
Abstract
Objective
To collect pairs of nonfactual information and their interpretations and rate their usefulness in distinguishing between primary and secondary headache disorders.
Background
Physicians use clinical indicators such as Red Flags and ask about exposure to potential causes to differentiate primary from secondary headaches; however, these approaches have limitations and may result in unnecessary diagnostic procedures.
Methods
Using the Delphi process, the participants proposed information-interpretation pairs in the first round and rated them anonymously in two subsequent rounds. The ratings relied on quality estimators to evaluate the reliability, validity, relevance, and frequency on 5-point Likert scales, ranging from 0 to 5. We considered pairs with an average rating of 4.0 or higher to have reached consensus.
Results
Four proposals reached consensus, of which two referred to nonfactual information: (i) “A headache that feels familiar indicates a primary headache.” (ii) “A headache that feels completely different from any previous headache raises the suspicion of a secondary headache.”
Conclusions
The participants generally found little use for nonfactual information for distinguishing between primary and secondary headache disorders. Solely the presence and absence of patients’ notion of a familiar headache were deemed helpful. While the participants viewed the former as being associated with a primary headache, they felt that the latter pointed towards a secondary headache. Further research is necessary to evaluate their usefulness in clinical practice.
Introduction
Physicians take different steps to distinguish primary and secondary headaches. One is to ask about exposure to a known cause of secondary headaches, such as larger quantities of alcohol or trauma. 1 In addition, they assess the phenotype and examine the patients to search for symptoms and signs that are nontypical for primary headaches, known as Red Flags.2,3 Then, they query if the patient has risk factors for developing a disorder associated with secondary headaches; an example is pregnancy, which predisposes to sinus thrombosis. 2 Finally, evaluating the presence of Green Flags, which indicate an increased probability of having a primary headache, has recently received some attention. 4
Although the sensitivity of commonly used Red Flags is very high,5,6 they still cannot guarantee detection of every secondary headache at every stage of the underlying disorder. As a consequence clinicians may, out of concern for missing a potentially serious case, oversuspect secondary headaches, which can lead to additional—and sometimes unnecessary—investigations such as neuroimaging or lumbar puncture. 7
Besides, even when collecting data attentively, random errors can still occur. One way to mitigate their influence on data quality is by repeating the information collection. 8 For example, one could reiterate important questions or rephrase them when unsure if the patient understood them correctly. In addition, one could also tap further information resources, which is the topic of this study.
While observing, examining, and taking a history from their patients, physicians also collect information beneath the factual layer, so-called nonfactual information, which can be transmitted verbally and nonverbally.9,10 They comprise patients’ and physicians’ interpretations of what is seen and heard, as well as feelings and intuitions.
The diagnostic value of these pieces of information is largely unknown, and it is not always obvious how to use them for diagnostic purposes. Using the Delphi method,11,12 this study investigates whether nonfactual information holds any value in its participants’ perceptions for distinguishing between primary and secondary headache disorders.
Methods
Study design
This study collected and then rated information potentially helpful for classifying headache disorders through the classic Delphi process between March and June 2025.11,12 All participants contributed anonymously, and each contribution had equal weight.
In the first round, participants listed pieces of information that fell into one of the categories detailed below (opinion, feelings, relationship, intentions, and appearance) and their significance.
In the second round, all participants reviewed and rated the proposals using predefined quality indicators. In the third round, the participants reviewed the proposals again, this time along with the ratings they had received in the second round (reported as means and standard deviations). Bearing these ratings in mind, the participants then re-rated the proposals using the same assessment criteria.
No consulting regarding method took place.
Participants
The members of the Secondary Headache Special Interest Group of the International Headache Society were eligible to participate.
Nonfactual information
The participants were invited to contribute nonfactual information along with its diagnostic significance that falls into the following categories.
Patients’ interpretation of or opinion regarding their symptoms: For example, physicians may ask, “Does your headache feel familiar”? Patients’ feelings about the symptoms they report: For example, they might reveal their fear of “something serious,” or they might seem emotionless and disconnected. Patients’ relationship in which they see themselves with their physician: For instance, they might expect the physician to know how to treat the pain, but they might also be hostile, accusatory, or clingy. Patients’ intentions: For example, they might want a remedy for the pain, a certificate of incapacity for work, or relief from their fear. Patients’ appearance, which, beyond revealing their feelings, may indicate, for example, ill health through pallor and exhaustion.
Quality indicators
Participants rated the quality of the proposals based on clinical experience using the following indicators. Their purpose is to estimate the reliability, validity, relevance, and frequency of the piece of information. For each piece of information, the participants indicated their agreement with the following sentences on a 5-point Likert scale (“strongly disagree,” “somewhat disagree,” “neither agree nor disagree,” “somewhat agree,” “strongly agree”).
Inter-rater reliability: “Different physicians assessing the presence of the information would come to the same conclusion.” Retest reliability: “Physicians can assess the information at any time of the emergency visit, and the result would remain the same.” Face validity: “The proposed interpretation of the piece of information is justified.” Relevance: “The collected information is relevant for the diagnostic process.” Frequency: “The piece of information is encountered in many patients presenting with acute headaches.”
Consensus criterion
To compare the ratings of the proposals, we calculated a total score by averaging the mean scores of individual quality indicators, assigning equal weight to each indicator. We considered proposals with a total average score of 4.0 and above as meeting the consensus criterion.
Statistical analysis
In this primary analysis of the collected data, we treated scores of the quality indicators as continuous variables and then described them as means and standard deviations. We determined the total score for each quality indicator in the second and third rounds by calculating the mean and standard deviation of all votes cast for each proposal. The statistical analysis was conducted at the University Hospital Zurich using IBM SPSS 29.0.0.0. The available data determined the sample size.
Ethical statement
In every round, everybody provided informed consent before participating. As we collected strictly anonymous data, and only group members participated, ethics committee approval was deemed unnecessary.
Results
Twenty experts were invited to participate. In the first round, 15 participants (response rate 15/20, 75%) proposed 39 pieces of information (see Table 1), which entered the second round. There were seven proposals (7/39, 17.9%) for category A (interpretation or opinion), eight (8/39, 20.5%) for Category B (feelings), four (4/39, 10.3%) for category C (relationship), six (6/39, 15.4%) for category D (intentions), and 14 proposals (14/39, 35.9%) for category E (appearance).
Results of the first round of the Delphi process.

In the second round, 12 participants (response rate 12/20, 60.0%) rated the proposals. Four pieces of information with their interpretations (4/39, 10.3%) reached consensus (see Table 2) of which three fell into the category “Patients’ interpretation of or opinion” (proposals numbers 2, 4, and 7), and one into the category “Patients’ appearance” (proposal number 34). The average ratings of proposals in category A were 3.77 ± 1.22, in category B 3.06 ± 1.22, in category C 3.04 ± 1.11, in category D 3.37 ± 1.18, and in category E 3.60 ± 1.19.
Results of the second and third round of the Delphi process; the five rows correspond to the five quality indicators defined for this study, the values in the cells represent the average ratings (± standard deviation) of all participants; the overall score was obtained by calculating the mean of all average ratings of every individual quality indicator.
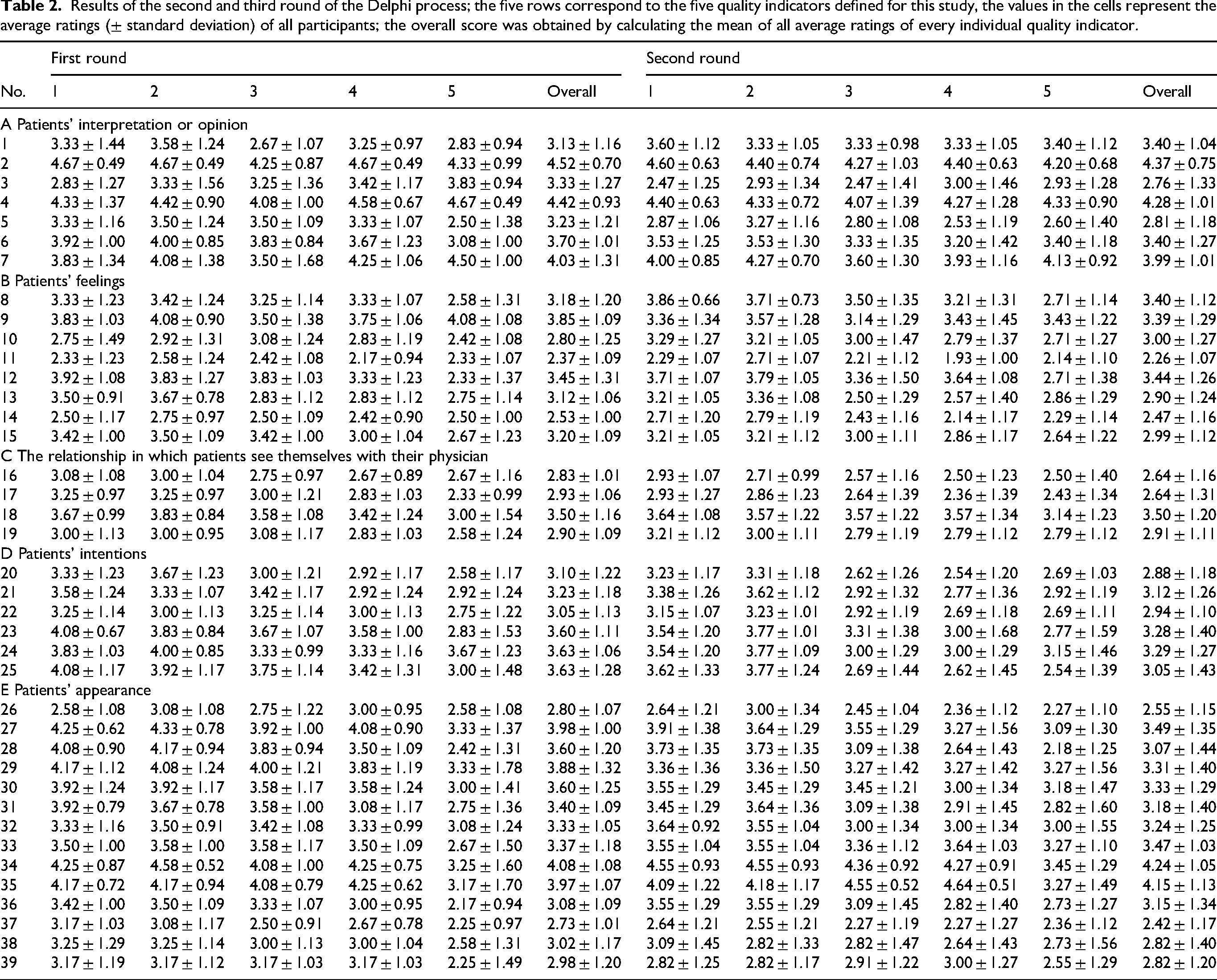
Fifteen participants responded to the third round, yielding a response rate of 75% (15/20). Three of the four proposals that reached consensus level in Round 2 (see Table 3) also achieved this in Round 3. However, the rating of proposal 7 dropped below the consensus level, while the average rating of proposal 35 was now above the threshold. The average rating of proposals in category A were 3.57 ± 1.25, 2.98 ± 1.26 in category B, 2.93 ± 1.24 in category C, 3.09 ± 1.28 in category D, and 3.23 ± 1.35 in category E.
Proposals that reached consensus level in the third round.

Discussion
This study used the Delphi method to analyze the value of nonfactual information—for example, emotional, relational, and motivational content implicitly embedded in communication—in distinguishing between primary and secondary headache disorders. Of the proposals that reached consensus, two centered on the same idea—the familiarity of a headache—, and two did not refer to nonfactual information but to findings of the physical examination (see below). Consequently, the participants generally found little use for the type of information analyzed in this study.
In Rounds 2 and 3, category A, “patients’ interpretation of or opinion regarding their symptoms,” received the highest average ratings, and two of the proposals that reached consensus level in the third round fell into this category. Conceptually, the underlying idea is that patients have an intuition that complements the information that physicians usually collect.
This relatively high appraisal of the type of information corroborates previous data: different studies have shown that primary care physicians also find considerable value in patients’ intuitions in the decision-making process.13–16 Thus, in this category may lie the additional information source that the study hoped to see, and future research could investigate.
Interestingly, participants distinguished patients’ interpretations and intuitions (category A) from their feelings (category B), which received lower ratings. So, in the view of the participants, neither does fear indicate a severe underlying disorder nor does being calm argue against a secondary headache. Instead, patients’ “gut feelings” must provide new information to be helpful. A possible reason is that worrying easily is a personality trait known as neuroticism, which, although common among migraineurs, does not occur in the context of a disorder but independently. 17
The categories C, D, and, most evidently, E assessed the physician's views and intuitions, instead of the patients’ views and intuitions. They received low ratings, except for the category E “appearance.” There, the participants seemed to distinguish between transient, situational features such as unwashed hair or clothes (item 26), sunglasses (item 27), or a facial expression that did not match the reported level of pain (item 29), and (2) more stable physical characteristics such as obesity (item 34), enlarged masseter muscles (item 33), or dull facial features (item 39). The latter features reached higher scores, but here, the participants’ struggle to distinguish between factual and nonfactual information became most evident.
Several of the proposals made to category E significantly overlap with the physical examination, which also comprises the inspection of the patient. In particular, the two proposals that reached consensus level—obesity and swelling of temporal arteries—could well be categorized as “factual.” While the clinical value of recognizing obesity18,19 and swelling of temporal arteries 20 is well-established, these findings are not the topic of this Delphi study. Ideally, such items would have been excluded earlier; however, at study initiation, we defined no explicit for excluding first-round proposals. For this reason, all initial suggestions were carried forward to avoid subjective post hoc filtering.
Overall, if the participants had some reservations against giving too much weight to patients’ interpretations of their symptoms, they wholly opposed physicians trusting their gut feelings.
Useful information-interpretation pairs
A headache that feels familiar indicates a primary headache.
This information-interpretation pair is similar to the Green Flag, “The current headache has already been present during childhood,” published previously.
4
The central information is the sense of familiarity. This information-interpretation pair comprises several claims.
First claim: headaches with the same pathophysiology can feel familiar, while headache attacks with a different pathophysiology do not. Second claim: a headache that feels familiar has likely occurred in the past and has consistently exhibited an analogous pathophysiology and a recognizable phenotype. Third claim: having experienced a headache due to the exact underlying pathophysiology repeatedly implies that the symptoms of future attacks of that type will be similar; consequently, a secondary headache with grave consequences would not have remained undetected. Fourth claim: because primary headaches are more likely to recur than secondary headaches, a familiar headache is more likely to be a primary headache.
In our experience, physicians taking a headache history often ask whether an acute headache has occurred before, in particular, since many view this information as a Red Flag. 3 As a consequence, the participants likely have an intuitive understanding of the truth value of this claim. Nevertheless, many of the assumptions require further research.
While there is some evidence suggesting that a new onset, i.e., unfamiliar, headache has an increased risk of being secondary, 21 the predictive value of a sense of familiarity remains to be studied. Additionally, it is generally not possible to precisely trace the pathophysiology of a headache. Furthermore, repeated occurrence does not guarantee that all associated symptoms are already known, and that the headache is primary. For example, the ominous thunderclap headache can occur repeatedly before a major subarachnoid hemorrhage appears. 22
Given the uncertain truth of the underlying claims, the notion of familiarity can be no more than a supporting criterion for the hypothesis of recurring primary headaches. It cannot overrule Red Flags suggesting a secondary headache.
A headache that feels completely different from any previous headache raises the suspicion of a secondary headache.
This information-interpretation pair, similar to a Red Flag formulated in a previous article, 3 resembles the previous information-interpretation pair. The difference is that here, the claim is that a headache that does not feel familiar is likely to have a different pathophysiology than previous pain and, thus, has an increased risk of being secondary.
Although there is some evidence supporting that claim, 21 a strong caveat is that the absence of the notion of familiarity is a “Catchall Red Flag.” That means it does not suggest any specific underlying pathology and, thus, does not indicate where to look for the disorder causing the pain. 2
Furthermore, a new headache does not equal a secondary headache. In the neurological emergency department 23 and, in particular, in tertiary headache centers, 24 the pretest probability of encountering a primary headache is higher than that of encountering a secondary headache. Thus, future studies must analyze the predictive value of the notion of “unfamiliarity” in different settings.
Strengths, limitations, and future directions
The strength of this study lies in its combination of expertise from several headache specialists, shedding light on a concept that has received little scientific attention. Additionally, the method enabled the generation and testing of ideas without requiring the conduct of major clinical studies beforehand.
However, the latter strength is also a limitation, as the study collected opinions. Although all participants are experienced headache experts, their opinions and intuitions do not replace scientific evidence collected in clinical studies; this study intended to inspire future studies, not to replace them. In this context, it is essential to note that all participants primarily treat adult patients. The results of this Delphi study could have been very different if conducted among pediatricians.
With an average of less than two proposals per participant and some proposals not addressing nonfactual information (see above), in the first round, the participants struggled to contribute. Moreover, in the second and third rounds, most ratings exhibited a central tendency (i.e., they centered around the value 3), indicating that participants were uncertain about the value of the information-interpretation pairs. Reasons may be that they have attributed little importance to this type of information in the past, and that the concept was unfamiliar. Perhaps repeating the survey in the future would identify further useful information-interpretation pairs.
The quality indicators used in this study aimed to assess different aspects of the information-interpretation pairs. They were arbitrary to some degree; in particular, there is room for discussion about whether all of them should have the same weight. However, given the generally low standard deviation of the overall ratings, there is little reason to believe that different weights would have substantially changed the overall result.
This study aims to stimulate further research into secondary headache disorders. Although clinical history and patient examination frequently enable accurate diagnosis, it is also imperative to understand when these approaches can be insufficient at times. For such instances, we need sensitive and specific tests, potentially including biomarkers, that—when used in a targeted manner—allow for reliable diagnosis of patients’ headache disorders. Nonetheless, optimizing the collection and interpretation of clinical history remains fundamental, and further research should prioritize enhancing these methods to improve diagnostic accuracy.
Conclusion
The participants generally found limited use for nonfactual information for distinguishing between primary and secondary headache disorders. Nevertheless, patients’ interpretations of their feelings or intuitions received relatively high values. Within that category, the notion of a familiar or unfamiliar headache was deemed helpful: While the participants viewed the former as being associated with a primary headache, they felt that the latter pointed towards a secondary headache.
Further research is needed to determine the clinical utility of the information-interpretation pairs in the diagnostic process. Currently, it is imperative to bear two limitations in mind. First, the notion of familiarity cannot overrule established Red Flags; thus, it cannot be more than a supporting criterion. Second, while there may be a statistical association between an unfamiliar headache and a secondary headache, unfamiliarity does not necessarily indicate a specific secondary headache; as a result, an unfamiliar headache could prompt many unnecessary additional examinations.
Clinical implications
This study used a Delphi process to assess how nonfactual, intuitive information might aid in distinguishing between primary and secondary headache disorders.
Overall, experts found limited diagnostic value in such information. Thus, these impressions cannot replace established red flags.
The only nonfactual cues reaching consensus were patients’ impressions of a “familiar” versus “unfamiliar” headache. A familiar headache was considered suggestive of a primary headache, whereas an unfamiliar headache raised suspicion of a secondary headache.
Footnotes
ORCID iDs
Consent to participate
As we collected strictly anonymous data, and only group members participated, ethics committee approval was deemed unnecessary.
Consent for publishing
In every round, everybody provided informed consent before participating.
Author contributions
Heiko Pohl: Conceptualization; methodology; investigation; data curation; formal analysis; writing—original draft. All other authors: Investigation; writing—review & editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data used for this article may be obtained from the authors with a reasonable request.