
Abstract
Objective
To evaluate the clinical effects and safety of omega-3 fatty acid dietary and supplemental interventions for the prevention of migraine in adults, considering subgroups according to dosing and migraine subtypes.
Background
Migraine is a highly prevalent and disabling neurological disorder worldwide, with multifactorial pathophysiology and limited understanding of its underlying biological mechanisms. Given the role of diet in migraine modulation and the involvement of omega-3 fatty acids in pain-related inflammatory pathways, their therapeutic potential as migraine prophylactic remains to be clarified.
Methods
A systematic search in Cochrane Central-Ovid, Scopus, Embase, and Web of Science (November 2025) identified randomized controlled trials (RCTs) on omega-3 or omega-6 supplementation in adults with migraine. The primary outcomes included monthly headache days, daily headache hours, pain intensity, headache impact (HIT-6 and MIDAS), and adverse events. A random-effects model estimated the mean differences (MD) with 95% confidence intervals (CI), and the certainty of evidence was assessed using GRADE.
Results
Ten RCTs on omega-3 interventions were found, with two evaluating omega-3-rich diets and others using doses of 1–6 g/day. No studies assessed omega-6. Overall, omega-3 interventions reduced daily headache hours (MD:1.74, 95% CI: −2.29 to −1.19 and monthly headache days (MD:-2.39 days; 95% CI: −3.78 to −1.00) but did not reduce pain intensity. It improved MIDAS (MD: −12.88, 95% CI: −18.36 to −7.40) and HIT-6 (MD:-2.94; 95% CI: −4.32 to −1.56). Digestive adverse effects were reported with 6 g/day. The certainty of evidence was low or very low due to bias, imprecision, and inconsistency. The omega-3 diet improved the chronic migraine frequency but not the quality of life. Capsules (1 to 1.5 g/day) had no effect, while 2 g/day slightly improved headaches and HIT-6. However, in episodic migraine, 1 to 2.5 gr./day improved the frequency and quality of life, but 6 gr./day had no effect.
Conclusion
Omega-3 interventions, particularly structured high-omega-3, low-omega-6 dietary programs and moderate-dose supplementation, may modestly reduce migraine frequency and disability, with the greatest benefit observed in episodic migraine. Further large, high-quality RCTs are warranted to confirm these findings and clarify the optimal dosing strategies.
This is a visual representation of the abstract.
Introduction
Migraine, recognized as one of the main causes of disability worldwide, has seen an increase in its prevalence in recent decades, impacting a considerable number of people.1,2 Migraine has a global prevalence estimated at roughly 14.4%, impacting both genders. 3 It has been identified as a significant factor in the degradation of quality of life among the global population. 4 Migraine can be categorized based on the frequency of monthly headache days: Episodic migraine (EM) occur on fewer than 15 days per month, while chronic migraine (CM) is defined as headache occurring 15 or more days per month for more than three months, with at least 8 days fulfilling migraine criteria. 5
Migraine is a neurological disorder that tends to recur throughout the lifespan with multifactorial characteristics. However, the complete understanding of the biological mechanisms underlying this condition is still under investigation. This gap in knowledge has limited progress in the formulation of effective strategies for its prevention and treatment.1,6 Conversely, within lifestyle choices, diet holds a significant position in the onset of headaches disorders including migraine, suggesting that dietary habits could be instrumental in both preventing and managing this condition.7–9 However, it remains uncertain whether these dietary elements serve as a prevention or a trigger for headaches. 10 Nutritional strategies, including the intake of specific micronutrients such as omega-3 fatty acids through diet or supplementation, have been proposed as potential approaches for migraine prevention.11,12
Omega-3 fatty acids are vital constituents of tissues implicated in the development of migraine.13–15 They serve as important precursors for various groups of bioactive lipid compounds. These mediators, which include prostaglandins, leukotrienes, resolvins, and maresins, regulate pain. 16 In addition, these fatty acids are involved in the regulation of multiple biochemical pathways associated with pain. As key components of the cell membranes of vascular, immune, myelin, glial and neuronal cells, fatty acids could transform into neuronal lipid mediators. These mediators possess properties that could be beneficial to health. 13
Specific dietary changes involving omega-3 fatty acids could alleviate pain. Some reviews suggest that supplementation of omega-3 fatty acids improves the frequency and severity of migraine17–19 similar to other first-line treatments. 20 However, these reviews do not include all relevant clinical studies and combine the effects between different migraine types. In addition, they do not consider the different doses and intervention forms that the omega-3 could be supplemented and the GRADE approach to assess de certainty of evidence. Thus, the objective of this systematic review/analysis was to evaluate the efficacy of omega-3 as a supplement or diet in adult patients with migraine, according to different intervention doses and migraine types.
Methods
Data sources and inclusion criteria
The current study is a systematic review of randomized clinical trials (RCTs) with meta-analysis according to the PRISMA guidelines. 21 The study protocol was registered in PROSPERO (CRD42022296249). The main outcomes were migraine attack frequency and duration, pain intensity evaluated by the visual analog scale (VAS), and/or the impact of migraine. Adverse events were also evaluated.
We included RCTs that evaluated the effects of omega-3 or omega-6 fatty acid supplementation on clinical outcomes in adult patients diagnosed with migraine. These trials were compared with placebo, adjuvant therapies, or any other intervention. The interventions involving omega-3 or omega-6 fatty acid supplementation encompassed both dietary and pharmacological approaches. In addition to omega-3 or omega-6 fatty acid supplementation, we considered trials that included any other co-interventions, as long as these were also present in the control group. Studies involving pregnant patients were excluded, as were those that assessed interventions involving multivitamins comprising more than two distinct substances, including omega-3 or omega-6 fatty acids.
The research was carried out comprehensively in the Cochrane Central-Ovid, Scopus, Embase, and Web of Science databases using the MeSH- and EMTREE-terms “Migraine,” “Fatty- acids,” and others. The detailed search strategies for the databases can be found in Supplementary Table S1. The date up to which the search was made was February 15, 2023, and the updated date was November 7, 2025. An exhaustive search was made of the references cited in the selected studies using the Google Scholar search engine (https://scholar.google.com/), in parallel with an examination of the bibliographic references of the selected studies.
Study selection and data extraction
First, the results of each of the searches were exported to the free online software Rayyan QCRI (https://rayyan.qcri.org; Qatar Computing Research Institute, Qatar Foundation, Qatar) and duplicate references were eliminated. The titles and abstracts were initially reviewed by two groups of two independent reviewers (FJM, FMT, PAGR, APL), and a full-text assessment was then performed. In both phases, a third reviewer resolved any disagreements (CAAR). Supplementary studies were selected according to the previously mentioned criteria for bibliographical references and their citations.
Data from the included studies were extracted independently by the two groups of investigators (FJM, FMT, PAGR, APL) using a data collection form in Microsoft Excel (Microsoft, Washington, USA). For all included studies, we obtained data on the intervention groups receiving omega-3 or omega-6 supplementation, together with data from the appropriate control groups. Each selected article provided the following data: Name of author, year of publication, country, population, dates of recruitment (in months and years), study duration (in months), criteria for selection, criteria for definition of migraine, average age, intervention (concentration, dose, route of administration, time, co-intervention), control (concentration, dose, route of administration, time, co-intervention), outcomes, funding and authors’ conflict of interest. Numeric results were obtained from the reported outcomes at the follow-up measurement and their mean difference for each arm of the study. In the event of disagreements, both researchers would resolve by consensus.
Risk of bias and certainly of evidence
Two independent authors (FJM, PAGR) used Cochrane's risk of bias tool version 2 for RCTs to evaluate systematic errors in the design, implementation, analysis, and outcome reporting of each individual study. They assessed one general domain and five specific domains: bias in the randomization process, bias from planned intervention deviations, bias from missing information, bias from outcome measurement, and bias from outcome reporting. For each item, the potential outcomes of high risk of bias, some bias concerns, and low risk of bias were considered. In case of differences, a third reviewer helped to reach a consensus (CAAR).
In addition, we applied the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach to establish confidence in the evidence and to grade the confidence in the results for each outcome as being very low, low, moderate, or high. Our evaluation of the evidence on each outcome focused on the risk of bias, impression, inconsistency, indirect evidence and publication bias. 22 The risk of bias was evaluated according to the findings of RoB 2.0 for each included trial. 23 Imprecision was evaluated by reviewing the calculated optimal information size for each quantitative or qualitative outcome following GRADE approach. 24 Inconsistency was evaluated by the heterogeneity of the results of the meta-analyses, with an I2 > 50% indicating substantial heterogeneity that could not be accounted for by alternative hypotheses. 25 Publication bias was qualitatively assessed considering study funding and author conflicts of interest. 26 The certainty of evidence was established for all primary outcomes of this systematic review.
The assessment of risk of bias and certainty of evidence was conducted independently by two reviewers and in case of discrepancy, consensus was sought by a third reviewer (PAGR, FJM, CAAR). The findings are presented in the form of a summary of findings using standardized language, 27 and the size of the treatment effect has been interpreted according to the minimum clinically important differences. 28
Statistical analysis
Meta-analyses were performed when one or more studies had similar measures and outcomes, and depending on the heterogeneity of those data, the random or fixed effects method and the inverse variance method were used. The mean difference (MD) and 95% confidence intervals (95% CI) are given as the measures of association. The MD was used because of the uniformity of the scale of the measures reported across studies. In most cases, the last measure of the outcome during the follow-up was used in obtaining the MD. In the case of the MIDAS measure of treatment outcome, since this was available, we used the change in values from baseline to follow-up for the MD. We considered subgroups for complementary meta-analysis according to migraine type (episodic vs chronic migraine) and omega-3 doses. Review Manager version 5.4 (The Cochrane Collaboration, London, UK) was used for all statistical analyses.
Results
Study selection
After the first search, 1411 documents were screened, and 47 were evaluated in full text. Thirty-two studies were excluded because they were documents without results or were not RCTs (excluded reports and reasons in Supplementary Table S2). In addition, one article from a previously identified study 29 and one article from a new study 30 were retrieved from the citation search. Then, after the update search, one article from a previously identified study 31 and three new studies32–34 were retrieved. Therefore, we obtained 15 articles with results from 11 individual studies (Figure 1).
Flow diagram for study selection (flowchart).
Study characteristics
Five studies were conducted in Iran,30,33–36 three in the USA,15,37,38 one in Brazil, 39 one in France, 40 and one in Taiwan. 32 Most trials reported omega-3 supplementation with varying dosing in milligrams and in terms of eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA) or alpha-linoleic acid (ALA). Six studies assessed omega-3 supplementation as an isolated intervention (capsules or sachets diluted in water).32,33,35,36,39,40 Additionally, two studies investigated omega-3 as part of a dietary approach high in omega-3 with 1500 mg. of EPA plus 1500 to 2000 mg. of DHA,15,29,37,41 and two studies examined omega-3 as a co-intervention with vitamin D supplementation, 38 carnitine, 34 or sodium valproate. 30 Oral supplementation omega-3 varied between 1000 and 6000 mg per day with 180 to 2000 mg. of EPA plus or minus 120 to 600 mg. of DHA. Notably, no study was found to assess the effect of omega-6 supplementation.
Most of the studies employed placebo as the control group; however, two studies utilized a low or average omega-3 diary diet as the control.15,37 Participant numbers varied, ranging from 40 to 1287, and the follow-up duration spanned from 2 months to 4.6 years. These studies were conducted in clinical ambulatory care centers and included non-pregnant adults with mostly CM15,30,33,37,39 or EM,32,34,35,40 with or without aura, as classified by ICHD-1, 40 ICHD-2,15,30,35–37 or ICHD-3 criteria.32–34 Some baseline clinical characteristics, including comorbidities, were not consistently reported across trials. However, most studies excluded participants with significant comorbidities and were using vitamin supplementation or headache medication before the study initiation (Table 1).
Characteristics of the individual included studies.
Chronic primary headache ICHD-2 criteria: headaches ≥ 4 h/day and ≥ 15 days/month for at least 3 months and a headache history of ≥ 2 years under the care of a physician for headache management; migraine with or without aura ICHD-2 and ICHD-3: At least 5 attacks lasting 4 to 72 h (untreated or unsuccessfully treated), with headaches (with at least two of the following characteristics: unilateral location, pulsating quality, moderate or severe pain intensity, or aggravation by or causing avoidance of routine physical activity), associated with at least one of the following: nausea and/or vomiting, or photophobia and phonophobia, and not attributed to another disorder. LA: Linoleic acid; AC: Arachidonic acid; ALA: Alpha-linoleic acid; EPA: Eicosapentaenoic acid; DHA: Docosahexaenoic acid/
Summary of the findings of omega-3 fatty acid supplementation in adults with migraine.
95% CI: 95% confidence interval; GRADE: Grading of Recommendations Assessment, Development and Evaluation; HIT-6: Headache Impact Test-6; MSQ: Migraine specific quality of life questionnaire; PROMIS-29 Patient reported outcomes measurement information system; RCT: Randomized clinical trial; SF-12: 12-item Short Form Survey; VAS: Visual Analog Scale.
Decrease two levels because of the high risk of bias in individual trials.
Decrease one level for imprecision because the total sample size is lower than the optimal size between 32 and 20958.
Decrease one level for imprecision because the total sample size is lower than the optimal size between 26 and 152584.
Decrease one level for inconsistency I2 > 70%.
Decrease one level for imprecision because the total sample size is lower than the optimal size between 64 and 652.
The moderate effect considering the minimal important change of the Migraine Disability Assessment score after nonpharmacological treatment of migraine is 4.5 points (28).
Synthesis of the results and certainty of evidence
Ten studies evaluated the three outcomes related to the frequency of migraine attacks: Diminution of frequency of migraine attacks, daily headache hours, and monthly headache days.15,30,32–35,37–40 Omega-3 fatty acid supplementation was associated with a significantly lower number of daily headache hours (MD = –1.74 h; 95% CI: −2.29 to −1.19; Figure 2(B)) and monthly headache days (MD = –2.39 days; 95% CI: −3.78 to −1.00; Figure 2(C)). The evidence of these outcomes was very uncertain. However, there was no significant difference for the dichotomic outcome diminution of frequency of migraine attacks (Figure 2(A)), with low certainty of evidence (Table 2).
Forest plots of omega-3 supplementation us placebo on outcomes related to (a) Diminution of frequency of migraine attacks. (b) Daily headache hours. (c) Monthly headache days.
Then, the meta-analysis of six studies30,32–35,37 reported that the omega-3 fatty acid supplementation was not associated with lower units of migraine attack intensity using the VAS (MD = –0.57 units; 95% CI: −1.20 to 0.06; Figure 3(A)). However, the certainty of evidence on this outcome was very low (Table 2).
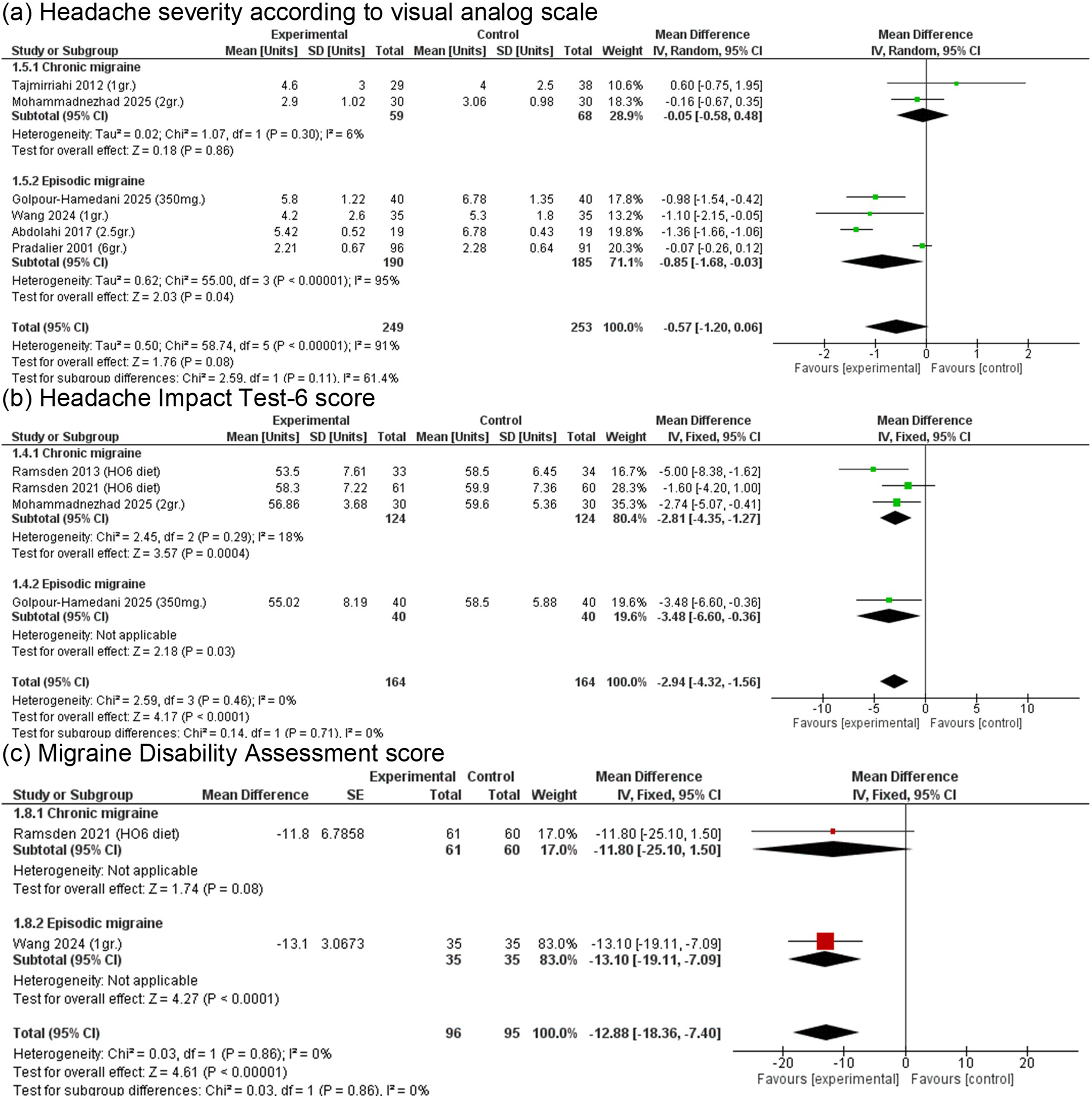
Forest plots of omega-3 supplementation us placebo on outcomes related to (a) Pain headache according to the VAS. (b) Headache impact test-6 score. (c) Migraine disability assessment score.
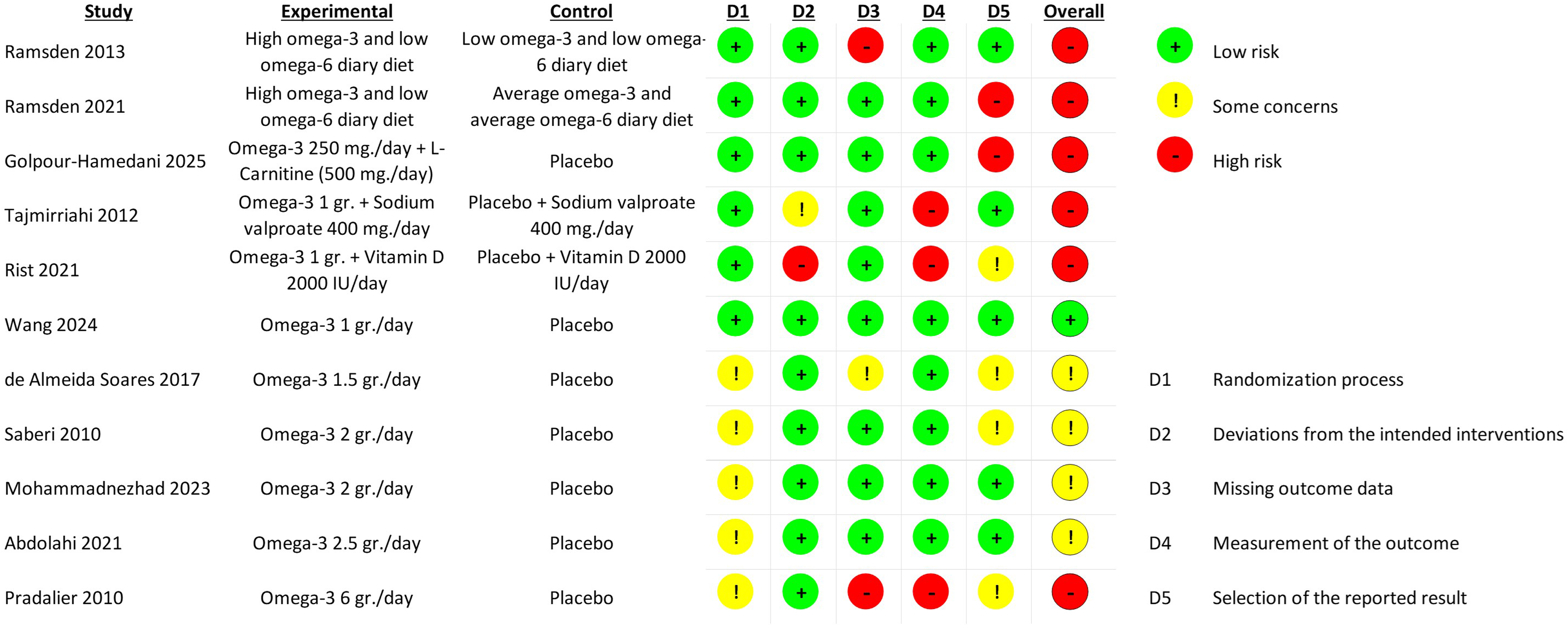
Risk of bias of individual studies using the Cochrane risk of bias 2.0 tool.
Five studies evaluated outcomes related to the impact of migraine attacks.15,32–34,37 Omega-3 fatty acid supplementation was associated with a significantly lower score of the Headache Impact Test score (MD = –2.94 units; 95% CI: −4.32 to −1.56; Figure 3(B)) and the Migraine Disability Assessment score (MD = –12.88 units; 95% CI: −18.36 to −7.40; Figure 3(C)). Regarding quality of life, one study reported that a high omega-3 fatty acid concentration diet increased the health-related quality of life with a 12-item Short Form Survey score (MD = 6.70 units; 95% CI: 2.59 to 10.81), but not the Patient Reported Outcomes Measurement Information System-29 score (MD = 1.20 units; 95% CI: −1.50 to 4.00). However, another study reported an improvement in the migraine-specific quality of life questionnaire score with 1-g daily supplementation of omega-3 fatty acid (MD = 6.70 units; 95% CI: 2.59 to 10.81). The certainty of evidence for these outcomes was low (Table 2).
Finally, four studies reported any adverse effects of omega-3 fatty acid supplementation.32,33,37,40 In the overall analysis, omega-3 fatty acid supplementation was not associated with increase or decrease of any adverse effects, severe effects, or withdraw of intervention due to adverse effects (Supplementary Figures S1-S3). Specifically, considering the intervention dosing and presentation, in the case of a diet with high omega-3 fatty acid concentration, they reported a low frequency of any adverse events (8%) related or possibly related to the intervention with no differences with the control group. However, the participants who used daily 6 or omega-3 fatty acid capsule supplementations reported high digestive tract adverse effects such as nausea (5.1%) and eructation (4.6%). Otherwise, the participants who used daily 2-gr omega-3 fatty acid capsule supplementations reported no differences in adverse effects versus placebo.
Assessment of the risk of bias
Out of the ten included studies, one had a low overall risk of bias 32 ; four studies raised some concerns,33,35,36,39 and the others five had a high overall risk of bias.15,30,34,37,38,40 Different domains are affected by bias in most of the selected studies. Domain 5, which assesses the selective results of the outcomes, identified concerns about the registration of a protocol for six RCTs. Furthermore, domain 1, which assesses the correct randomization of participants, presents some concerns or five studies. Additionally, three studies probably did not adequately describe the measurement of their outcomes (Figure 4).
Other three studies did not report on their funding statement and their conflicts of interest. Publication bias was qualitatively assessed. There were different public and private institutions funding some of the studies, and there is no important reported conflict of interest, so the probability of publication bias is low.
Subgroups analysis
Omega-3 supplementation as a diet was assessed only in patients with mostly CM. The intervention in this subgroup lowered the daily headache hours and monthly headache days. However, it did not significantly change some scores of impact and quality of life related to headaches. Omega-3 supplementation according to daily oral doses was informed by single trials. The omega-3 supplementation as daily capsules in 1 and 1.5 gr./day did not change the outcomes in patients with CM. Otherwise, the dose of 2 g/day slightly improved the monthly headache days and the HIT-6 score. In patients with EM, we observed a dose-response effect on the omega-3 supplementation with higher doses of 2 and 2.5 g/day improved the frequency of headaches and the migraine-related impact scores. However, the 6 g/day did not change the frequency and pain intensity outcomes (Table 3).
Subgroup analysis of omega-3 fatty acid supplementation in adults with migraine according to the intervention dose and type of migraine.
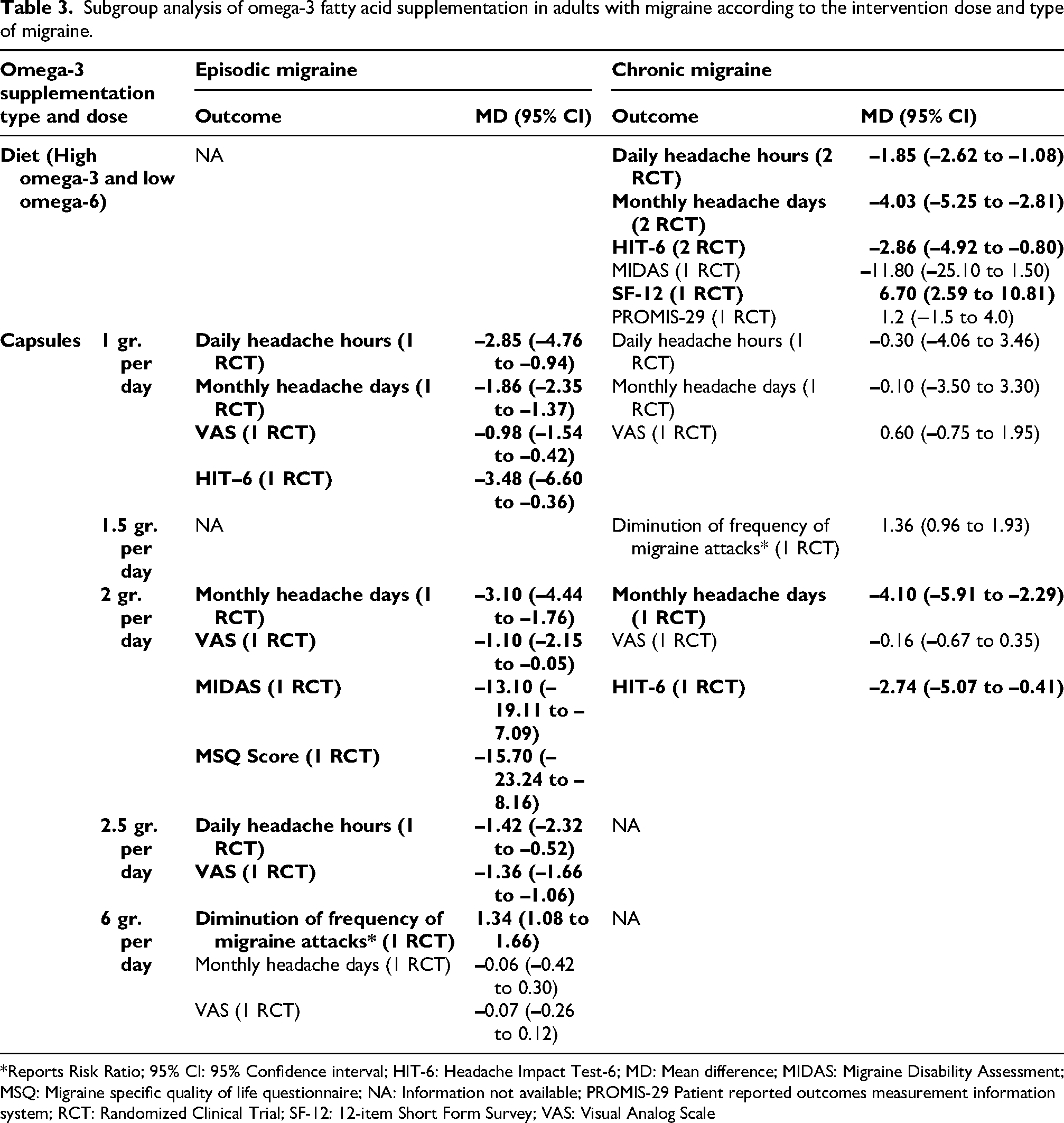
*Reports Risk Ratio; 95% CI: 95% Confidence interval; HIT-6: Headache Impact Test-6; MD: Mean difference; MIDAS: Migraine Disability Assessment; MSQ: Migraine specific quality of life questionnaire; NA: Information not available; PROMIS-29 Patient reported outcomes measurement information system; RCT: Randomized Clinical Trial; SF-12: 12-item Short Form Survey; VAS: Visual Analog Scale
Discussion
Summary of the results
Omega-3 supplementation, as capsules or via diet, was associated with improvements in migraine outcomes. The meta-analyses showed significant reductions in headache frequency and impact compared to placebo. EM patients appeared to show more consistent benefit than those with CM. However, dose-specific findings, particularly at 2.0 to 2.5 g/day, are based on limited data from single studies and should cautiously interpreted. Diet-based omega-3 interventions likewise reduce the frequency of headaches in CM patients. Overall, the certainty of evidence was judged to be low to very low.
Beneficial effects in em and cm
Omega-3 interventions in trials that included adults mainly with EM assessed EPA and DHA delivered as capsules at 1 to 2.5 g/day. These interventions were associated with consistent and clinically meaningful reductions in headache frequency and disability measures. In pooled and individual trials, omega-3 supplementations reduced monthly headache days and improved VAS and HIT-6 in several studies,32,34,35 whereas very high-dose (6 g/day) trials did not show any benefit. 40 These effects are biologically plausible given the modulation of pro- and anti-inflammatory lipid mediators by omega-3 s, including specialized pro-resolving mediators within TRPV1 and TRPA1 ion channels, and the possible down-regulation of trigeminovascular inflammation. These therapeutic mechanisms align with EM pathophysiology.42–44
Dietary trials that specifically targeted a high- and low-omega-3 and low-omega-6 regimen produced the clearest benefit in adults with CM. These studies replaced habitual dietary fatty acids with an EPA- and DHA-rich pattern and reported meaningful reductions in monthly headache days, daily headache hours, and HIT-6 scores.15,29,37 However, capsule-based trials in CM showed heterogeneous results (1 g/day often inactive; some benefit reported at 2 g/day), suggesting a possible threshold or interaction with background prophylactic therapies. The issue that there is no consistent benefit for omega-3 supplements in CM shows the complexity in its pathophysiology. While EM involves transient activation of the trigeminovascular system and reversible peripheral sensitization, CM is characterized by sustained neuroinflammation, central sensitization, and no conditioned pain modulation.45,46
Safety and adverse effects
Omega-3 interventions were generally well tolerated across the included trials. The most common adverse effects were gastrointestinal (nausea, abdominal discomfort, eructation) and were dose-related, notably more frequent with 6 g/day supplements. 40 These may limit adherence in certain individuals, highlighting the importance of tailoring the dosage based on both efficacy and tolerability. High doses of omega-3 supplementation might increase the risk of bleeding, 47 development of atrial fibrillation, 48 and worsening of hematocrit and some liver enzymes. 49 Although no serious treatment-related events were reported in the trials, key safety domains such as bleeding and cardiac endpoints, changes in liver enzymes, and long-term safety were not systematically assessed across studies.
Therefore, when recommending omega-3 supplementation, clinicians should start at moderate doses and up-titrate only if tolerated, and counsel patients about potential gastrointestinal effects and strategies to reduce them such as taking with food and split dosing. Routine baseline or follow-up laboratory monitoring is optional but may be reasonable for patients with hepatic or cardiac disease or high bleeding risk. 50 Overall, while current evidence supports the safety of short-to-intermediate term omega-3 supplementation, further research with longer follow-up and a standardized report of adverse effects is warranted to confirm its tolerability over time and diverse populations.
Clinical and practice implications
Adults consume around 800 to 1600 mg/day of omega-3 mostly from vegetable oils, with lower doses of EPA and DHA between 30 and 200 mg/day.51,52 These doses are under the 2 to 2.5 gr./day range with EPA dosing of 1200 to 2000 mg/day and DHA of 600 to 2000 mg/day associated with clinical benefits in trials in both EM and CM. Therefore, regular diet alone may be insufficient for most patients to achieve therapeutic omega-3 exposure. Interestingly, a recent network meta-analysis suggested a dose–response effect with clinically meaningful benefit only at doses >4 g/day. 20 However, this analysis combined heterogeneous populations, including children, adolescents, adults, EM and CM, and compared omega-3 interventions to standard pharmacologic prophylaxis, limiting applicability. In contrast, our findings in adults indicate a ceiling effect, with better benefits observed at 2 to 2.5 g/day but no additional efficacy and poorer tolerability at very high doses (6 g/day). This effect could be related to a pro-resolvine lipid pathway saturation, metabolic competition with other fatty acids, or compensatory down regulation of receptors. 44 Therefore, for EM, current evidence supports short-to-medium term supplementation of 2 to 2.5 g/day of EPA + DHA for 12–16 weeks as an adjunctive preventive option, particularly for patients seeking non-pharmacologic strategies or with contraindications to standard preventives.
For CM, evidence instead supports structured dietary modification with a high-omega-3/low-omega-6 regimen, targeting EPA 1500 mg + DHA 2000 mg/day, while reducing linoleic acid to <2% of energy, arachidonic acid to ∼150 mg/day, and ALA to ∼1.8% of energy. This diet is achievable through increased oily-fish intake (e.g., mackerel, salmon, tuna, trout), high-quality oils (macadamia nut, extra-virgin olive, cod liver), 53 and avoidance of processed foods, low fat fish or poultry, and certain milk-derived food like cheese and yogurt.15,29,37 Implementation and adherence of any dietary or supplementation intervention can be challenging with limited feasibility in clinical practice. 54 Therefore, individual follow-up, counseling, and dietitian support may be necessary. Overall, clinicians should individualize recommendations, integrate mentioned dietary interventions with habitual dietary intake, set realistic expectations, consider the use of oral supplementation with separated dosing based on current trials to avoid adverse effects, and reassess benefit after 8–12 weeks given the low certainty and heterogeneity of current evidence.
Limitations and strengths
This systematic review has several limitations that include many small RCTs, substantial risk of bias, heterogeneity in formulations (diet vs. capsules, EPA:DHA ratios, ALA vs marine food, and doses from 1 to 6 gr/day), follow-up lengths and outcomes, and limited safety reporting, hence low/very-low certainty for almost all endpoints. Different omega-3 fatty acids, including EPA, DHA, and plant-derived ALA have distinct biological properties and metabolic pathways, which may contribute to heterogeneity in clinical effects observed across studies. Also, omega-3 supplementation results according to daily oral doses were informed by single trials, limiting the robustness and generalizability of these findings. In addition, our findings do not capture or considered other relevant variables like the baseline fish/omega-3 serum concentration and mental health disorders of participants. These variables could influence the overall effect and should be considered in future research.
Furthermore, the strengths of this review are the prespecified protocol, comprehensive database searching, use of GRADE to transparently rate certainty, inclusion of both dietary and supplemental approaches, and subgroup analyses by migraine type and dosing that provide practical and actionable recommendations for clinicians in real-world scenarios. In addition, this review includes recent randomized trials and provides an updated synthesis of the available evidence on omega-3 supplementation in adults with migraine, compared with recent previous reviews.17,19,20,55 Overall, although limited by quality evidence, this review provides a complex synthesis that may benefit future research and clinical decision making. In future trials and clinical practice with patients with migraine a baseline fish/omega-3 intake should be captured.
Conclusion
Omega-3 supplementations may offer a clinically relevant benefit in adults with migraine with an apparently well-tolerated safety profile, particularly for patients seeking nonpharmacological preventive strategies, despite the low to very low certainty of evidence. Results are stronger for a modest benefit in EM with capsule doses in the 1–2.5 g/day range and for dietary high-EPA/DHA with low-omega-3 dietary strategies in CM. Heterogeneity in the study design, dosing, and outcome measurement must be considered for individual decision-making. Future research should focus on identifying optimal dosing strategies, evaluating long-term effects, and confirming benefits across diverse patient populations and migraine subtypes.
Public health relevance
Omega-3 interventions may mildly reduce migraine frequency and disability in adults.
Benefits appears to be more consistent in episodic migraine than chronic migraine.
Optimal effects might occur with moderate doses (≈2–2.5 g/day) or structured dietary interventions.
Supplemental Material
sj-docx-1-rep-10.1177_25158163261454627 - Supplemental material for Dosing effects of omega-3 fatty acid interventions in adults with migraine: Systematic review and meta-analysis of randomized clinical trials
Supplemental material, sj-docx-1-rep-10.1177_25158163261454627 for Dosing effects of omega-3 fatty acid interventions in adults with migraine: Systematic review and meta-analysis of randomized clinical trials by Christoper A. Alarcon-Ruiz, P. Alejandra Goicochea-Romero, Fátima Jiménez-Mozo, Frank Mayta-Tovalino, Andrés Pacherres-López, Fernando M. Runzer-Colmenares and Mario F.P. Peres in Cephalalgia Reports
Supplemental Material
sj-png-2-rep-10.1177_25158163261454627 - Supplemental material for Dosing effects of omega-3 fatty acid interventions in adults with migraine: Systematic review and meta-analysis of randomized clinical trials
Supplemental material, sj-png-2-rep-10.1177_25158163261454627 for Dosing effects of omega-3 fatty acid interventions in adults with migraine: Systematic review and meta-analysis of randomized clinical trials by Christoper A. Alarcon-Ruiz, P. Alejandra Goicochea-Romero, Fátima Jiménez-Mozo, Frank Mayta-Tovalino, Andrés Pacherres-López, Fernando M. Runzer-Colmenares and Mario F.P. Peres in Cephalalgia Reports
Supplemental Material
sj-png-3-rep-10.1177_25158163261454627 - Supplemental material for Dosing effects of omega-3 fatty acid interventions in adults with migraine: Systematic review and meta-analysis of randomized clinical trials
Supplemental material, sj-png-3-rep-10.1177_25158163261454627 for Dosing effects of omega-3 fatty acid interventions in adults with migraine: Systematic review and meta-analysis of randomized clinical trials by Christoper A. Alarcon-Ruiz, P. Alejandra Goicochea-Romero, Fátima Jiménez-Mozo, Frank Mayta-Tovalino, Andrés Pacherres-López, Fernando M. Runzer-Colmenares and Mario F.P. Peres in Cephalalgia Reports
Supplemental Material
sj-png-4-rep-10.1177_25158163261454627 - Supplemental material for Dosing effects of omega-3 fatty acid interventions in adults with migraine: Systematic review and meta-analysis of randomized clinical trials
Supplemental material, sj-png-4-rep-10.1177_25158163261454627 for Dosing effects of omega-3 fatty acid interventions in adults with migraine: Systematic review and meta-analysis of randomized clinical trials by Christoper A. Alarcon-Ruiz, P. Alejandra Goicochea-Romero, Fátima Jiménez-Mozo, Frank Mayta-Tovalino, Andrés Pacherres-López, Fernando M. Runzer-Colmenares and Mario F.P. Peres in Cephalalgia Reports
Footnotes
Abbreviations
Acknowledgements
None.
Ethical considerations
The current study is a systematic review.
Consent to participate
None required for reviews.
Consent for publication
The authors agree to publish with Cephalalgia Reports, if the manuscript is accepted.
Author contributions
CAAR conceived the study. CAAR conducted drafting of the PROSPERO protocol. All authors contributed to the design of the study. CAAR, PAGR, FJM, FMT, and APL collected data and assured data integrity. CAA performed the statistical analysis on the data obtained. CAAR, APL, FJM, FMT, PAGR prepared the first draft of the report. All authors contributed to its revision and final preparation. All authors guaranteed that all aspects of reliability and of the freedom from bias of the discussed interpretation of the data presented are assured.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that supports the findings of this study are available on request from the corresponding author.
Open practices
Not applicable
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.