
Abstract
Purpose:
To describe visual and vestibular functioning and the effects of age and surgery effects on postural control in healthy children with vertical strabismus.
Design:
This is a comparative case series.
Methods:
We evaluated participants at the Scientific Institute Eugenio Medea during routine clinical activities. We enrolled 30 consecutive children/adolescents (age range 4–13 years) with isolated vertical strabismus, with and without corrective surgery. Participants were split into four subgroups according to age (4–8 years versus 9–13 years) and ocular surgery (surgery versus no surgery). The clinical protocol included ophthalmological, orthoptic, neurological, physiatrical, otolaryngological, and vestibular evaluations, and the instrumental protocol included ocular cyclotorsions assessment, posturography, and vestibular myogenic-evoked potentials. Main outcome measures of the study were the prevalence of study-relevant orthopedic, ocular, vestibular, and posturographic abnormalities.
Results:
Among the overall largely variable findings across patients’ groups, we found some interesting trends: larger binocular vision and convergence disorders in younger children, smaller prevalence of asymmetric vestibular-evoked potentials in operated children, less posturographic abnormalities in younger children. No clear-cut beneficial effect of surgery was found on all clinical and instrumental parameters considered, despite good re-alignment of the eyes.
Conclusion:
The pathophysiology of postural control in vertical strabismus is extremely complex and above the potential of this study design and should be specifically addressed in deeper experimental studies.
Introduction
Postural control relies on proprioceptive, visual, vestibular, and somatosensory inputs. Furthermore, postural control changes according to age. 1 In fact, from infancy to adulthood and, eventually, to old age, all these sensory systems – and all the motor systems that are activated to gain postural control – change according to different developmental trajectories or to different degenerative processes. This has direct effects on how individuals maintain the vertical position of the head and of the body during both quite stance and movement, and on how they activate compensatory postures/movements to preserve stability. Many clinical conditions can determine impairments of postural control development in early life – if congenital or early acquired – or they can determine its loss if they emerge after the infancy period. In general, when one sensory system input is not working well, the other subsystems compensate for the impairment by playing a greater role. 2
From the early childhood to adolescence, subjects maintain their postural control by relying principally on visual information, contrary to what holds good for adults 3 who tend to maintain their postural control on a multisensorial basis. Therefore, it is of notable interest to investigate postural control in children suffering from any type of visual sensory disorder.
Strabismus in children is quite frequent (2–4% of the general population). It can determine postural control disorders affecting binocular vision and proprioceptive information coming from extra-ocular muscles. However, few studies have so far addressed the effects of strabismus on postural control deficits. Kapoula and Lee 4 showed that improving convergence efficiency determined direct benefits on postural control. Legrand and colleagues reported improving effects of ocular surgery on postural control 2 months after surgery 5 and following re-alignment of the eyes with prisms and with eye surgery, 6 demonstrating that improving binocular vision determines significant postural control gain. Gaertner and colleagues 7 confirmed benefits of binocular vision on postural control in strabismic children. To the best of our knowledge, even if visual–vestibular interactions mature very early in infancy, no previous studies have investigated visual and vestibular functioning in children with strabismus. Only Bucci and colleagues 8 described poor postural stability in children with vertigo and convergence abnormalities.
Thus, in this pilot clinical–epidemiological study, we address postural control in young and older children with one type of ocular strabismus (specifically, vertical strabismus), relative to visual and vestibular functioning and to corrective ocular surgery. Vertical strabismus is quite infrequent (2%), while esotropic and exotropic deviations are much more frequent (45% and 53%, respectively). 9 We decided to focus on vertical strabismus in that, among all types of strabismus, it is frequently responsible for head tilt (also named ocular torticollis) 10 that, per se, can determine anomalous vestibular functioning affecting head verticality. Head tilt represents compensative posture to maintain binocular vision and the best visual acuity. In addition, ocular torticollis is frequently associated with positional (deformational) plagiocephaly 11 that can result in anatomic, and potentially functional, asymmetries of the vestibular system. 12
Our study hypothesis was that, in agreement with previous studies, which demonstrated postural control gain following surgical correction of exo- and esotropic strabismus,5,6 surgical correction of vertical strabismus should determine postural control recovery and this should be larger in younger children known to rely their postural control more on visual information than on multisensorial (somatosensory, vestibular, proprioceptive) bases. 3 Therefore, we expected younger operated children to show better posturographic parameters than not operated ones.
Methods
We enrolled 2000 consecutive children/adolescents (0–18 years old) presenting with manifest or latent (evident on Cover test) strabismus attending the ophthalmologic clinic of our institute over a 6-month period for ophthalmologic and orthoptic evaluations. All participants’ parents signed written informed consent. The investigation adhered to the principles of the Declaration of Helsinki on human research and the ethical committee of our research institute approved the research protocol (project ID: 83, approval 11 March 2014). We excluded all subjects affected by developmental congenital or developmental acquired neurological and psychiatric disorders, and subjects with auditory – hearing loss – or visual – mild to severe blindness – disorders, or with, developmental genetic syndromes, in general.
Among the 196/2000 subjects that we first identified with vertical strabismus, we selected 30 of them (overall best corrected visual acuity 9–10/10, 24/30 patients wore glasses to gain normal visual acuity, 15/30 presented with alternate vertical deviations). These 30 subjects presented the following characteristics: age ranging from 4 to 13 years (corresponding to the age limits of our normative data set of posturographic evaluations), presence of manifest vertical strabismus (mean vertical deviation equal to 10 prismatic diopters, see Table 1) (we excluded those with a latent strabismus), presence of ocular torticollis. In addition, we considered absence of secondary forms of vertical strabismus [i.e. all subjects had primary strabismus free of neurologically functional and anatomic pathologies, as ascertained by means of magnetic resonance imaging (MRI) scanning]. This group of 30 subjects underwent all clinical evaluations: full ophthalmological, orthoptic, neurological, physiatrical, otolaryngological, and vestibular clinical evaluations, scanning laser ophthalmoscopy to measure ocular cyclotorsions, posturography to investigate stance control, and vestibular myogenic-evoked potentials to address asymmetries of vestibular function.
Clinical and instrumental findings.

We split the whole group into four subgroups according to age and ocular surgery (for strabismus): 4- to 8-year-old young children without ocular surgery, 9- to 13-year-old older children without ocular surgery, 4- to 8-year-old young children who underwent ocular surgery for strabismus, and 9- to 13-year-old older children who underwent ocular surgery. The four subgroups included, respectively, 11, 6, 8, and 5 individuals (Table 1). Ocular surgeries consisted of inferior oblique or superior rectus recession. Around 25% of surgeries (3/13) were bilateral.
No sample power calculation was performed as the initial group of 30 patients was too small to do it. This represents a known limitation of this pilot study.
We ran all clinical and instrumental evaluations at least 1 year following surgical interventions in the last two subgroups. We measured fovea positions by means of Maia Microperimeter Scanning Laser Ophthalmoscope. We first took reference of the horizontal axis and of the subject’s head using a clinometer fixed to the subject’s head. Then, we superimposed this reference to ocular fundus pictures in order to evaluate the presence/absence of ocular cyclotorsions.
Participants underwent a full functional motor and muscular–skeletal examination. We performed posturographic evaluation running three consecutive registering trials in four conditions. The first was standing on the footboard with eye open (NO – normal open, the ecologic stance condition). The second was standing on the footboard with eyes closed (NC – normal closed, the stance condition where postural control relies more on proprioceptive somatosensory input). The third was standing on pads with eyes open (PO – pad open, the stance condition where postural control relies more on visual information). The fourth was standing on pad with eyes closed (PC – pads closed – the stance condition where postural control relies more on vestibular afferent information). We used a footboard with piezoelectric crystals (Kristler 9286AA model). We applied a low-bandpass filter set at 10 Hz. Participants were standing still looking at a 3-m far fixating point. To quantify the postural performance from data obtained from the platform, we analyzed the surface (data not reported) and the variance of speed of the center of pressure (CoP). In a previous work, 13 we had collected normative values for 4–13 years old children/adolescents.
Participants underwent also vestibular-evoked myogenic potentials (VEMPs), registering cervical responses. We registered cervical-evoked potentials (c-VEMPs) from the active electrode placed on the body of the sternocleidomastoid muscle, with reference places at the top of the sternum. We administered 50-ms long square tones of 100 dB amplitude at 0.5-Hz stimulation frequency. Filter bandpass lower and upper limits were 20 Hz and 20 kHz, respectively.
Results
All clinical and instrumental findings are reported in Table 1 in detail. Here, we will briefly report some of them that deserve deeper attention and that will be discussed further in the following section.
Vertical strabismus prevalence
In our population, the prevalence of subtypes of strabismus was 890/2000 (44.5%) patients with esotropic deviation, 914/2000 (45.7%) patients with exotropic deviation, and 196/2000 (9.8%) patients with vertical deviation.
Plagiocephaly
No differences between groups was present (
Percentage of scoliotic deviations or true scoliosis
Prevalence of scoliotic deviations or true scoliosis was comparable across groups (
Ophthalmoscopic evaluations
Prevalence of Bielschowsky sign range between one third and two thirds of patients, across groups. Even if no statistical difference between groups was present (
Asymmetries on VEMPs
No statistical difference between prevalence of asymmetric VEMPs was found across groups (
Posturography
No statistical difference between prevalence of abnormal posturographic evaluations was found across groups when NO (
Discussion
Here, we will discuss the main findings reported in the previous section. For details, see Table 1.
Vertical strabismus prevalence
The high percentage of vertical strabismus among all strabismus subtypes considerably differed from those reported in the literature (e.g. 2% of vertical strabismus among all strabismus subtypes 9 and 0.26% among the general population 14 ). Our findings are likely to be due to a selection bias. Subjects attending our ophthalmologic clinic presented far more complex ophthalmologic history than normal (general) population as our clinic is a regional third-level center for pediatric neuro-ophthalmology. In fact, all patients came to our clinic following their general pediatric practitioners’ consultation request as suspecting complex clinical picture.
Plagiocephaly
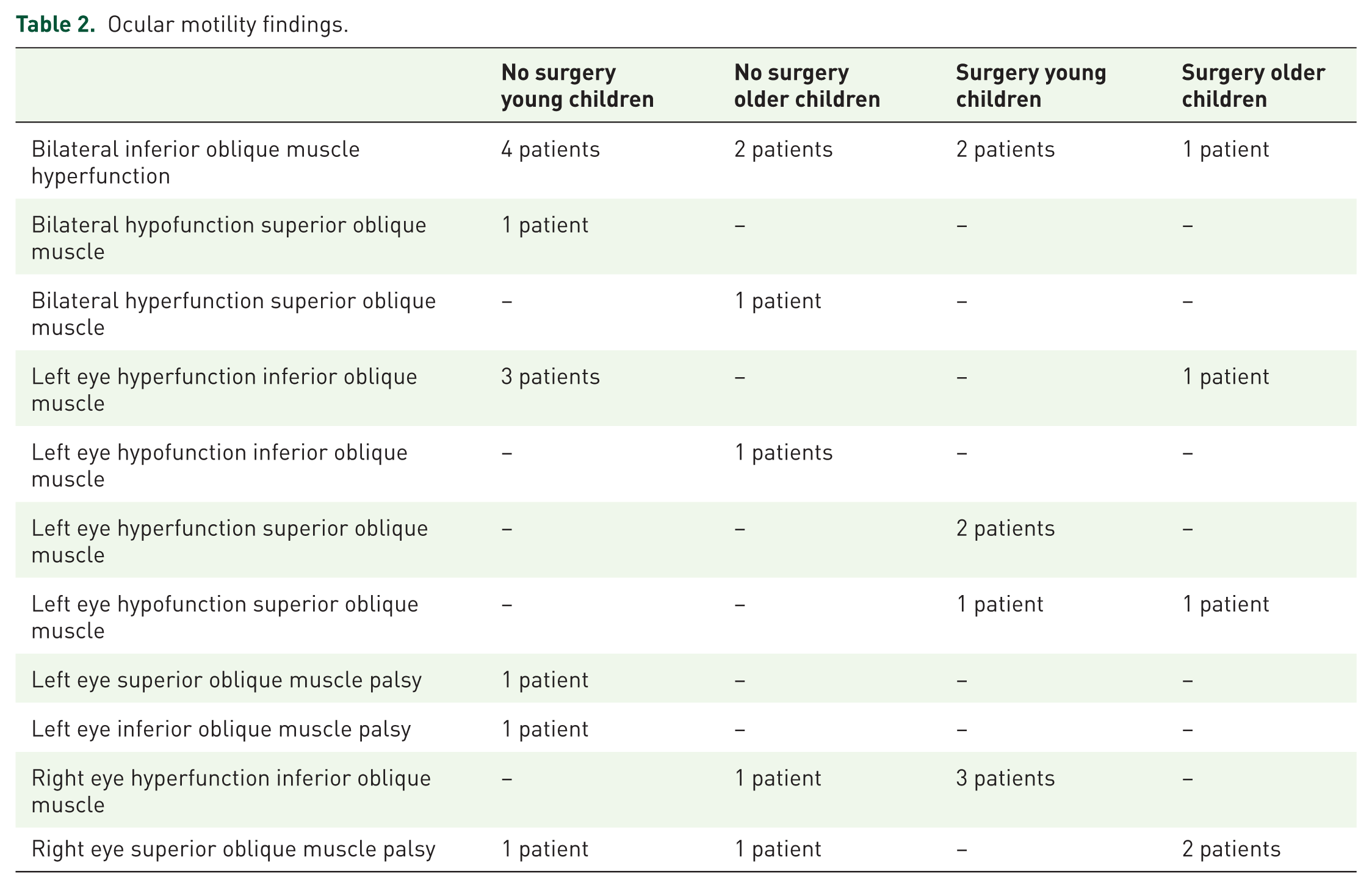
The low prevalence found in our patients (around one third of patients) differs from those reported in literature 11 and it is most likely to depend on different subtypes of vertical strabismus of ocular origin in our group of patients. They presented very variable ocular motor dysfunctions (see Table 2). Usually, most of abnormal head postures, especially head tilts, are due to vertical or oblique muscle dysfunctions and, among them, superior oblique palsy – causing secondary inferior oblique overaction – is more common. 14 Surgery usually can return the head in its nearly correct position, thus regaining best visual acuity (with variable levels of stereopsis recovery).
Ocular motility findings.
Scoliosis or scoliotic deviations of the axis
Overall, all patients’ groups presented this clinical sign in agreement with previous research. 12 This is unsurprising as, irrespective of the ocular subtypes of vertical strabismus (see Table 2), a misalignment of the eyes, with compensatory head tilt, easily determines some vertebral axis abnormality. A trend toward larger prevalence of scoliotic deviations/true scoliosis was present in patients who underwent ocular surgery. This likely depends on the longer clinical history before surgical correction (mean years: 3.4, range; 2–5 years, following the emergence of ocular strabismus), or of the earlier emergence of vertical strabismus (in very early infancy). Thus, unsurprisingly, ocular surgery did not represent a protective intervention to prevent/correct scoliotic deviations or true scoliosis.
Ophthalmoscopic evaluations
We found large variability across the four groups of patients on the Bielschowsky head tilt test, in agreement with large variability of ocular motor findings (see Table 2), with a trend toward smaller prevalence in young not operated children. This likely depends on the young patients’ age that might have determined more efficient intra-ocular motor compensatory mechanisms. Despite good re-alignment of the eyes obtained in all patients, in line with previous studies, 5 surgery had no influence on all ophthalmoscopic parameters (stereopsis, convergence, subjective visual vertical, and ocular cyclic torsions). However, a trend toward higher prevalence of binocular vision disorders and convergence disorders was present in younger versus older children (11/17 versus 3/11, and 11/17 versus 3/11, respectively). This likely depends on maturational processes of the ocular system. This might suggest that age plus surgery could play possible recovering role for these visual parameters. Worthy of mentioning, we found that 33–50% of patients in each subgroup presented ocular cyclic torsions. All ocular cyclic torsions were exocyclic torsions. Half of them (6/12) had the left eye involved and 3/12 had the right eye involved. Previous studies already reported larger involvement of the left eye (22/30 patients versus 8/30 patients presenting ocular cyclic torsion of the right eye, in Rousié and colleagues’ 12 cohort) in line with the cranial–facial asymmetries found. However, we found bilateral cyclic torsion in 3/12 patients. This was likely due to the variability of ocular motility abnormalities found in our group of patients (see Table 2) suggesting a complex pathophysiology underlying the ophthalmoscopic evaluations. Finally, we found two cases of clear-cut ocular tilt reaction (exocyclic torsion of the hypotropic eye). 15 Finally, the majority of patients (60–73%) presented abnormal subjective visual vertical. Children (contrary to adults) are known to be imprecise in reporting their perception of true vertical reference. 16 Thus, our children with vertical strabismus (up to 13 years of age) were likely too young to show the more efficient compensatory mechanism present in adults.
Asymmetries on VEMPs
No differences across groups were found in terms of prevalence of asymmetric VEMPs. However, a trend toward protective effect of surgery was found, especially in younger children. This disagrees with evidence found concerning ophthalmologic findings (re-alignment of the eyes but no clear-cut effect of surgery on stereopsis, convergence, and cyclic torsions of the eye) and subjective visual vertical. To understand better the effects of ocular surgery on vestibular functioning, larger groups of patients should be studied, especially considering the time postsurgery and age variables.
Posturography
No statistical difference across groups was found. However, a trend toward an age effect was found: younger children tended to present with smaller percentages of posturographic abnormalities with respect to older ones. In addition, younger children largely failed to modify their posturographic performance across registering paradigms (see NC/NO, PO/NO, and PC/NO data in Table 1). On the contrary, older children showed some possible condition-dependent effects: older no-surgery patients tended to improve stability when relying more on somatosensory and vestibular information, and older surgical patients tended to improve stability when vestibular information was the critical one (PC condition). Surgical re-alignment of the eyes had no effects on postural stability in PO condition where visual information is relevant to maintain postural stability (see Table 1). There is wide consensus in claiming that postural stability efficiency increases with age. This holds for healthy children when compared with healthy adults 16 and across different age groups during the developmental period. 13 On the contrary, Nolan and colleagues 17 showed no significant difference, in healthy participants, across childhood (from 9 to 16 years of age) but across sexes, thus, suggesting that the developmental physiology of postural control is somehow more complex than it is usually claimed. We found that younger children felt below age-related normal means of posturographic evaluations probably less than older ones, contrary to what we might have expected. We cannot put forward a clear-cut interpretation of these surprising findings due to the small dimensions of our groups and to the observational design of the study. However, it is likely that they mostly depended on the different effects played by vertical strabismus at different ages. Younger children with vertical strabismus might easily find better postural stability relying on all sensorial input information, contrary to what usually happens in typical development, 3 being congenital their vertical strabismus. On the contrary, older children tended to use more somatosensory and vestibular information (see findings in NC and PC conditions) to maintain balance control in agreement with findings coming from previous studies. 5 However, this might be enough ineffective to compensate for perturbations determined by ocular (visual and proprioceptive oculo-motor) information. We also found that surgical re-alignment of the eyes had no effect on postural control recovery. These findings disagree with previous ones.5,6 However, these authors considered effect of surgery of convergent or divergent strabismus only. No previous studies addressed surgery effects on balance control in vertical strabismus.
The present paper presents several limitations
The first concerns the study design. This research was clinical–observational and only aimed at describing the complexity and the variability of clinical presentations in congenital vertical strabismus conditions. No clear-cut interpretation of our findings can be put forward as they must rely more on experimentally controlled paradigms. We can only suggest that such investigations are mandatory as the pathophysiology of vertical strabismus is extremely complex.10,15,18 In fact, we suggest the opportunity of multidimensional (ophthalmologic, orthoptic, physiatrical, otolaryngological, vestibological, and neurological) evaluations. The second concerns the overall amount of participants included. Even if the patients were neurologically homogeneous (all subjects displayed normal neurological examination and a neuropsychiatric history within normal limits), they constituted quite a restricted group. When splitting participants on the bases of age and ocular surgery, subgroups included quite few children or adolescents. The third limitation concerns the different oculo-motor disorders underlying the clinical diagnosis of vertical strabismus. Since ocular motility and vertical strabismus are pathophysiologically interconnected, future studies on larger populations should address this point specifically.
Summary
The pathophysiological underpinnings of vertical strabismus in neurologically healthy children and adolescents seem to be very complex, with visual and vestibular effects, on one side, and age effects, on the other. Surgical correction of vertical strabismus adds further variables. To better understand the roles played by all these factors, further research with larger groups is needed.
The interested readers of this article should be aware that all protocols and registering data are available at our institute.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.