabeculectomy group. The success rates at 3 years in this study are similar to the success rates reported in previous studies.3,4 The success rate of trabeculectomy in experienced hands is estimated between 60% and 100%. 30
Although new modalities like drainage devices have been developed for glaucoma treatment, still trabeculectomy procedure is the preferred choice for surgical management of glaucoma. There are several factors associated with this. The availability of newer treatment modalities is not uniform. Affordability and treatment compliance of patients are also among different factor.
Sutures provide resistance to flow across the flap in the early postoperative period prior to wound healing. Sutures are important because the healing is delayed with antimetabolites, although no antimetabolites were used in this study perioperatively or postoperatively. 31 Suture adjustment and bleb interventions are often required after trabeculectomy.3,30 Different types of sutures technique has been used for flap closure in trabeculectomy. It includes single sutures cut with laser lysis, 32 sutures released by corneal incision,24,27 or sutures that can be transconjunctivally adjusted.30,33,34
In this study, we used a single suture for flap closure in all patients. The midterm probability of success and percentage reduction in IOP is comparable with other studies.33,34 Aykan et al. reported 92% success after laser suture lysis of single sutures. 23 This study also reported 94% success probability after trabeculectomy using simplified single scleral suture technique without suture lysis. The single suture knot was buried inside sclera so that it will not have any suture knot–related conjunctival perforation or foreign body sensation. Bleb leak was noticed in two patients at 1 week follow-up. This was managed medically with the help of large size bandage soft contact lens and topical use of Gentamycin eye drop for 3 weeks. Hypotony noticed at day 1 were also managed medically with recovery within a week without any complication in two patients. However, in one patient hypotonus maculopathy was developed. This was managed medically with topical and oral steroid and patient recovered within a week’s time.
This simplified technique is beneficial for ophthalmologist working with limited recourse setting in peripheral ophthalmology centers. There are advantages and disadvantages of all surgical techniques. The advantage of putting one suture is that surgeon does not require a setup of laser suture lysis. Patient does not require additional follow-up. Shorter surgical time is also one of the advantages of this technique. There are certain limitations of this study. Only 21% in the trabeculectomy group and 32% in the phacotrabeculectomy completed the 3 years follow-up. The success probabilities of trabeculectomy performed by single scleral suture were not compared to the control group with double, triple, or releasable suture.
Conclusion
The complications after putting single suture are comparable with other technique of scleral flap closure. The results of this study suggest that this surgical technique is effective in adequate reduction of IOP, with low comparable complication rates with other techniques.