
Abstract
Introduction
Mechanical thrombectomy (MT) is standard of care for acute ischaemic stroke from large vessel occlusion following randomised controlled trials performed largely in high-income countries. Limited data exists on its effectiveness in the setting of low-and-middle-income countries. We aimed to evaluate the safety and efficacy of MT in a tertiary level public hospital in Cape Town, South Africa.
Methods
Patients with acute ischaemic stroke presenting consecutively to Groote Schuur Hospital between 1 January 2018 to 1 January 2022 with proximal intracranial occlusion in the anterior circulation treated with MT within 6 h from onset using computed tomography (CT) and CT angiography imaging-based protocols were evaluated. Demographic, clinical, radiological and procedural data were obtained from the stroke unit database. Recanalisation was evaluated post-procedure by modified Treatment in Cerebral Infarction score (mTICI). Functional independence (modified Rankin scores 0–2) and mortality at 90 days were also assessed.
Results
Thrombectomies were performed in 84 patients during the study period. The median age was 56 years (interquartile range, IQR) and 51% of participants were female. Median National Institute of Health Stroke Score was 18 and median baseline Alberta Stroke Programme Early CT score was 8. Bridging thrombolysis was given to 65% of participants. Median time from symptom onset to reperfusion was 339 min (IQR). Successful recanalisation (mTICI 2b/3) was obtained in 62%. At 90 days, 34% of participants gained functional independence and mortality was 34%.
Conclusion
This study demonstrated similar rates of recanalisation and functional independence to that seen in trials in high-income countries using basic imaging despite a higher mortality and longer median time to reperfusion. This data supports the effectiveness of MT in a tertiary level public hospital in South Africa despite the challenges of providing emergent stroke care in a resource-constrained setting.
Introduction
The benefit of mechanical thrombectomy (MT) in the treatment of acute ischaemic stroke due to large vessel occlusion (LVO) of the anterior circulation was established following five major randomised clinical trials in 2015, which demonstrated better functional outcomes at 3 months compared to best medical therapy alone.1–5 Pooled analysis of these trials by Hermes group showed that MT was effective overall and within sub-groups under-represented in the individual trials, such as the elderly, patients not receiving IV alteplase and those treated later than 300 min after stroke onset. 6 Subsequent trials have shown consistent superiority of MT compared to best medical treatment alone. Favourable outcomes have moreover been reported in the extended time periods up to 24 h for patients carefully selected using advanced imaging,7,8 in patients undergoing MT without thrombolysis 9 and in resourced constrained healthcare systems compared to the earlier trials.10,11
At Groote Schuur Hospital, we conducted a retrospective review of the clinical and interventional outcomes of patients who underwent MT from 1 January 2018 to 1 January 2022, utilising protocol-based recommendations from the updated American Stroke Association guidelines of 2015 12 for the management of acute ischaemic stroke due to LVO of the anterior circulation. We describe our disability, mortality, and recanalisation outcomes of MT for acute LVO stroke to assess its efficacy and safety in a South African public healthcare system, and analyse factors associated with these outcomes. We thereafter compare our results to published data from a randomised control trial in a comparable low-and-middle-income country (LMIC), namely Brazil, 10 as well as other similar published trials.
Methodology
Study design
A single centre retrospective review study. The study was approved and overseen by the Department of Surgery Research Committee and Human Research Ethics Committees at Groote Schuur Hospital (GSH).
Data collection methods
Neurovascular procedural reports for all patients undergoing MT for LVO from 1 January 2018 to 1 January 2022 were identified and cross-referenced with the GSH Stroke Unit clinical database. Data was extracted from the clinical database, and missing data obtained from folders, imaging, and telephonic interviews. All digital subtraction angiograms, pre-procedure and post-procedure, were independently reviewed by the author and stroke neurologist to determine the location of the initial large vessel occlusion and modified thrombolysis in cerebral infarction scale (mTICI) score. Discrepancies were resolved by consensus decision with an interventional neurosurgeon.
Participants
All patients undergoing MT for LVO at GSH from 1 January 2018 to 1 January 2022 were included. Eligible patients were above 18 years of age, pre-stroke score of 0 or 1 on modified Rankin scale (mRS), a clinical baseline of 6 or higher on the National Institutes of Health stroke Scale (NIHSS), with an arterial occlusion of the internal carotid artery (ICA), the first segment of middle cerebral artery (M1) or both confirmed by computed tomographic angiography (CTA) who had a baseline Alberta Stroke Program Early CT Score (ASPECT) above five and treatment initiated within 6 h from stroke onset.
Intervention
After triage in the emergency department, the stroke team reviewed and identified patients who met the clinical and radiological criteria for MT according to local hospital acute stroke protocols (Appendix 5). Patients who arrived within 4.5 h and without contraindication to thrombolysis were given 0.9mg/kg of IV alteplase (IVT).
MT was performed by experienced neuro-interventionalists: two neurosurgical consultants, one neurosurgical endovascular fellow and one consultant interventional radiologist. All cases were done under general anesthaesia. Neuro-interventional techniques included both Direct Aspiration First Pass Technique and use of stent retriever with Aspiration (SOLUMBRA), at the discretion of the treating neuro-interventionalist. After the procedure, patients were admitted to a neurocritical care unit for at least 24h for monitoring and optimised blood pressure management before transfer to a specialised postacute stroke ward for continued best medical therapy and rehabilitation.
Outcome variables
The primary outcome was the proportion of MT patients achieving an mRS of 0–2 (no or mild disability) or 6 (death) at 90-day post-stroke. The mRS is routinely evaluated at follow-up either in-person or telephonically by the attending neurologists at the post-reperfusion stroke clinic. For those patients with missing outcome data, telephonic assessment was carried out by a study investigator. The secondary outcome was the proportion of MT patients achieving successful post-procedure recanalisation defined by an mTICI grade of 2b, 2c or 3.
Statistical analyses
Descriptive data were generated as median and interquartile ranges for continuous variables, and frequencies and proportions for categorical variables. Analyses were run with SPSS version 26, with the threshold for statistical significance set at p = 0.05.
Comparison of the current dataset to RESILIENT, 2020 (Brazil)
Our data was compared to the RESILIENT trial, 2020(Brazil). One sample Wilcoxon rank tests were used to compare continuous variables to the RESILIENT data, and one sample binomial tests were used for the categorical variable comparisons.
Predictors of modified Rankin scale scores and successful recanalisation
Three separate logistic regression analyses were used to assess the predictors of (a) an mRS of 0–2; (b) an mRS of 6 (which indicates the patient died), and (c) successful recanalisation defined as a mTICI grade of 2b-3. Univariate analyses were run for between-group comparisons (independent sample t-tests for continuous variables and chi-square for categorical variables). Variables identified as having a significant difference/association with the outcome variables in the univariate analyses were entered into the regression model as predictors. Backwards stepwise logistic regression analyses were run to determine which variables from the univariate analyses remained significant predictors of the outcome variables.
Results
Participants
From 1 January 2018 to 1 January 2022, a total of 84 patients had MT done. The median age was 55.5 years, 43 (51.1%) were female. The median NIHSS score was 18 (IQR, 15–21). The baseline median ASPECT was 8 (interquartile range (IQR) 7–9) and 7 (8.3%) of whom had ASPECT score of <6. 55 (65.5%) received IV thrombolysis. Occlusion sites included M1 in 41 (48.8%), carotid terminus in 21 (25%), Tandem ICA in 18 (21.4%) and M2 & M3 level in 4 (4.8%) patients, respectively (Figure 1).
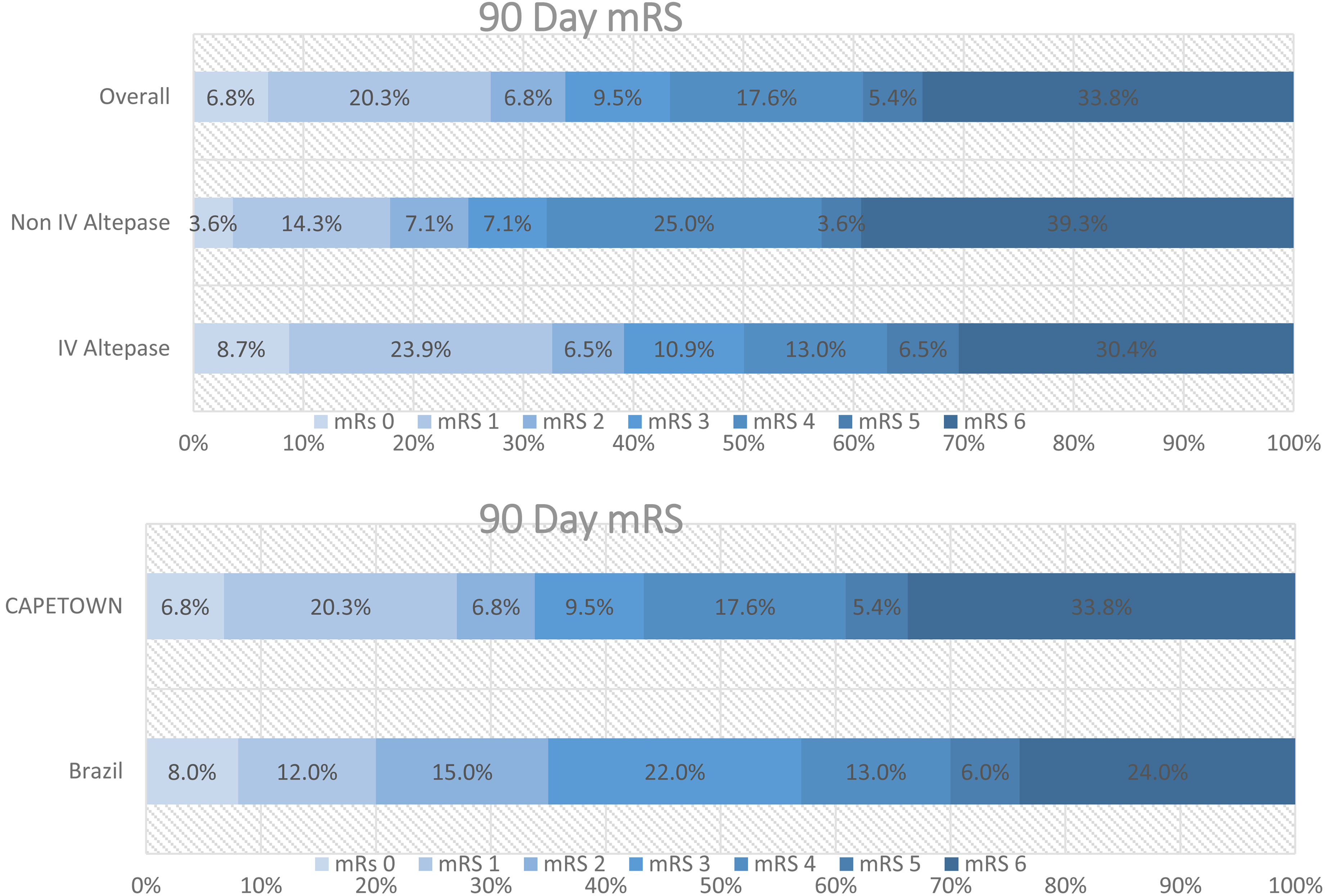
Scores on modified Rankin scale at 90 days. (A) Patients in our study according to use or non-use of IV alteplase and the overall outcome(Cape Town). (B) Comparison between overall outcome in our study and Intervention Group of RESILIENT(Brazil) trial.
When comparing patient baseline characteristics between our study and RESILIENT, the following significant differences were found. Our patient group was younger (p ≤ 0.001), and we had a significantly lower proportion of patients with stroke in the left hemisphere (p = 0.039), significantly higher proportion of patients with M1 and extracranial (tandem) occlusion (p ≤ 0.001) and a significantly higher proportion of patients with atrial fibrillation (p = 0.005) but significantly fewer patients with congestive cardiac failure (p = 0.002) (Table 1).
Baseline patient characteristics of cohorts from Cape Town and Brazil.
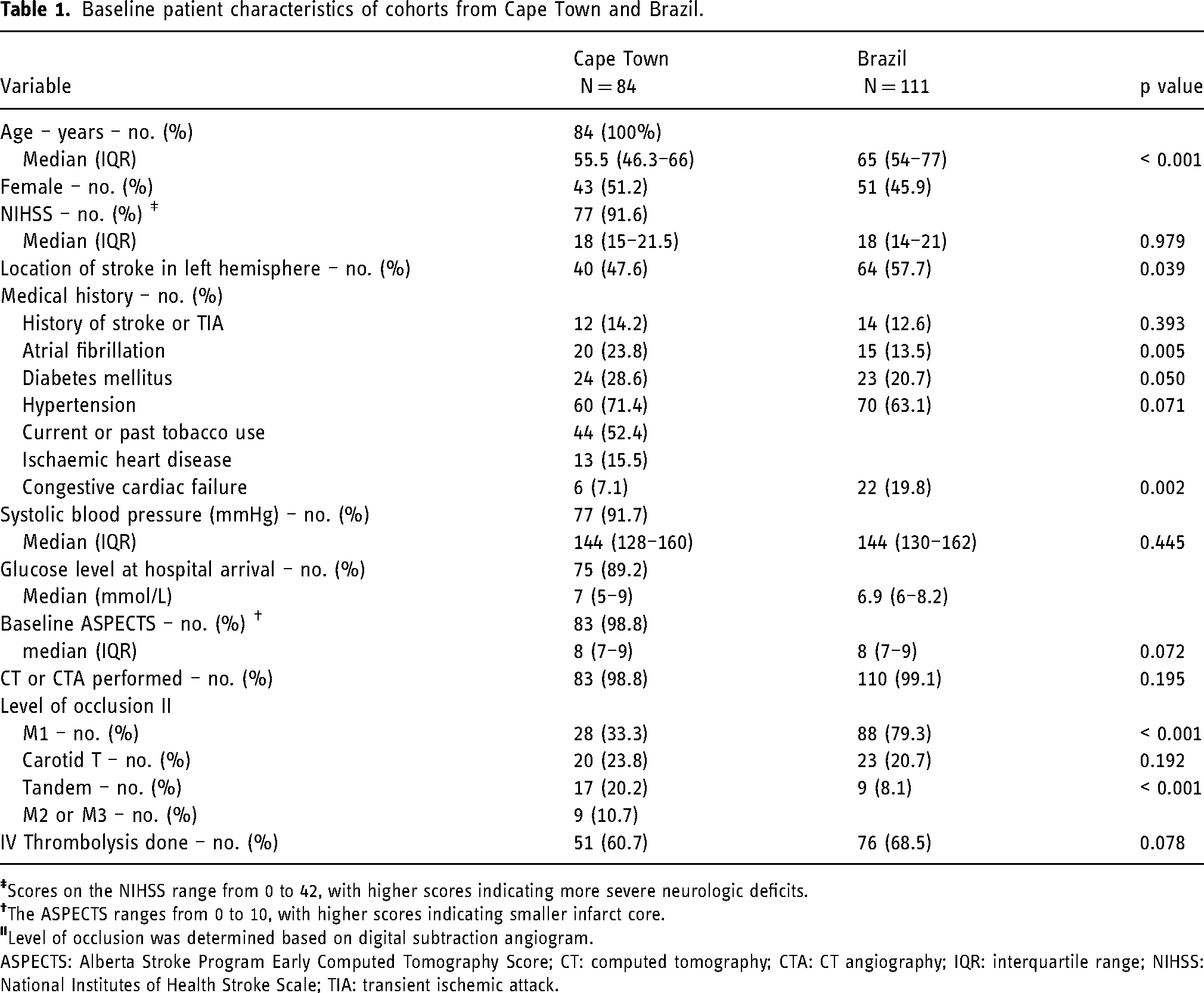
ASPECTS: Alberta Stroke Program Early Computed Tomography Score; CT: computed tomography; CTA: CT angiography; IQR: interquartile range; NIHSS: National Institutes of Health Stroke Scale; TIA: transient ischemic attack.
Procedural outcome
Intravenous thrombolysis was started at a median of 175 min (IQR, 135.8–210) for 32 (65.5%) of the eligible patients. Median time of stroke onset to groin was 297 min, (IQR, 236–350). Median procedural duration (groin puncture to recanalisation) was 39 min (IQR, 23–58). Median time of onset to reperfusion was 339 min (IQR, 287–394) (Table 2).
Treatment pathway time variables.*
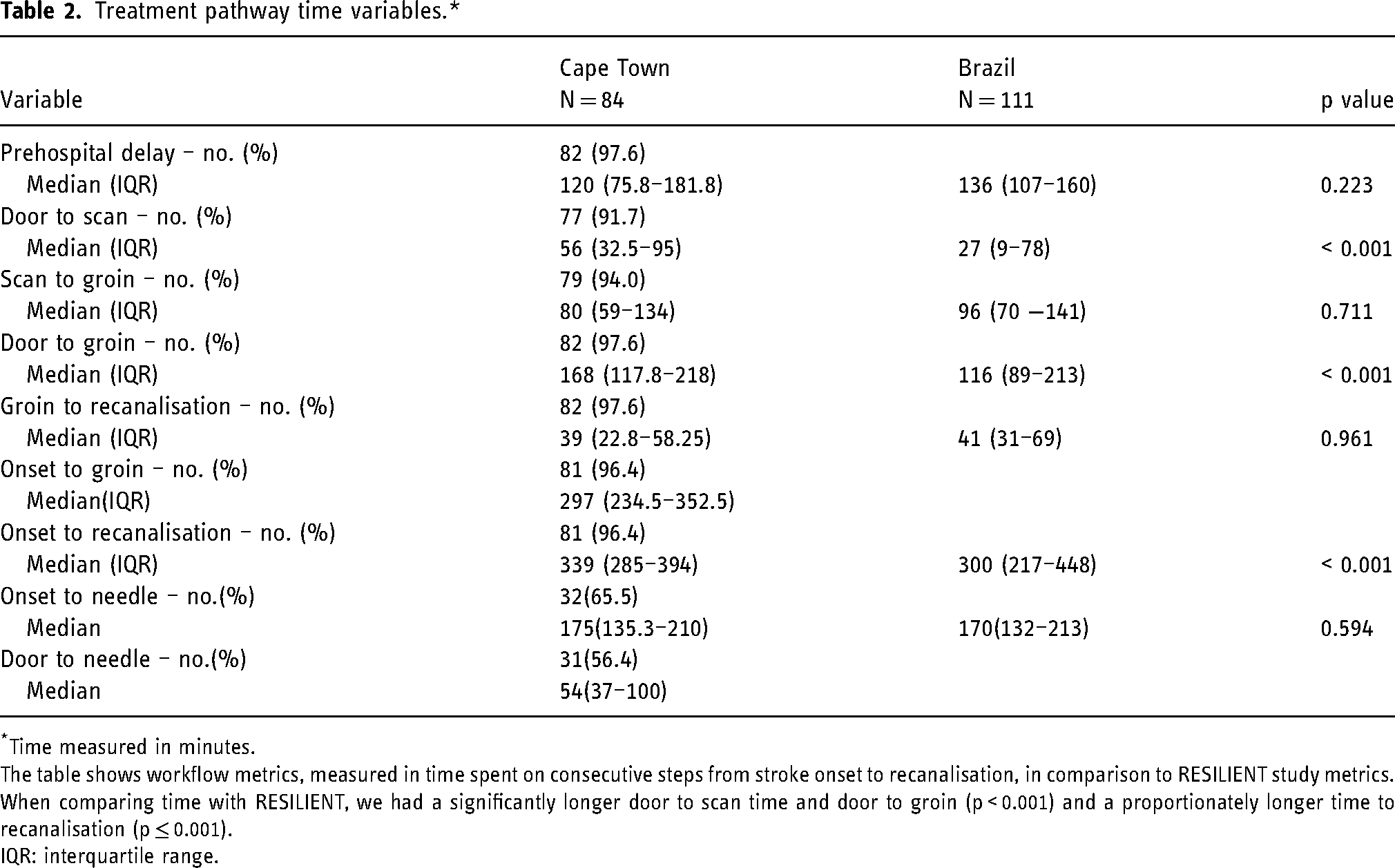
*Time measured in minutes.
The table shows workflow metrics, measured in time spent on consecutive steps from stroke onset to recanalisation, in comparison to RESILIENT study metrics.
When comparing time with RESILIENT, we had a significantly longer door to scan time and door to groin (p < 0.001) and a proportionately longer time to recanalisation (p ≤ 0.001).
IQR: interquartile range.
Primary and secondary outcomes
The primary outcome, mRS at 90 days was collected from 74 patients, of which 25(33.9%) were functionally independent with mRS 0, 1 or 2 and 25(33.8%) died (mRS 6).
Successful recanalisation, mTICI 2b, 2c, and 3 was achieved in 52 (61.9%). The procedure failed in two patients; one due to stenosis of cervical segment of ICA limiting access to the clot and the second patient had a blister aneurysm that bled. Both patients were included in the study as an mTICI 0.
Comparative statistical analysis done with a one sample binomial test on primary and secondary outcomes indicated that proportion of patients with mRS of 0–2 was similar between our study and RESILIENT study (p = 0.488), proportion of patients who died, mRS of 6 was significantly higher in our sample and proportion of patients with successful recanalisation was significantly higher in RESILIENT study compared to ours (p < 0.001) (Table 3).
Primary and secondary outcomes.
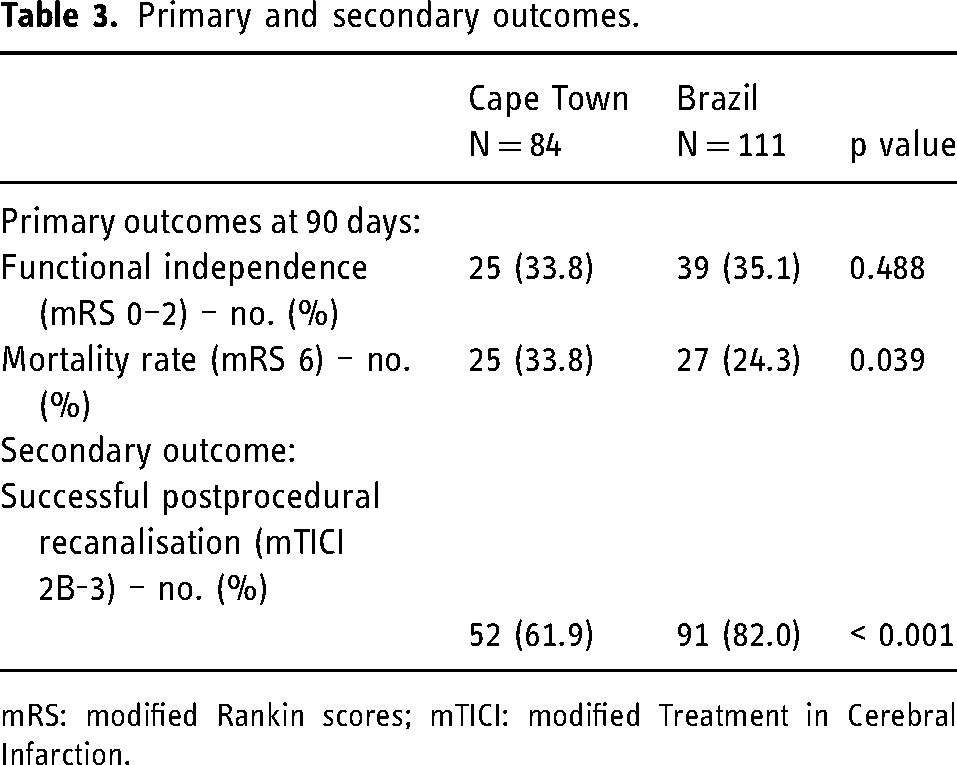
mRS: modified Rankin scores; mTICI: modified Treatment in Cerebral Infarction.
Predictors of disability, mortality and successful recanalisation
Predictors of modified Rankin scale scores 0–2
Univariate variate analyses found a significant association between an mRS of 0–2 and Carotid T occlusion, NIHSS and ASPECT (see Table 4). There was a trend towards a significant association with age and NIHSS. These significant variables were entered into a logistic regression model. The final model was statistically significant (χ2 = 13.13, p = 0.004), correctly classified 76.1% of patients, and had a Nagelkerke R2 of 0.248. Patients with an mRS score of 0–2 were less likely to have Carotid T occlusion site, were younger in age, and had a higher ASPECT score (Table 4).
Associations with mRS of 0–2.
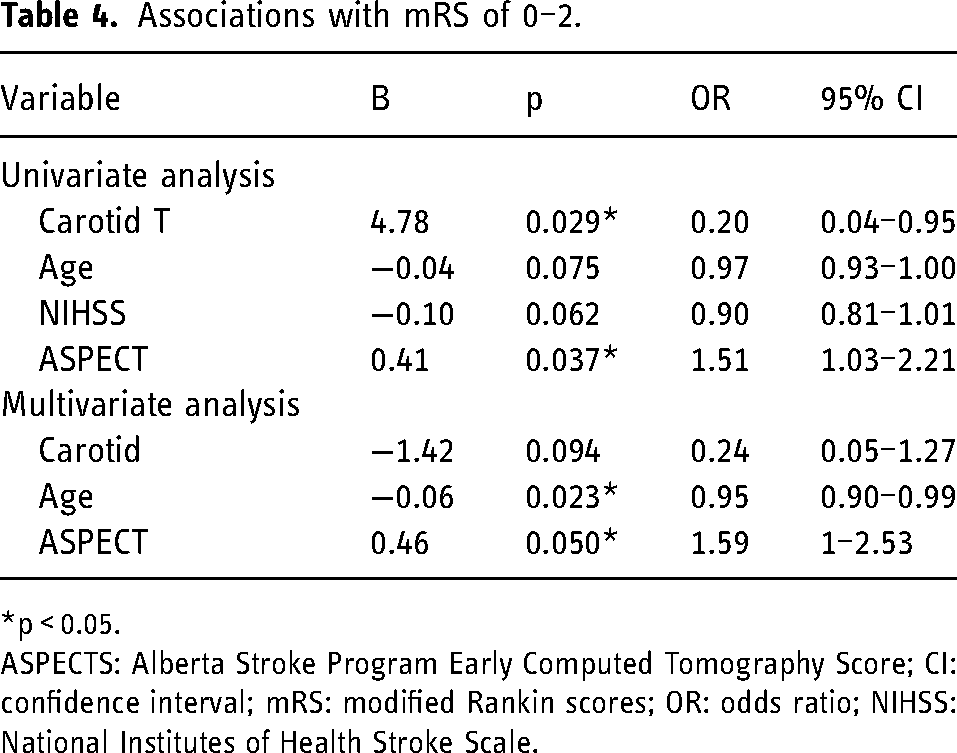
*p < 0.05.
ASPECTS: Alberta Stroke Program Early Computed Tomography Score; CI: confidence interval; mRS: modified Rankin scores; OR: odds ratio; NIHSS: National Institutes of Health Stroke Scale.
Predictors of modified Rankin scale scores of 6
Univariate variate analyses found a significant association between mRS of 6 and hypertension, Carotid T and time from scan to groin (see Table 5). There was also a trend in a significant association with time from door to scan. These variables were entered into a logistic regression model. The final model was statistically significant (χ2 = 24.12, p < 0.001), correctly classified 83.3% of patients, and had a Nagelkerke R2 of 0.475. Patients with an mRS score of 6 were more likely to have Carotid T occlusion site, more likely to have hypertension, had a longer Door to scan time but a shorter scan to groin time (Table 5).
Associations with mRS of 6.
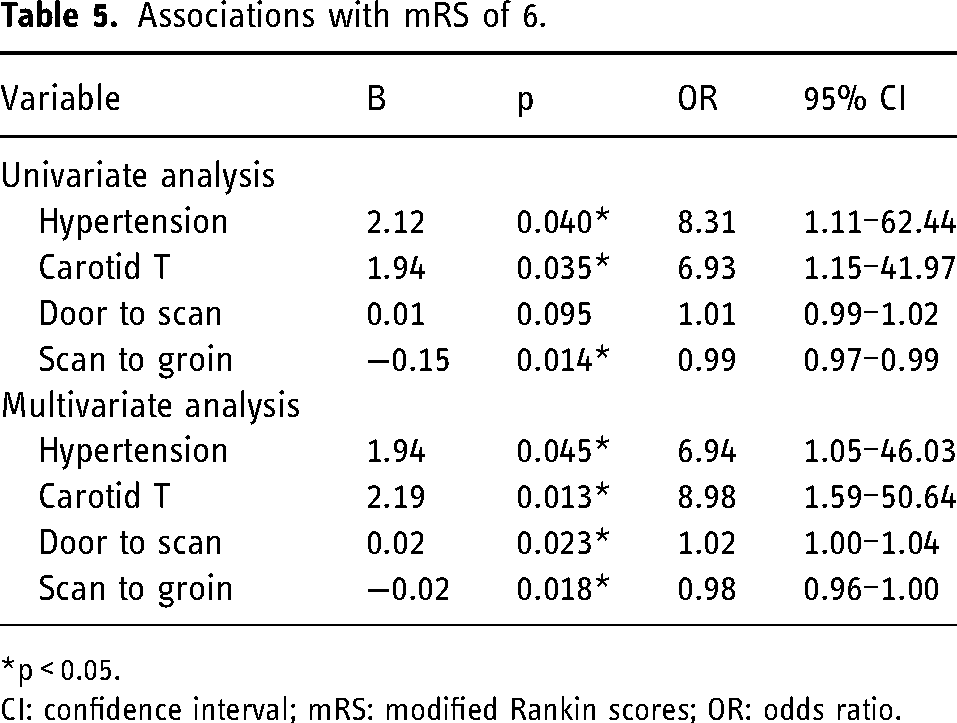
*p < 0.05.
CI: confidence interval; mRS: modified Rankin scores; OR: odds ratio.
Predictors of successful recanalisation (grade 2b-3)
Univariate variate analyses found a significant association between successful recanalisation and previous stroke, atrial fibrillation, and time from groin to perfusion (see Table 6). These significant variables were entered into a logistic regression model. The final regression model was statistically significant (χ2 = 15.39, p < 0.001), correctly classified 68.3% of patients, and had a Nagelkerke R2 of 0.234. Patients with successful recanalisation were less likely to have had a previous stroke, but more likely to have atrial fibrillation (Table 6).
Associations with grade 2b-3.
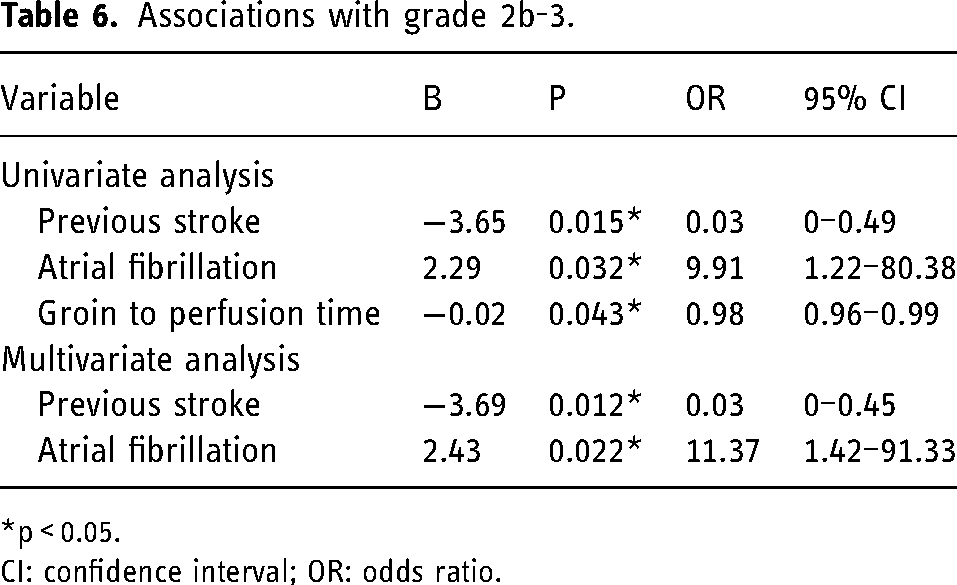
*p < 0.05.
CI: confidence interval; OR: odds ratio.
Discussion
South Africa is one of the most highly populated countries in sub-Saharan Africa with a population of 52 million people. 13 Just like many LMICs, stroke is a major cause of morbidity and mortality; and was declared a catastrophic illness in South Africa in October 2007. 14 Although the incidence is not known, the age-standardised prevalence of stroke is estimated at 290 per 100,000. 15 Ischaemic stroke accounts for a large amount of disability (95,000 years lived with disability) and mortality (25,000 deaths/year) in South Africa. 16 GSH is one of the two tertiary level public hospitals with endovascular capabilities in Cape Town, a city with an estimated population of 3.7 million people. 17
Standardised stroke protocols were implemented at GSH in 2018 utilising uncontrasted CT brain and CTA to select patients with acute ischaemic stroke due to LVO for MT (Appendix 5), using criteria similar to that used in the Mr CLEAN study performed in the Netherlands (2015). This retrospective analysis of data from 1 January 2018 reveals recanalisation rates and 3-month disability outcomes comparable to Mr CLEAN and RESILIENT(Brazil) studies, supporting the effectiveness of MT in middle-income countries despite the challenges facing health systems in this setting.
Our primary outcome was evenly distributed in thirds, one-third of the patients achieved functional independence (mRS 0–2), one-third dependant (mRS 3–5) and a third mortality (mRS 6) at 90 days. Young age and higher ASPECT scores had positive predictive value for mRS 0–2. Our study had a younger population, with a median age of 55 years at presentation compared to currently published trials from RESILIENT and HERMES Collaboration where their median age was 65 and 68 years, respectively. Seven (8.3%) of the patients included in this study had APECT scores lower than 6 and therefore were likely to have had a larger a much larger ischaemic core prior to treatment. MT in patients with a larger ischaemic core may be effective in improving overall disability but fewer patients with large core infarcts achieve functional independence compared to those with small ischaemic core. 18
The secondary outcome, mTICI 2b-3 was achieved in 62% of the patients. Success of recanalisation has been identified as one of the most important modifiable factors affecting disability 19 however it did not reach statistical significance in this study.
Patients who received thrombolysis had trend towards higher functional independence and lower mortality rate at 90 days. All patients who received thrombolysis, barring two patients referred from a private Hospital, were administered intravenous alteplase at our facility. Both ‘mothership’ and ‘drip-and-ship’ models of acute stroke are employed in the state-funded hospital referral networks in Cape town but the ‘mothership’ model predominates, particularly after hours where services services and expertise may not be available at smaller facilities.
Due to limited resources, less established stroke triage and response systems compared to higher income countries, there were pre-hospital and in-hospital delays, and ultimately longer time to treatment. Median time from symptom onset to recanalisation was 339minutes, which is much higher than what has been reported in other centres – including RESILIENT trial who had median time of 300 min. 10 Onset to groin time has been shown to be an independent factor that affects success of recanalisation, 20 and our results indicate the need for improved in-hospital management protocols and performance to optimise outcomes. Some of the factors that contributed to in-hospital delays included lack of pre-hospital notification, delay in folders retrieval and triage, time to scan and the time to assemble the on-call stroke teams after decision is made. Long door to scan time was one of the factors associated with mortality in our study (Table 5).
The long onset to groin time also highlighted the potential benefit for having advanced perfusion-based imaging which would improve patient selection, as well as be used to evaluate and add on patients who arrive to hospital during the extended window period with clinical deficit infarct volume mismatch.7,8
Despite, a higher mortality rate, we achieved comparable results to other trials. The percentage of patients with mRS of 0–2 of 33.8% in our study was comparable to MR CLEAN, 32.6%, and RESILIENT trial 39% which even though was slightly higher, a one-sample binomial test showed the difference was not significant. While RESILIENT trial selection criteria was more accommodative, extending eligibility time of stroke onset to treatment up to 8 h; 50(45%) of their participants in the intervention group were selected based on advanced CT perfusion imaging. They also achieved an overall significantly higher recanalisation rate of 82% and lower mortality of 24.3%. The mortality rate of 33.8% found in our study, is the highest compared to the currently published randomised control trials. Hypertension, Carotid T level of occlusion, longer time to scan, and scan to groin were found to have significant association. Even though no clear statistically significant mortality benefit is established in previous outcome studies of MT compared to the best standard medical therapy alone, there is a trend in favour of MT. 21 Our study being retrospective and non-randomised we were not able to compare our outcomes to standard medical therapy alone.
Conclusion
Our study represents a real-life scenario and outcome in a public healthcare system in sub-Saharan Africa. We achieved similar rates of recanalisation (61.9%) and functional independence (33.9%) to that seen in published trials from high-income and other LMICs using basic imaging despite a higher mortality and longer median time to reperfusion. These data support the effectiveness of MT in a public hospital in South Africa despite the challenges of providing emergent stroke care in a resource-constrained setting.
Strengths
The data is from a high-volume state hospital that offers comprehensive stroke care in South Africa.
Limitations
Some of the limitations of our study included loss to follow up of 10(12%) of the patients by the 90th day. Being a real-life retrospective non-randomised study, with MT as standard of care for eligible patients, there was no control group with standard medical therapy alone to compare our outcomes to. The outcomes were assessed by the investigators who are part of the stroke team involved in the management of the patients.
Footnotes
Abbreviations
Author contributions
MMK, AT and KB assisted with data collection. MMK, KB, AT and DLF analyzed the data. All authors had access to the dataset, assisted with data review and manuscript preparation, and approved the final manuscript.
Declaration of conflict of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
The study was approved and overseen by the Department of Surgery Research Committee (Project 2019/073) and Human Research Ethics Committees at Groote Schuur Hospital (GSH) (HREC ref 444/2019).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix 1