
Abstract
Background
Migraine headaches in the Caribbean region, despite being a debilitating illness impacting quality of life and inherently disability adjusted life years has not been given the emphasis it deserves. Migraine has a significant and rising neurologic burden internationally. Yet as advancements are being made, the Caribbean region is falling behind. This paper attempts to bridge that gap by gathering statistical evidence, not just of the prevalence of migraine headaches, but also of the scope of practice surrounding migraine headaches within the English speaking Caribbean. The primary objective is to assess existing healthcare infrastructure, aiming to identify critical gaps, subsequently proposing areas for improvement, to ultimately enhance care for individuals across the diverse Caribbean diaspora.
Methods
A descriptive, cross sectional survey was conducted over the period July to August 2025 among Neurologists across seven English speaking Caribbean territories. The questionnaire assessed specialist availability, diagnostic tools, access to therapies, non-pharmacologic interventions, barriers to care, and educational initiatives. Ethical approval was not required due to the design of the study, and the CARE guidelines were adhered to throughout. Responses reflected perceived availability rather than audited formularies. Data were analysed descriptively. No patient data were collected, ethical approval was not required, and participation was voluntary and uncompensated.
Results
Caribbean territories, including Trinidad, Barbados, and Jamaica, demonstrated comparatively broader therapeutic availability, while smaller nations such as Antigua, St Vincent, Guyana, and St Lucia reported markedly restricted options. Acute management remains largely reliant on older, non-specific agents, with limited access to triptans and an almost complete absence of neuromodulation or novel migraine specific therapies. This heterogeneity in therapeutic access reflects systemic disparities in headache care across the region.
Conclusion
The Caribbean diaspora is a multi-cultural and highly diverse group, which unfortunately has previously been under-represented in worldwide studies on migraine treatment and management, meaning that the care afforded to patients has often been limited. This paper has identified several key gaps, that once addressed, should significantly improve the standard of care for migraine headaches in the region, thereby improving the quality of life of patients, and by extension, mitigating it's downstream socio-economic consequences.
This is a visual representation of the abstract.
Introduction
The International Classification of Headache Disorders, 3rd edition describes migraine as a primary headache disorder with attacks lasting 4–72 h and typical characteristics being unilateral location, pulsating quality, moderate or severe intensity, aggravation by routine physical activity and association with nausea and/or photophobia and phonophobia. 1
The Global Burden of Disease (GBD) study 2021 demonstrates that migraine is within the top 20 causes of disability-adjusted life years (DALYs), but fourth among young adults and third among young females.2,3 Pacheco-Barrios et al., 4 in their 2023 meta-analysis of population based studies, concluded that primary headaches were of a higher prevalence in Latin American countries (LAC) and the Caribbean as compared to other systematic global and regional estimations; they reported a pooled frequency of 15.0% for migraine (12.0–18.3, 95% CI). This is mirrored in the GBD data, which shows upward trends in estimated annual prevalence changes for Latin America, of 0.28 for prevalence and 0.26 for DALYs. Again, though this data is lacking for the Caribbean region, analysis of DALYs against the socio-demographic Index (SDI) shows that specific to the medium and low to medium SDI populations (of which the Caribbean islands are included) there is a large number of people who experience migraine, and the resulting disease burden is considerable. 5
Migraine often goes undiagnosed and undertreated, an issue which disproportionately affects low-to-middle-income countries (LMICs), where there is a paucity of education, research and resources dedicated to investigation and management of this headache disorder. 6
In LMICs this disparity is multi-faceted; as both the recognition and management of migraine are limited due to an already overburdened healthcare infrastructure, working with limited economic resources, and a paucity of specialized clinics with qualified specialists. The superimposition of cultural beliefs and misconceptions only serves to make this more challenging. 7
Much research has been conducted into the pathophysiology of migraine, 7 and knowledge of its complex biology have led to the development and use of targeted therapies such as calcitonin gene-related peptide (CGRP) monoclonal antibodies & receptor antagonists and serotonin 5HT1F receptor agonists.7,8 These novel migraine treatments are not widely available, and it has been postulated that their high cost renders reimbursement extremely unlikely across most Caribbean healthcare systems. 9
The English-Speaking Caribbean represents a particularly understudied and under-resourced region. Many islands are understaffed, with few specialist neurologists managing a vast volume of patients. Healthcare infrastructure and resources are constrained, with limited diagnostic procedures, whilst national pharmaceutical formularies often include only low-cost medications without access to newer agents. To date, no multi-country study has examined migraine care across the region.
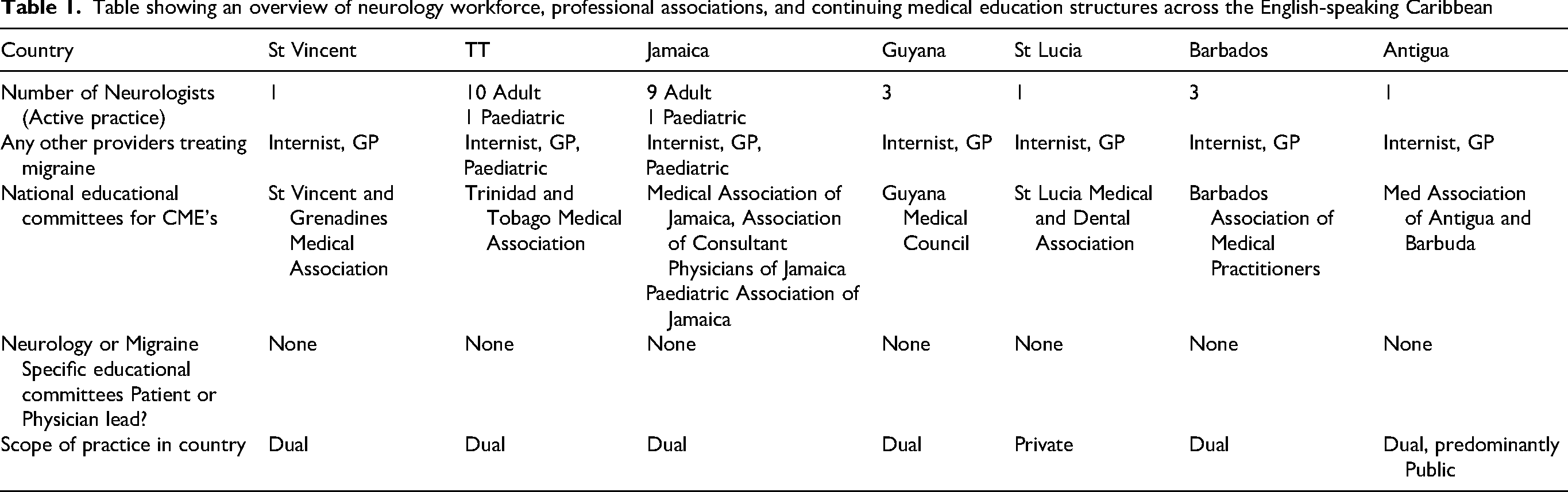
This study aims to provide a snapshot into current practices in the management of migraine in the English-Speaking Caribbean, a brief overview of which is included in Table 1. Neurologists across seven English-Speaking Caribbean islands were surveyed, and their subjective assessments on diagnostic and therapeutic practices, the availability of procedures and the barriers they faced were ascertained.
Table showing an overview of neurology workforce, professional associations, and continuing medical education structures across the English-speaking Caribbean
Methods
This was a descriptive, cross-sectional survey conducted between July–August 2025. Neurologists from seven English-Speaking Caribbean territories (Antigua, Barbados, Guyana, Jamaica, Trinidad and Tobago, St Lucia, St Vincent and the Grenadines) were invited to participate via completing the survey instrument. Each respondent was an actively practicing neurologist in their territory, and thus well poised to provide expert insight into the current practices of migraine management.
The survey instrument (Appendix 1) was developed for this study. Notably, one of the authors of this study (A.P.) was involved in the designing of the survey and was also the respondent for Trinidad and Tobago. The survey comprised both open- and closed-ended questions across a number of domains; (1) specialist availability and migraine caseload, (2) availability of diagnostic tools, (3) access to preventative/prophylactic pharmacotherapies, (4) access to abortive treatments, (5) availability and use of procedural or non-pharmacologic interventions, (6) perceived barriers to care and (7) available educational initiatives regarding migraine management. The survey instrument evaluated the respondents’ perception of availability; formularies were not objectively audited.
The completed questionnaires were analysed descriptively to provide an overview of migraine care in the English-Speaking Caribbean. No statistical tests were conducted given the small sample size.
This study did not utilise patient data nor were any personal data collected. Institutional review board approval was thus not required. Participation was voluntary. No compensation, whether financial or otherwise, was offered to respondents for viewing or completing the survey.
Results
Figure 1 is a stacked bar graph titled “Stacked Graph showing Variations in the Management of headaches in the English Speaking Caribbean.” It illustrated the availability and reported use of different therapeutic approaches for headache management across seven Caribbean countries. Trinidad (blue), Barbados (orange), Jamaica (gray), Antigua (yellow), St Vincent (light blue), Guyana (green), and St Lucia (dark blue). Each Vertical bar represents a specific treatment modality, and the height of the stacked bar (maximum 7) corresponds to the number of Countries that reported availability or use of that treatment. The therapeutic modalities examined included prophylactic agents, antiepileptic drugs (AEDs), antidepressants, supplements, injectable treatments, neuromodulation, novel therapies, and selected specialist interventions.

Stacked graph showing variations in the management of headaches in the English-speaking Caribbean.
Prophylactic agents such as propranolol and amitriptyline were widely available and consistently reported across nearly all countries, indicating reliance on older, well established therapies. Similarly, AEDS (particularly sodium valproate and topiramate) were present in most territories. Antidepressants showed a similar pattern, with duloxetine being the most ubiquitous agent, while nortriptyline, venlafaxine and mirtazapine demonstrated more limited distribution.
Marked variability was observed in the availability of supplements. Countries such as Trinidad and Barbados, reported broader access to riboflavin, magnesium, and coenzyme Q10, whereas other territories often lacked these options.
Both neuromodulation techniques, as well as injectable treatments viz nerve blocks and botulinum toxin injections were consistently not available, reflecting disparities in access to resource intensive interventions.
The most striking gap was observed in the domain of novel migraine specific therapies, particularly the CGRP monoclonal antibodies (erenumab, fremanezumab, galcanezumab and eptinezumab). Access to these treatments is entirely absent, with rimegepant the only drug amongst the new treatments reported as available in select nations. This highlights a significant unmet need when compared to international standards of care.
Specialist interventions such as onabotulinumtoxin A, intravenous dihydroergotamine, and non-pharmacological approaches including acupuncture and greater occipital nerve blocks were sporadically reported, again with wider representation in certain territories.
Overall, the data illustrates a clear gradient: Caribbean nations (such as Trinidad, Barbados, Guyana, and Jamaica) demonstrate a broader therapeutic range spanning traditional agents to some advanced modalities, while St Lucia and Antigua, report far narrower options. Despite existing international recommendations and regional policy discussions, uptake of advanced therapies remains extremely limited across the Caribbean, underscoring persistent inequities in migraine care.
Figure 2 is a stacked bar graph titled “stacked Graph showing Acute Treatments in the management of headaches in the English speaking Caribbean.” It illustrates the reported use of acute headache therapies across seven Caribbean countries. Trinidad (blue), Barbados (orange), Jamaica (gray), Antigua (yellow), St Vincent (light blue), Guyana (green) St Lucia (dark blue). Each vertical bar represents a specific acute treatment, while the height of the stacked bar (up to 7) indicates the number of countries in which that treatment is available.

Stacked graph showing acute treatments in the management of headaches in the English-speaking Caribbean.
Analgesia was universally reported, with widespread availability of paracetamol, ibuprofen, and naproxen across nearly all territories. Diclofenac was also commonly reported, while tolfenamic acid and ketoprofen were more restricted.
Antiemetics such as metoclopramide, chlorpromazine and prochlorperazine were widely available, reported across most territories. Domperidone, however was inconsistently represented, appearing in most countries but not Antigua.
Triptans demonstrated the greatest treatment disparity. Sumatriptan was most frequently available, reported primarily in Barbados, Jamaica, Antigua, St Vincent, Guyana and St Lucia, while other triptans (rizatriptan, naratriptan, zolmitriptan, and eletriptan) were almost completely absent across the region.
Neuromodulation therapies were entirely absent. These advance device based approaches such as non-invasive vagus nerve stimulation, transcranial magnetic stimulation, trigeminal nerve stimulation or remote electrical neuromodulation were not reported in any territory surveyed.
Novel treatments such as rimegepant and use of onabotulinumtoxin A/nerve blocks were reported amongst 5 different nations.
Trinidad, Barbados, and Jamaica demonstrated the broadest therapeutic range, including analgesics and limited triptan use, whereas nations such as Antigua, St Vincent, Guyana and St Lucia relied mainly on older non-specific analgesics with little or no access to triptans, neuromodulation or novel agents in some cases.
Overall, a duality of practice exists in the region, whereby certain medications are available but may be restricted to the private sector. This disparity creates significant barriers to equitable treatment access, as patients reliant on the public health system may be unable to obtain migraine specific therapies. Consequently, the distribution of care is uneven, with those able to afford private treatment benefitting from a wider therapeutic range, while others are limited to older, less effective options. Further studies are warranted to examine the extent of these disparities and to create strategies aimed at improving equitable access to migraine care across the Caribbean.
Discussion
This study confirms that migraine care in the English-Speaking Caribbean is plagued by many of the issues that affect other low-and middle-income countries (LMICs) worldwide.
Mortel et al., 10 in their 2022 review of barriers to headache care in LMIC noted that accurate diagnosis and management of headache disorders at a systemic level relies on physicians of all levels providing optimal management for common disorders. Whilst some countries in the English-Speaking Caribbean offer exposure to migraine management at the undergraduate medical school level, it is often minimal, and six of the seven countries noted there were no migraine specific Continuing Medical Education (CME) opportunities (Trinidad and Tobago was the exception, noting sporadic CME opportunities). Specific headache education is lacking in many LMIC, including Latin America which consist of approximately nine percent of the global population. 11
Further, there was a striking dearth of practicing neurologists across the participating nations, with several islands reporting only one practicing adult neurologist, confirming the 2017 World Health Organization (WHO) Atlas of Country Resources for Neurological Disorders’ finding that neurologists are in short supply in most LMIC. The Atlas further cements that the region of the Americas (of which the Caribbean is a part), consistently ranked amongst the lowest not only in terms of the available Neurologic workforce, but also in dedicated country policies for Neurologic disorders as well as in data reporting for these conditions, of which headaches comprised 32% of the data reported. 12
Consequently, four of the seven respondents reported that long waiting times and/or limited access to a specialist neurologist were barriers to migraine care. Discrete figures regarding the number of patients availing of specialist Neurology input were unfortunately unavailable, due to the fact that Electronic Medical Records are not standard across the islands, however the overall trend mirrors the situation found in Türkiye where there are free public hospitals, but long waiting times are a challenge to patients in the public sector. 13 The surveyed Neurologists also noted that though patients may seek to circumvent this obstacle by accessing healthcare through the private sector, this places them under a significant financial burden; which is yet another roadblock to proper migraine treatment in the region.
Access to acute therapies was a relative strength, with all respondents reporting access to several classes of acute therapies, including analgesics, antiemetics and triptans. Nonetheless, inequity was evident, as triptans were frequently unavailable. It is notable that persons in high-income countries have access to numerous triptan formulations, but those in LMICs face limited access and often at high costs, as demonstrated by Roxas et al. 14 in the Philippines and Alsaadi et al. 15 in the Middle East.
Similarly, preventative therapies were available in every country, usually via older agents on the WHO Essential Medicine List. 16 Inequity was again displayed, as CGRP monoclonal antibodies were universally unavailable in the region. Long-term studies support their long-term safety and efficacy 17 and the American Headache Society has recommended 18 that they be considered a first-line approach for migraine prevention. Rimegepant was available in some of the countries in this study, sometimes via special order only, thus likely remaining financially and functionally inaccessible. Anukoolwittaya et al. 19 have reported that most patients in Thailand are unable to reimburse CGRP-based treatment with either public coverage or private insurance. In LACs, diagnosis and treatment methods are often better in private institutions, but only some patients can afford access to these. 20 The Pan-African Medical Journal has published a practical guideline 21 on widely available medications for headache management, demonstrating a need for recommendations adapted to local resources. Pacheco-Barrios et al., 4 in their 2023 meta-analysis of population based studies, concludes that headaches are highly prevalent in LACs and recommends integrating modifiable risk factors into community-based interventions as a call for decisive action. Several countries have highlighted that, although North American organizations have proposed provisions aimed at improving migraine care in the region, these recommendations have yet to be effectively implemented.
Procedural interventions and non-pharmacologic therapies such as onabotulinumtoxin A injections and nerve blocks were reported as rarely available in our study, typically in the private setting only. None of the seven countries surveyed reported availability of neuromodulation devices, likely as these are still generally considered investigational are not covered by conventional insurance plans even in high-income countries. 22
Cultural practices often form a barrier to care. Teas, massages and marijuana are commonly used by patients in the English-Speaking Caribbean. Mortel et al. 10 have reported that cultural beliefs are a major factor on headache health-seeking behaviours, and myths and behavioural preferences often result in delayed or missed diagnoses, and thus failure to receive evidence-based treatment. None of the countries report any migraine advocacy groups. Gouider et al. 23 have concluded that advocacy efforts are urgently needed in LMIC to facilitate greater access to care and note that the delay in advocacy efforts in these nations are an opportunity to benefit from the lessons learnt from advocacy efforts in high income countries.
Hazard et al. 24 have performed similar descriptive analyses, specifically focusing on the economic impact of migraine within the United States, concluding that patients with migraine were both underdiagnosed and undertreated; which imposed a substantial socio-economic burden. Such infrastructural deficits are only compounded in LMICs such as the English speaking Caribbean, and we have detailed that a paucity of specialized training and dedicated headache clinics coupled with inordinate waiting times and financial factors results in delays in diagnosis and initiation of treatment. Limited access not only to first line but also novel medical therapies will in turn increase the prevalence of chronic migraine, further complicating the quality of life of patients.
There are numerous limitations to this study. There was one respondent from each country, limiting generalization of their responses to the population. Their responses were subjective and thus their recall of drug and procedure availability may be biased. Objective outcomes regarding medications dispensed or procedures performed were not assessed. Further limitations were also encountered, involving both pharmacologic and non-pharmacologic therapies. For instance, the range of triptans is not standardized across the islands, nor was integral behavioural interventions such as mindfulness or cognitive behavioural therapy available, which reflects further structural gaps in the Caribbean healthcare system.
The International Headache Society has recently advocated for raising the standards of migraine prevention and proposed a shift from percentage-based measures of success to absolute goals whilst on treatment, with control being deemed insufficient or optimal based on headache severity and migraine days. 25 The ultimate aim of this being to improve not only innovation in migraine treatment, but also the quality of life of patients with migraine.
Cephalgia Reports has also undertaken the advancement of migraine care, and is doing so by seeking to understand country-specific needs, thereby assessing their healthcare models and the implicit barriers that impede access to migraine care. 26 Whilst the limitations of this study must be considered, it nonetheless serves as a first step towards improving migraine management in the English-Speaking Caribbean. The strength of this survey study is that it is the first multi-country overview of migraine care in this region and thus the first set of region-specific data. It provides policymakers, healthcare administrators and physicians an empiric foundation for improving healthcare systems, particularly updating the formularies. Furthermore, it serves as a basis to guide further research. It is essential that patient-level data be collected moving forward and analysed in the context of the physician analysis provided herein. This study highlights that vigorous CME programs on migraine care should be initiated across the region and that neurology specialist training is desperately needed. Physicians and patients alike must collaborate on advocacy campaigns to raise awareness of the burdens imposed by migraine. The International Headache Society's ambitious goal of “migraine freedom” is difficult to achieve under the healthcare constraints demonstrated in this study.
Conclusion
This study details the first multi-country overview of migraine care in the English-Speaking Caribbean. It confirms major inequities, with limited access to triptans, preventative pharmacotherapies and procedural interventions. It highlights educational and advocacy gaps.
The International Headache Society has called for “migraine freedom” and striving for this means that Caribbean healthcare systems must expand the workforce, integrate CME opportunities for continuous medical education and update pharmaceutical formularies. Thereby seeking to bridge the existing gaps in healthcare infrastructure within the region, affording the significant neurologic burden of migraine the attention it deserves, as a means of mitigating it's downstream socio-economic consequences.
Clinical implications
Specialist workforce shortage: The surveyed Caribbean islands reported very few practicing neurologists, with virtually none having fellowship training in migraine/headache specifically.
Access barriers: Long waiting times in public clinics and high costs in the private sector significantly limit access to specialist neurology care.
Therapeutic gaps: Both acute and prophylactic migraine treatments show major deficiencies, with minimal availability of triptans and a complete absence of novel or modulatory therapies
Awareness deficits: There is an overall lack of migraine awareness among both patients and practitioners, highlighting the need for structured educational initiatives and advocacy programmes.
Supplemental Material
sj-docx-1-rep-10.1177_25158163251415565 - Supplemental material for Management of migraine in the Caribbean: A descriptive study
Supplemental material, sj-docx-1-rep-10.1177_25158163251415565 for Management of migraine in the Caribbean: A descriptive study by Joshua Duncan, Sesh Gowrie-Sankar, Saeed Rashaad Mohammed, Amza Ali and Avidesh Panday in Cephalalgia Reports
Footnotes
Acknowledgments
The authors would like to sincerely thank the neurologists across the English-speaking Caribbean who generously contributed their time and expertise by participating in this survey. We wish to acknowledge Dr L. Compton, Dr M. Adams, Dr S. Jacinto, Dr G. Osbourne, and Dr J. Watson, whose meaningful contributions to the completion of the survey were invaluable. Their insights were essential in providing a comprehensive regional perspective on migraine management and care.
Ethical considerations
Institutional review board approval was thus not required.
Consent to participate
This study did not utilize patient data nor were any personal data collected.
Consent for publishing
All authors reviewed and approved the final version of the manuscript and agree to be accountable for all aspects of the work and publish with Cephalalgia Reports.
Author contributions
Joshua Duncan: Conceptualization, Methodology, Formal analysis, Data curation, Project administration, Writing-original draft, Writing-review & editing.
Sesh Gowrie-Sankar: Conceptualization, Methodology, Project administration, Data interpretation; Writing-original draft, Writing-review & editing.
Saeed Rashaad Mohammed: Data interpretation, Writing-review & editing.
Amza Ali: Validation, Contribution to discussion and global health contextualization.
Avidesh Panday: Conceptualization, Methodology, Data acquisition, Data interpretation, Writing-review & editing, Supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during the current study are not publicly available due to the small number of respondents and the potential risk of indirect identification but are available from the corresponding author on reasonable request.
Open practices
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.