
Abstract
Background
Migraine impairs daily functioning, including driving, but its impact relative to epilepsy remains underexplored. While epilepsy is well-known to increase driving accident risk, the impact of migraine on driving safety remains underexplored. We aimed to compare driving risks between the two groups.
Methods
We conducted a 3-month observational, cross-sectional study. Consecutive patients with migraine or epilepsy attending a tertiary outpatient clinic, all holding a driving license, completed questionnaires collecting sociodemographic, clinical data, and accident history.
Results
A total of 135 patients participated: 77 with migraine and 58 with epilepsy. Migraine predominated among females, while epilepsy among males [84% (65/77) vs. 68% (26/38), p < 0.001)]. Educational level was lower in epilepsy patients (p < 0.001). In epilepsy, 62.7% (32/51) reported seizures with impaired consciousness; 67.2% (39/58) had fewer than one seizure per trimester. In migraine, 66% (51/77) reported visual aura. Accident history was more frequent in migraine than epilepsy [54.5% (42/77) vs. 31% (18/58), p = 0.009] but accidents attributed to neurological causes were comparable [20.5% (8/39) aura-related vs. 18.8% (3/16) seizure-related, p = 0.882]. Most patients with migraine (54/77, 70%) refrained from driving during attacks; 23% (18/77) supported legal driving restrictions.
Conclusion
Migraine may confer a driving accident risk comparable to epilepsy, underscoring the need for individualized clinical risk assessment.
This is a visual representation of the abstract.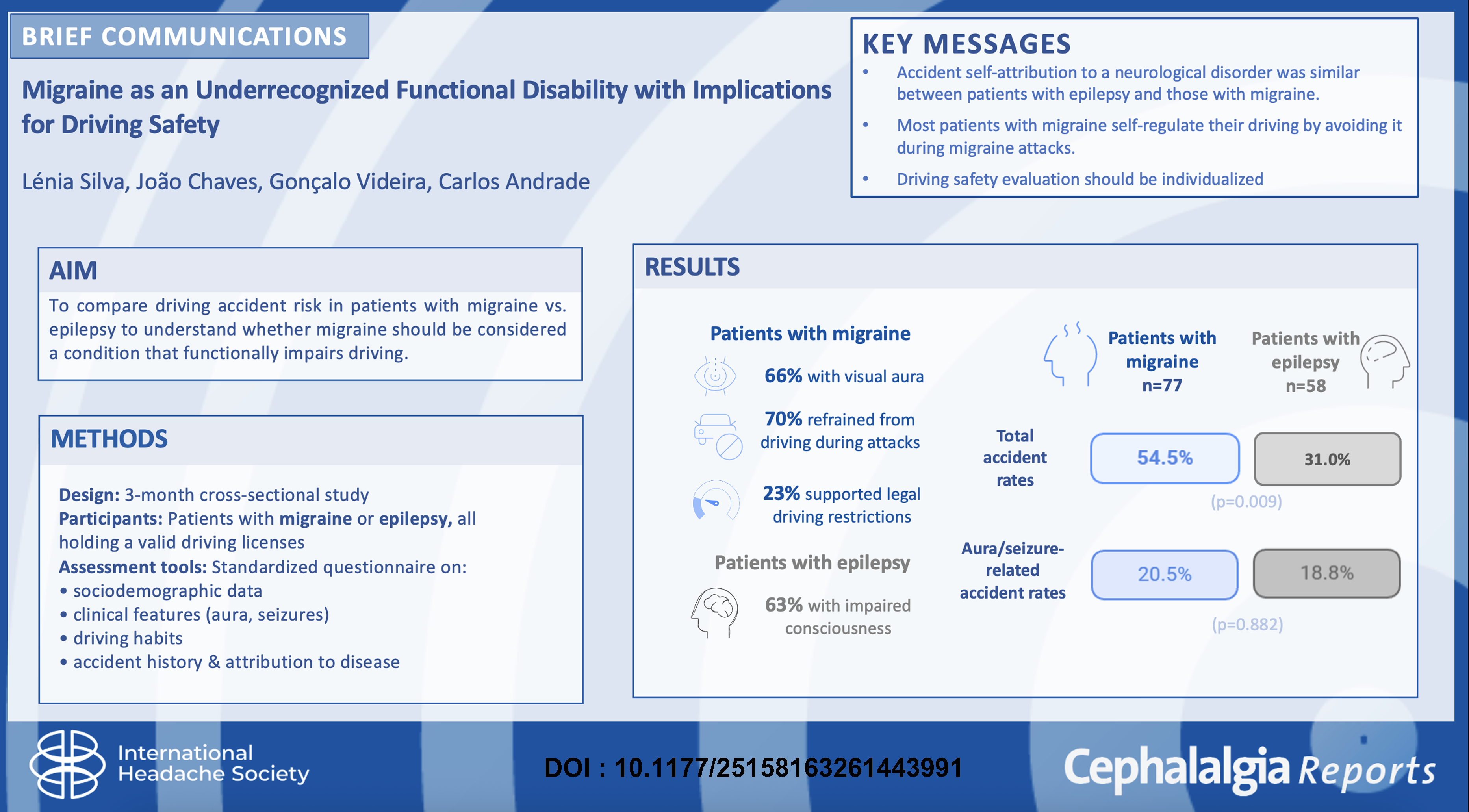
Introduction
As a highly disabling neurological condition, migraine extends its influence beyond pain, impairing essential aspects of daily functioning, including driving. 1 Although epilepsy is well-known for its risk of sudden loss of consciousness, which justifies strict driving licensing restrictions worldwide, the impact of migraine, especially with aura or associated cognitive and vestibular symptoms, on driving safety is less well recognized.2,3 Both conditions can cause transient neurological impairments that may compromise driving performance and increase accident risk, but clinical guidelines and legal frameworks differ markedly.
In Portugal, patients with epilepsy are legally prohibited from driving for one year following the last seizure with loss of consciousness. 4 Nevertheless, their driving license is not formally revoked during this period, allowing patients to hold valid licenses despite a seizure history and allowing them to return to driving as soon as one year without seizures has passed. On the other hand, there are currently no legal restrictions on driving in patients with migraine (with or without visual, ophthalmic, or brainstem auras). Legislation regarding driving with epilepsy was explained or reexplained to the patients who accepted to participate.
Given these considerations, we designed this study to compare driving habits and accident proportion between patients with migraine and those with epilepsy. While these conditions are distinct, epilepsy serves as a relevant reference condition because its association with driving risk is recognized and formally regulated. This comparison aims to contextualize the potential impact of migraine on driving safety rather than to imply neurological equivalence between the two disorders.
Methods
We conducted an observational, cross-sectional study based on questionnaires administered consecutively over 3 months to patients attending the Epilepsy and Headache outpatient clinics of a tertiary hospital in Portugal. Eligible participants were adults with a diagnosis of migraine or epilepsy, all holding valid driving licenses. Patients diagnosed with both migraine and epilepsy were excluded from the study. A standardized questionnaire collected data on sociodemographic characteristics, clinical history, driving habits, and motor vehicle accident history. Patients were also asked whether they considered their neurological condition to have contributed to previous accidents and whether they self-regulated their driving behavior. This study was approved by the Institutional Ethics Committees (010-CAC/010-CE), and all participants provided written informed consent in accordance with the Declaration of Helsinki.
Continuous variables are reported as mean (standard deviation) and were compared using the Mann–Whitney U test. Categorical variables are presented as counts (percentages) and were compared using the chi-square test. Some variables contained missing data; therefore, the total number of participants included in each analysis may vary. The exact sample size for each variable is reported alongside the corresponding results. Statistical significance was defined as p < 0.05. All statistical analyses and graphical representations were performed using IBM SPSS Statistics v28 (IBM, New York, USA).
We used the STROBE reporting guideline to draft this manuscript, and the STROBE reporting checklist when editing, which is included in the supplements.5,6
Results
A total of 135 patients were included: 77 with migraine and 58 with epilepsy. Mean ages were similar between groups [46 (10) vs. 47 (14) years, p = 0.855] and among females, migraine was more frequent (65/77; 84%), whereas epilepsy predominated among males (26/38; 68%), (p < 0.001). A significantly higher proportion of patients with migraine had a bachelor's degree or higher compared to patients with epilepsy [66% (51/77) vs. 33% (19/58), p < 0.001]. Among patients with epilepsy, 62.7% (32/51) reported seizures with impaired consciousness, while 11% (8/74) reported impaired consciousness in migraine crisis. In the epilepsy group, 67.2% (39/58) had less than one seizure per trimester in the preceding 2 years (implying that some patients are not aware of the legislation related to driving with epilepsy). Among migraine patients, 32% (25/77) had 8–15 migraine days per month and 66% (51/77) reported visual aura.
Motor vehicle accident history was more frequently reported by patients with migraine than patients with epilepsy [54.5% (42/77) vs. 31% (18/58), p = 0.009]. Nevertheless, the proportion of accidents attributed by the patient to his/her neurological disorder was similar between groups [20.5% (8/39) aura-related vs. 18.8% (3/16) seizure-related, p = 0.882]. Two serious accidents requiring hospital evaluation occurred in each group. Importantly, most patients with migraine recognized the impact of their condition on driving, with 70% (54/77) reporting that they had voluntarily refrained from driving during attacks, highlighting a degree of self-regulation, while 23% (18/77) expressed support for potential legal restrictions.
Discussion
Patients with migraine in our cohort frequently recognized the impact of their condition on driving and reported self-regulatory behaviors, with most refraining from driving during migraine attacks. Despite these precautions, accidents were commonly reported, and a relevant proportion were considered by patients themselves to be related to migraine symptoms, particularly aura. 7 Population-based studies confirm the functional impact of migraine on driving: in Spain, 63% of drivers considered that migraine or headache impaired driving “a lot,” and in Italy, 20% of patients reported being severely limited in driving due to migraine.8,9 In New Zealand, 18% of treated migraine patients reported a crash, compared to 10% in nonmigraine controls, and a Canadian population survey found a higher proportion of accident history among respondents with migraine (12% vs. 7%, p < 0.0001).7,10 Among older American adults newly diagnosed with migraine, crash risk increased threefold in the subsequent year. 11 Older studies also showed a 1.5–2.3-fold increased odds of driver injury in people with migraine, and a hospital-based study in the United Arab Emirates found migraine-related accidents accounted for 4.7% of accident drivers.3,12
Our comparison with epilepsy provides a clinical reference point rather than implying equivalence between conditions. In our sample, the proportion of accidents attributed by patients to their neurological condition appeared similar between migraine and epilepsy groups, despite differences in legal regulation and disease characteristics. This finding underscores that migraine, although not subject to formal driving restrictions, may be associated with driving impairments perceived by patients as clinically relevant.
The relatively high proportion of patients reporting visual aura and frequent migraine attacks likely reflects the tertiary care setting of our study. However, patient recruitment was consecutive and based solely on driving license status, without preferential selection for any specific clinical features. Therefore, while our findings may not be generalizable to the broader migraine population, they provide valuable insights into driving risks among patients with more severe migraine presentations.
Our study has several limitations. The cross-sectional design precludes causal inference and limits temporal understanding of accident risk. The reliance on self-reported data introduces recall bias, particularly regarding accident history and symptom reporting. The comparison of accidents attributed to neurological causes is based on a small number of events, limiting statistical power. In addition, missing data may have affected the precision of some analyses and should be considered when interpreting the results. We did not assess driving exposure, migraine treatments, cognitive function, or vestibular symptoms, all of which could influence driving ability and risk. Aura was evaluated indirectly via patient self-report, which may lead to misclassification or overestimation. Despite these limitations, the strengths of our study include consecutive patient recruitment and the direct assessment of accidents attributable to migraine attacks rather than diagnosis alone.
This study is original in directly comparing the accident occurrence in migraine patients with a cohort of epilepsy patients, a group subject to strict legal driving restrictions, while most previous studies either included healthy controls or no comparator at all. This approach highlights the relative underrecognition of migraine's functional impact.
Our findings suggest that migraine patients may experience more driving-related accidents, despite attempts at self-regulation. Given the higher frequency of reported accidents in patients with migraine, our results highlight the need for individualized clinical assessment of driving risk in those patients. Importantly, we intend to raise awareness of these issues and stimulate further detailed research into the impact of migraine on daily life and driving safety. While we recognize the limitations, migraine's potential influence on driving is an underappreciated but critical topic that deserves discussion and more rigorous future investigation. Clinicians should be aware that migraine is more than a painful condition, as it can acutely impair reaction times, visual processing, and cognitive control. 2 Although formal guidance on counseling patients with migraine about driving is lacking, individualized risk assessment, considering visual aura, cognitive fog, vestibular symptoms, and patients’ own perceptions should become a routine of clinical practice.
Public health relevance
Accidents were frequently reported by patients with migraine, and a substantial proportion was perceived as related to migraine attacks or aura.
Most patients with migraine self-regulate driving by avoiding it during attacks.
Findings highlight the need for individualized driving risk assessment in migraine.
Footnotes
Ethical considerations
This study was approved by the Institutional Ethics Committees (010-CAC/010-CE).
Consent to participate
All participants provided written informed consent in accordance with the Declaration of Helsinki.
Consent for publishing
The authors target journal is Cephalalgia Reports.
Author contributions
Lénia Silva, Gonçalo Videira, and Carlos Andrade contributed to conceptualization and design. Lénia Silva, Gonçalo Videira, and Carlos Andrade contributed to data acquisition, literature review, and analysis. Lénia Silva contributed to manuscript drafting. João Chaves, Gonçalo Videira, and Carlos Andrade contributed to manuscript revision and commentary. Lénia Silva, João Chaves, Gonçalo Videira, and Carlos Andrade contributed to final approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.