
Abstract
Aim
To determine whether there is a difference in the time to complete a rapid number naming task during the interictal state compared to prodrome, migraine headache, postdrome phases of migraine and non-migraine headache, and characterize non-headache symptoms experienced during these phases.
Methods
This prospective longitudinal cohort study evaluated 30 adults with migraine with or without aura who completed diary entries and a timed rapid number naming task at least three times daily for up to four months from October 2020 to July 2022 at a tertiary headache center. Diary entries included self-report of current migraine phase (having a migraine headache, non-migraine headache, prodrome, postdrome, or interictal baseline) and detailed symptoms experienced. The outcome of interest for the timed rapid number naming task was the time to complete the task with zero errors.
Results
Compared to the interictal baseline, the time with zero errors for the rapid number naming task was significantly slower during the prodrome (median (Q1, Q3) 1.0 s slower (0.4, 2.9), p-value 0.010), migraine headache (median (Q1, Q3) 3.8 s slower (2.6, 7.5), p-value <0.001), and postdrome (median (Q1, Q3) 0.9 s slower (0.2, 2.1), p-value 0.011) phases of migraine, and non-migraine headache attacks (median (Q1, Q3) 1.2 s slower (0.1, 3.1), p-value 0.006). For those with migraine with aura (N = 15), the time with zero errors was significantly slower during all phases compared to interictal phase. For those with migraine without aura (N = 15), the time with zero errors was significantly slower only during the migraine headache, but not other phases compared to the interictal phase. The top 5 most reported non-headache symptoms during any phase of migraine and non-migraine headache attacks included fatigue, neck stiffness, light sensitivity, blurred vision/vision changes, and difficulty concentrating.
Conclusions
Among the overall participant cohort, the time with zero errors to complete a rapid number naming task was significantly slower during all ictal phases compared to interictal phase. This was also the case in the migraine with aura cohort but in the migraine without aura cohort there was only a significant difference during the migraine headache phase versus interictal phase. There is overlap in non-headache symptoms between the prodrome, migraine headache, postdrome, and non-migraine headache phases, which may make distinguishing between these phases difficult. Combining subjective data, such as symptom diaries, with objective measures, such as rapid number naming tasks, may allow for more refined assessment of migraine phases and distinguishing migraine from non-migraine headache attacks.
Introduction
Migraine is recognized as more than just a headache disorder. It is a chronic neurologic disease with recurrent attacks defined by a combination of symptoms of head pain, sensory sensitivities, nausea, and vomiting. Migraine consists of overlapping phases of prodrome (commonly referred to as premonitory), aura, headache, and postdrome. Prodrome and postdrome symptoms are common, affecting up to 80% of the migraine population.1–4 Prodrome symptoms can occur up to 48 h before a migraine headache attack; however, the most prominent prodromal change exists within the last 12 h before attack onset. 5
The non-headache symptoms of various migraine phases are non-specific resulting in difficulty for patients and clinicians alike to distinguish what is or is not related to migraine. 4 These symptoms often do not have dedicated interventions, and it is only recently that non-headache symptoms have become the focus of outcomes in treatment trials. Recognizing this, it is important to understand the non-headache symptoms of the various phases of migraine so that we can elucidate ways to intervene. Having objective measures to help identify when someone is in or going into a migraine attack is important for treatment planning.
The King-Devick test is a timed rapid number naming task (RNNT) where participants read numbers on test cards from left to right as quickly as possible without making errors. We have previously described that the time to complete the RNNT with zero errors was 4.6 s slower during migraine headache compared to interictal baselines (p < 0.001); with more prominent slowing of RNNT times during migraine headache in those with migraine with aura compared to individuals with migraine without aura (median 7.5 vs 2.8 s, p = 0.028). 6
The objective of this study was to determine whether there is a difference in the time to complete the RNNT with zero errors during the interictal phase compared to prodrome phase, postdrome phase, and non-migraine headache attack in addition to the previously noted differences between the interictal and migraine headache phase in patients with migraine with aura and migraine without aura. Additionally, non-headache symptoms experienced during these different phases will be characterized and compared.
Method
The study was approved by the Mayo Clinic Institutional Review Board (18-004102) and all participants provided informed written consent. This study is reported in accordance with the STROBE guidelines for observational study.
Study participants
This prospective longitudinal cohort study enrolled and collected data from 30 adults with migraine with or without aura from a tertiary headache center at Mayo Clinic Arizona from October 2020 through July 2022. Participants were enrolled if they were 18 years of age or older, diagnosed with migraine with or without aura per International Classification of Headache Disorders 3rd edition (ICHD-3), 7 reported experiencing 4–10 migraine attacks per month and having fewer than 15 headache days per month (average over the prior three months by self-report), and willing to provide RNNT and headache diary entries 3 times per day minimum. Given literature demonstrating changes in RNNT scores with various other conditions,8–13 participants were excluded if they had significant pre-existing ocular conditions, other neurologic diseases, history of intracranial surgery, or history of concussion within the past two years.
Study design and data collection
At the time of enrollment, detailed demographics (such as age, sex, gender, race, ethnicity), baseline headache characteristics (such as headache frequency, duration, location, quality, intensity; associated symptoms; history of aura; number of years with migraine; history of prodrome or postdrome symptoms; current preventive and acute therapies), Migraine-Specific Cognitive scores, and Utah Photophobia Symptom Impact Scale scores were recorded for each participant. For documenting baseline history of prodrome or postdrome symptoms, participants were asked on intake questionnaires: “Do you get premonitory/prodrome symptoms (i.e. symptoms before headache)?” and “Do you have postdrome symptoms (i.e. symptoms after headache is over)?.”
Each participant was given a tablet containing: (1) the RNNT application that allowed for self-administration of the RNNT via voice recognition with the time required to complete each test card, the number of errors and the number of trials to complete the test cards with zero errors being recorded; (2) the Symptom Diary through a Redcap weblink to record detailed clinical symptoms.
To self-administer the RNNT, participants would open the application on the tablet provided. The application provided written instructions which advised them not to block the tablet microphone and to speak naturally and clearly in an environment with minimal noise. Participants were instructed to position the screen at their normal reading distance and wear corrective lenses if normally used to read. Instructions advised that they would be timed reading a series of numbers aloud as quickly as they could without making any errors. A demonstration card was provided to allow participants to become familiar with the testing process with starting at the top and reading aloud from left to right. Participants were instructed not to use their hand or finger to follow the numbers. Timing started once test cards were displayed and ended upon them tapping the screen after calling out the last number on the test card. There were three test cards. There were break cards between each test card. After completion of the test, the application would tabulate whether any errors were recorded. An automated speech recognition system was built into the application, and the test recording was available for playback to participants. If errors were detected, the participant was instructed to review the audio playback to confirm results. There was also a visual summary of the results that showed the expected numbers in blue, correct numbers in green, incorrect numbers in red, missing numbers in red and corrected numbers in yellow. A corrected number meant that the participant initially misread the number but immediately corrected themselves. If actual errors were confirmed, the application prompted a re-test error-free. If there were no errors, the participant saved the test session and closed the application to proceed to completing their symptom diary entry.
Each participant was instructed to record a minimum of three RNNT and Symptom Diary entries per day in the morning (∼8 AM), mid-day (∼ 2 PM), in the evening (∼8PM), and additionally if there was an impending migraine attack or migraine attacks outside of these windows. These daily recordings were completed for up to four months to ensure at least eight migraine attacks were recorded. Each participant data entry included: (1) RNNT scores, comprised of time with zero errors, time of the first trial, number of errors of the first trial, number of trials to zero errors, and (2) Symptom Diary data, included subjective state of health—current state of health with five option rating from exceedingly poor to exceedingly good, menstruation status, sleep related information such as subjective quality of sleep with five option rating from exceedingly poor to exceedingly good, bed time, wake time, hours of sleep, and whether the participant experienced headache in the evening or overnight prior to that data entry; headache state—including subjective determination of the presence of migraine or non-migraine headache, and detailed symptom questionnaire, including but not limited to symptoms such as photophobia, phonophobia, neck stiffness, and fatigue, at each of the migraine phases—non-migraine headache phase, prodrome, migraine headache phase, and postdrome phase. Determination of state/phase was subjective. Participants were asked: “Do you have a headache?.” If yes, they were asked “Is it a migraine?.” If no, they were asked “Indicate your current state:” with the following options “Feeling a migraine coming on,” “Recovering from a migraine,” “Do not feel a migraine coming on.” If they indicated that they were having a headache but that it was not a migraine that was equivalent to a non-migraine headache state. If they indicated, they were having a headache and it was a migraine that was equivalent to a migraine headache state. If they indicated “Feeling a migraine coming on” that was equivalent to prodrome state, “Recovering from a migraine” was equivalent to postdrome state, and “Do not feel a migraine coming on” was equivalent to interictal baseline state.
All data collected were stored in a Redcap database at Mayo Clinic.
Statistical analysis
A sample of 25 participants with an estimated eight migraine attacks per participant would provide 80% power to detect an effect size of 0.25 or greater in RNNT score between time points with a significance level of 0.05. Thirty participants were included to account for drop-out. Descriptive statistics were used to summarize participants’ demographics, migraine characteristics including phase symptoms and treatments, median and ranges were used for continuous while counts and percentages were used for categorical characteristics. Differences between participants with a history of migraine with and without aura along with differences between interictal and migraine headache were compared using Chi-square test for categorical and Mann–Whitney U-test for continuous. Self-reported history of prodrome and postdrome phases at baseline and diary entry reports of prodrome and postdrome phases were compared using Cohen's kappa agreement, the Cohen's kappa agreement was reported along with the 95% confidence interval. Median RNNT scores were compared across the different phases. Paired differences were compared using Wilcoxon signed-rank test. All statistical tests were two-sided and p-values <0.05 were considered statistically significant. All statistical analyses were performed in R version 4.2.2.
Results
Demographics
Participant demographics are described in Table 1. Among the 30 participants enrolled, the average age was 44.6 (range 23.0–65.0), 29 (96.7%) were female, 27 (90%) were White, 2 (6.7%) were Asian, 1 (3.3%) was American Indian, 4 (13.3%) were Hispanic, and 26 (86.7%) were non-Hispanic. The mean duration of having migraine was 25.5 years, and the median days of headache and migraine days per month (28 days) was 10.0 (Q1, Q3 6.5, 13.8) and 7.0 (Q1, Q3 4.3, 8.0) days, respectively. Half of the participants had a history of migraine with aura (15/30 (50%)) with visual symptoms being most reported (14/15 (93.3%)). Participants reported taking acute treatments a median of 6.5 (Q1, Q3 4, 9.8) days per month. The top three most reported types of acute treatments included NSAIDS (18/29 (62.1%)), triptans (13/29 (44.8%)), calcitonin gene-related peptide (CGRP) small molecule receptor antagonists (9/29 (31.0%)). Twenty (66.7%) participants were on preventive treatments, with the majority utilizing multiple simultaneous preventive therapies (14/20 (70.0%)). The top three most reported preventive treatments included CGRP monoclonal antibodies (10/20 (50%)), Onabotulinumtoxin A (7/20 (35%)), and nutraceuticals (8/20 (40%)). Twenty-nine participants completed the study. One participant enrolled and completed a few days of the study and then contacted the study coordinators to discontinue study participation due to lack of time.
Participant demographics, migraine characteristics, and treatments.

Self-reported versus diary recorded prodrome/postdrome state
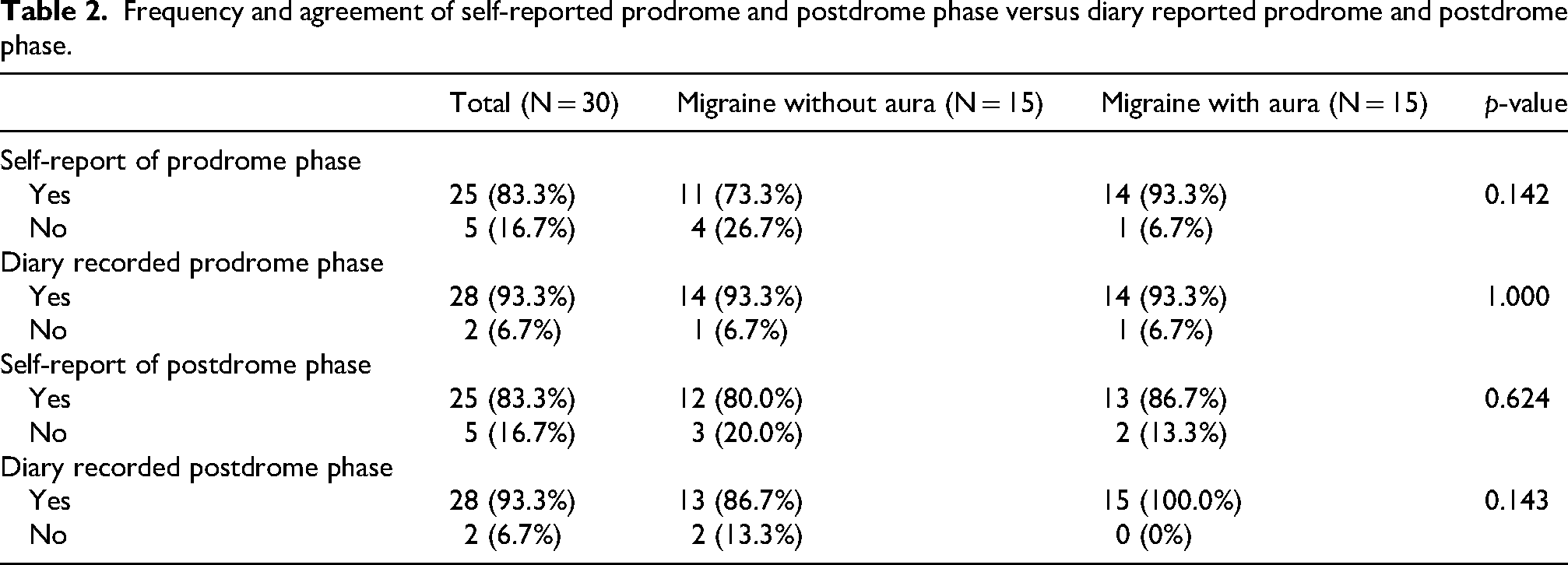
Among the study participants, at baseline 25 (83.3%) reported experiencing a prodrome state. However, with diary recordings 28 (93%) documented a prodrome state. This was the same for the postdrome state, with 25 (83.3%) reported at baseline and 28 (93%) documented by diary (Table 2). Given this, the Cohen's kappa agreement between self-report of history of prodrome state versus diary recordings showed moderate agreement (k: 0.53 95% CI (0.08, 0.97), p = 0.001) and the Cohen's kappa agreement between self-report of history of postdrome state versus diary recordings showed poor agreement (k: −0.11 95% CI (−0.22, 0.006), p = 0.51).
Frequency and agreement of self-reported prodrome and postdrome phase versus diary reported prodrome and postdrome phase.
Migraine versus non-migraine headache
Twenty-four participants (80%) reported by diary a non-migraine headache state at some point during the study period. Participants self-identified their state as migraine versus non-migraine headache with a sensitivity of 76.0% and specificity of 84.5% when comparing against ICHD-3 criteria (Table 3). When comparing non-headache symptoms that are included in the ICHD-3 criteria for migraine, photophobia was reported in 342/518 (66.0%) diary entries self-assigned as migraine phase among 28 participants compared to 79/289 (27.3%) diary entries self-assigned as non-migraine headache among 14 participants (p-value <0.001). Phonophobia was reported in 234/518 (45.2%) of diary entries self-assigned as migraine phase among 22 participants compared to 31/289 (10.7%) of diary entries self-assigned as non-migraine headache among eight participants (p-value <0.001). Nausea was reported among 224/518 (43.2%) of diary entries self-assigned as migraine phase among 24 participants compared to 26/289 (9.0%) of diary entries self-assigned as non-migraine headache among nine participants (p-value <0.001). Vomiting was reported among 17/518 (3.3%) of diary entries self-assigned as migraine phase among six participants compared to 1/289 (0.3%) of diary entries assigned as non-migraine headache phase among one participant (p-value 0.007).
Accuracy of participant reported migraine headache versus ICHD-3 diagnostic criteria.

Non-headache symptoms by phase
Table 4 outlines the frequencies of 32 different non-headache symptoms reported during migraine headache, non-migraine headache, prodrome, and postdrome phases. Photophobia, neck stiffness, and fatigue were among the three most common symptoms reported in all phases (Table 5). In the non-migraine headache phase, the three most common symptoms were tired/weary/fatigue /loss of energy (121/289; 41.9%), neck stiffness (85/289; 29.4%), and light sensitivity (79/289; 27.3%). In the migraine headache phase, the three most common symptoms were light sensitivity (342/518; 66.0%), tired/weary/fatigue /loss of energy (324/518; 62.5%), and neck stiffness (320/518; 61.8%). In the prodrome phase, the three most common symptoms were tired/weary/fatigue /loss of energy (89/181; 49.2%), neck stiffness (82/181; 45.3%), and light sensitivity (73/181; 40.3%). In the postdrome phase, the three most common symptoms were tired/weary/fatigue /loss of energy (166/290; 57.2%), light sensitivity (97/290; 33.4%), and neck stiffness (89/290; 30.7%).
Frequency of non-headache symptoms reported during various phases including migraine headache, non-migraine headache, prodrome, and postdrome phases among 30 adults with migraine with and without aura.

Rank list of most reported non-headache symptom by phase.

RNNT scores by phase
RNNT scores for the overall cohort were significantly slower during prodrome, migraine headache, and postdrome phases of migraine attacks and non-migraine headache attacks compared to the interictal baseline (Table 6 and Figure 1). The slowest changes were observed during the migraine headache phase (median 3.8 s slower, p < 0.001) compared to interictal baseline. For those with migraine with aura, RNNT score was also significantly slower during prodrome, migraine headache, and postdrome phases of migraine attacks and non-migraine headache attacks compared to interictal phase (Table 6). The slowest changes were also observed during the migraine headache phase (median 4.1 s slower, p < 0.001) compared to interictal baseline. For those with migraine without aura, RNNT score was significantly slower during migraine headache (median 3.8 s slower, p < 0.001), but not other phases compared to interictal phase (Table 6). RNNT slowing was significantly more prominent during self-reported migraine headache than non-migraine headache attacks in the overall group, migraine with aura, and migraine without aura groups (Table 7).

Median difference in rapid number naming task time with zero errors for prodrome, migraine headache, postdrome, and non-migraine headache in comparison to interictal baseline for overall participants and for participants with or without history of aura.
Comparison of rapid number naming task time with zero errors by phase.

Comparison of rapid number naming task score difference between migraine and non-migraine headache.

Discussion
As per our pilot study findings, RNNT scores were slower during the migraine phase compared to the interictal phase for the overall cohort as well as in the migraine with or without aura cohorts. Notably, the RNNT scores were significantly slower across all phases of the migraine attack for participants with migraine with aura but only significantly slower during the migraine headache phase for participants with migraine without aura. This builds upon our pilot study results of more prominent slowing of RNNT times during migraine headache in those with migraine with aura compared to individuals with migraine without aura (median 7.5 vs 2.8 s, p = 0.028). 6 This also suggests that even when aura symptoms are not actively happening there are changes in cerebral functioning of people with migraine with aura that can manifest as changes in objective tests such as RNNT. Furthermore, when comparing migraine headache versus non-migraine headache attacks, we also found that the RNNT score was significantly slower during migraine headache, providing objective evidence that more prominent cerebral function changes occurred during a migraine attack that goes beyond the level of head pain.
Prodrome and postdrome phases were common among participants as is described in the literature. The most common symptoms reported in the prodrome state of our study were consistent with the symptoms reported in recent literature, such as the PRODROME trial, and we additionally provided the most common symptoms during the postdrome, and non-migraine headache phase.4,14 A subset of participants initially reported that they did not have prodrome (N = 3) or postdrome (N = 3) phases but with diary recording did. This speaks to the importance of educating patients about these phases so that they can accurately attribute their symptoms to migraine. Numerous non-headache symptoms were reported across all phases of migraine and during non-migraine headache attacks. The most reported symptoms included fatigue, photophobia, and neck stiffness. When considering the migraine headache phase, it is not surprising that the most reported non-headache symptom was photophobia (66.0% of diary entries among 28/30 participants) given that it is part of the diagnostic criteria. However, the second and third most reported symptoms during migraine headache were non-specific, fatigue (62.5% of diary entries among 27/30 participants), and neck stiffness (61.8% of diary entries among 27/30 participants). These symptoms were among the top five symptoms reported in non-migraine headache, prodrome, and postdrome. Besides photophobia, the other ICHD-3 non-headache symptom criteria for migraine were reported as follows: phonophobia (45.2% of diary entries among 22/30 participants), nausea (43.2% of diary entries among 24/30 participants), and vomiting (3.3% of diary entries among 6/30 participants). The discrepancy in frequency of symptoms that we use for diagnosis and symptoms that are commonly reported illustrates the importance of reconsidering our approach to clinical trial outcomes and the importance of patient-reported outcomes that allow for identification of most bothersome non-headache symptoms whether included in the diagnostic criteria or not.
The strengths of our study include the detailed and longitudinal recording of clinical symptoms and RNNT from each participant three times a day for up to four months, with at least eight migraine attacks recorded, allowing a large amount of data to characterize migraine phase-specific subjective and objective changes. Given the real-time recording of symptoms, recall bias is minimized. This may explain the difference in frequency of reported prodromal symptoms in this study compared to the recent study by Lipton et al. which based prodromal symptom reports on interview rather than diary data. 14 Although there were only 30 participants, each participant provided very detailed data totaling 4983 records, including symptom descriptions and RNNT scores, thus allowing for thorough description of their migraine experience through all phases for each individual. This study provides detailed information about frequency of symptoms but cannot comment on what participants may have found most bothersome among their symptoms. The limitations of the current study include a small sample size of 30 participants, which may affect generalizability. Inclusion criteria required participants to have fewer than 14 headache days per month (i.e. episodic migraine). However, based on the preventive treatments that the participants were on, such as Onabotulinumtoxin A, technically some of them would have had chronic migraine diagnoses and their treatments reduced their headaches to an episodic frequency. As such, it is hard to know if these results can be generalized to chronic migraine populations or not. It raises the question of whether someone who has a diagnosis of chronic migraine but is now in an episodic pattern on preventive treatment would have phase symptoms and RNNT scores more like someone with untreated chronic migraine or more like someone with untreated episodic migraine. Phase state, such as reporting being in a migraine headache versus a non-migraine headache, was self-reported. However, when comparing self-reported headache state with ICHD-3 criteria based on symptoms recorded during attack, participants identified their state as migraine versus non-migraine headache with a sensitivity of 76.0% and specificity of 84.5%. As such, patient self-report appears to be a reliable indicator of migraine state. Our pairwise non-parametric approach focuses on marginal, per-contrast differences on aggregating participant level data and does not take within-subject correlation and unbalanced observations into account. Mixed-effects model would address these features more comprehensively; we plan to explore them in future extension.
Conclusions
Our study shows significant changes in the RNNT score during different phases of migraine and non-migraine headache attacks compared to the interictal phase, especially among participants with migraine with aura. This study highlights that cerebral function changes could be detected starting in the prodrome phase and continue throughout the migraine headache and postdrome phases. Additionally, we provided the non-headache symptoms patients reported across the prodrome, non-migraine headache, migraine headache, and postdrome phase, with photophobia, fatigue, and neck stiffness being the most common symptoms reported across all phases. Our data suggests a potential role for objective, real-time, self-administered tools, like RNNT used in the current study, in association with detailed symptom description to quantitatively assess patient state during different phases of migraine and possibly distinguish migraine from non-migraine headache.
Article highlights
In the overall study cohort and those with migraine with aura, the rapid number naming task was significantly slower during all phases compared to the interictal phase but only during the migraine headache versus interictal phase in those with migraine without aura.
The top 5 most reported non-headache symptoms during any phase of migraine and non-migraine headache included fatigue, neck stiffness, light sensitivity, vision changes, and difficulty concentrating.
Footnotes
Abbreviations
Acknowledgements
The authors would like to acknowledge the help of Nan Zhang MS who contributed statistical support during the manuscript review process.
Ethical considerations
The study was approved by the Mayo Clinic Institutional Review Board (18-004102).
Consent to participate
All participants provided informed written consent.
Consent for publishing
All authors have reviewed the manuscript and agreed to publish the article with Cephalalgia Reports.
Author contributions
Conceptualization: VanderPluym, Starling, Chiang. Data curation: VanderPluym, Patel. Formal analysis: VanderPluym, Girardo. Funding acquisition: VanderPluym. Investigation: VanderPluym, Patel, Starling, Chiang. Methodology: VanderPluym, Starling, Chiang. Project administration: VanderPluym. Resources: VanderPluym. Software: VanderPluym, Starling, Chiang. Supervision: VanderPluym. Validation: VanderPluym, Starling, Chiang, Patel, Girardo. Visualization: VanderPluym, Chiang, Girardo. Writing—original draft: VanderPluym, Chiang. Writing—review & editing: VanderPluym, Patel, Starling, Girardo, Chiang.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a Competitive Science Grant from Amgen. The Competitive Grant Program provides investigators and scientists with the opportunity for independent research into mechanisms and impact of specific diseases. This is not an Investigator Sponsored Study (ISS). The tablets (iPad) and King-Devick Home Monitoring app were provided by King-Devick technologies, Inc.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J. VanderPluym reports research support from Patient-Centered Outcomes Research Institute (MI-2023C2-33021) and State of Arizona (RFGA2023-008-26). She received Honoria from BMJ (for authorship and editing). She acts as Current Neurology and Neuroscience Reports, Headache Section Co-editor. A.J. Starling has received consulting fees from AbbVie, Allergan, Amgen, Amneal, Axsome Therapeutics, Eli Lilly, eNeura, Everyday Health, Impel, Lundbeck, MedIQ, Medscape, Miller Medical, Neurolief, Novartis, Pfizer, Salvia, Satsuma, Teva, Theranica, UpToDate, WebMD, and Woodberry Associates. C. Chiang has served as a consultant for Pfizer, AbbVie, Amneal, Satsuma and eNeura. She receives research support from the American Heart Association, Lundbeck and Pfizer with funds paid to her institution. R. Patel report no disclosures. M. Girardo report no disclosures.
Data availability statement
Identifiable individual-level data cannot be shared due to patient confidentiality. Aggregate-level data may be made available from the corresponding author upon reasonable request.