
Abstract
Background
Despite the high prevalence of migraine in Europe, there is limited research on the burden among people with migraine.
Methods
This cross-sectional survey used patient-reported data from the 2020 European National Health and Wellness Survey in France, Germany, Italy, Spain, and the United Kingdom. The study assessed the sociodemographic characteristics, health-related quality of life, depression, work productivity and activity impairment, and healthcare resource utilization among matched samples of people with diagnosed migraine (n = 3985) and compared to a matched cohort without migraine (n = 7970). The study also analyzed the burden across migraine subgroups stratified by the number of migraine headache days.
Results
Lower health-related quality of life, higher depression, increased work productivity and activity impairment, and higher healthcare resource utilization were reported among people with migraine and ≥1 migraine headache days compared to matched people without migraine (all p < 0.001). Additionally, the incremental burden was also observed across migraine subgroups (1–3, 4–7, 8–14, and ≥15 migraine headache days) irrespective of the use of prescription medication compared to the matched controls without migraine.
Conclusion
Migraine sufferers with ≥1 migraine headache days experienced worse productivity, lower quality of life, depression, and increased healthcare resource utilization than those without migraine, emphasizing the need for effective management strategies.
Keywords
Introduction
Migraine is a debilitating neurological disorder characterized by recurrent attacks of moderate to severe headaches which affect over one billion people worldwide (1,2). The age-standardized point prevalence and annual incidence rate of migraine were reported as 14,107.3 and 1142.5 per 100,000 of the population (3). Epidemiological data show that migraine prevalence is higher in females and young adults (2). The prevalence of migraine varies widely across countries and regions, with a prevalence of 11.4% in Europe (Eur.) (4).
Migraine is the second leading cause of disability worldwide as measured by years lived with disability (YLDs), and the first among young women based on disability-adjusted life years (DALYs), making it a significant public health concern (5). Migraine imposes a significant burden on patients’ daily activities, health-related quality of life (HRQoL), productivity, healthcare cost, and overall well-being and correlates with the frequency and severity of migraine attacks (6,7). Furthermore, the burden of migraine in terms of patient-reported outcomes and healthcare resource utilization (HCRU) was reported to be high among patients who have previously failed multiple acute and preventive treatment options (8,9).
Studies conducted in Eur. have documented the impact of migraine in their population, noting important implications for health policy (10,11). One recent study reported an incremental burden among migraineurs experiencing ≥4 monthly headache days characterized by poorer HRQoL and increased (poorer) work productivity and activity impairment (WPAI) scores and greater HCRU (12). Another study reported an association between an increase in the number of headache-free days and improved HRQoL, lower impairment of work productivity and activity, and HCRU among patients with migraine in five Eur. countries, France, Germany, Italy, Spain, and the United Kingdom (UK) (5Eur.) (13). Recent research also revealed disparities in care access and health equity across geographical areas, particularly for migraine and secondary headaches, with North America and Eur. benefiting widespread treatment availability, while many countries globally lack access to these therapies (14,15).
Examining the specific needs of those diagnosed with migraine and the burdens associated with different frequencies of headaches per month may be useful to identify their unique patient needs, inform healthcare policy and resource allocation, and promote advocacy for increased research funding and improved access to care. Despite the high prevalence of migraine in Eur., there is limited research on the incremental impact among people with migraine compared to people without migraine.
A previous National Health and Wellness Survey (NHWS) study reported an incremental burden of migraine among respondents who suffer from migraine ≥4 monthly headache days in comparison to the matched no-migraine controls in 5Eur. The study concluded that individuals suffering from ≥4 monthly headache days had lower HRQoL, higher work and activity impairment, and higher HCRU (16). That study was limited by sample size and did not report country-level results. Also, the burden of migraine among patients receiving prescription medication (Rx) for their diagnosed migraine has not been evaluated in the 5Eur.
The objectives of the present study were to determine the incremental burden of migraine among a large cohort of adults with diagnosed migraine matched to adults who report no migraine. Moreover, the study examined the incremental burden of migraine through stratification by the number of migraine headache days (MHDs).
Methods
Study design and data source
This retrospective cross-sectional survey study used patient-reported data from the European 2020 NHWS that included France, Germany, Italy, Spain, and the UK, fielded between December 2019 and March 2020. NHWS is an annual, cross-sectional, patient-reported, internet-based questionnaire designed to describe the health and disease burden of the general adult population for over 200 therapeutic conditions (17,18). Eligible respondents included adults aged ≥18 years who have given their consent to participate in the survey and could read and write in the primary language of their country of residence. Respondents who reported experiencing migraine in the past 12 months completed an additional module with questions on migraine characteristics.
The survey respondents were recruited from opt-in survey panels, including Profiles and its partners. All working data files contained no identifying information that could personally identify the respondents. To ensure that the survey sample was representative, quota sampling was used to recruit respondents based on age and gender.
The study protocol and questionnaire for NHWS were reviewed by the Pearl Institutional Review Board and were granted an exemption. Potential respondents received an email invitation to complete the survey.
Study cohorts
The 2020 Eur. NHWS collected complete responses from 62,319 adult respondents, of which, 14,536 self-reported having migraine and completed the migraine module. The present study sample was divided into two cohorts: people with diagnosed migraine (PwM) and people without migraine (PwoM). Respondents self-reported a physician diagnosis of migraine and a minimum of one (≥1) MHD in the past 30 days were included in the PwM cohort. Conversely, respondents who did not report a physician diagnosis of migraine or who responded with ‘did not know’ or reported MHD = 0 were excluded from the cohort. Respondents who did not report any migraine in the past 12 months were included in the PwoM cohort. To accurately identify migraine headache days, if respondents reported experiencing migraines on any days (>0) in the past 30 days, they were asked about their total headache days. Headache day was defined as having at least 4 h of continuous pain with a peak intensity that is at least moderate to severe. Respondents from the matched migraine cohort were also stratified based on the frequency of mean MHDs: 1–3 MHDs, 4–7 MHDs, 8–14 MHDs, and ≥15 MHDs (Figure 1).
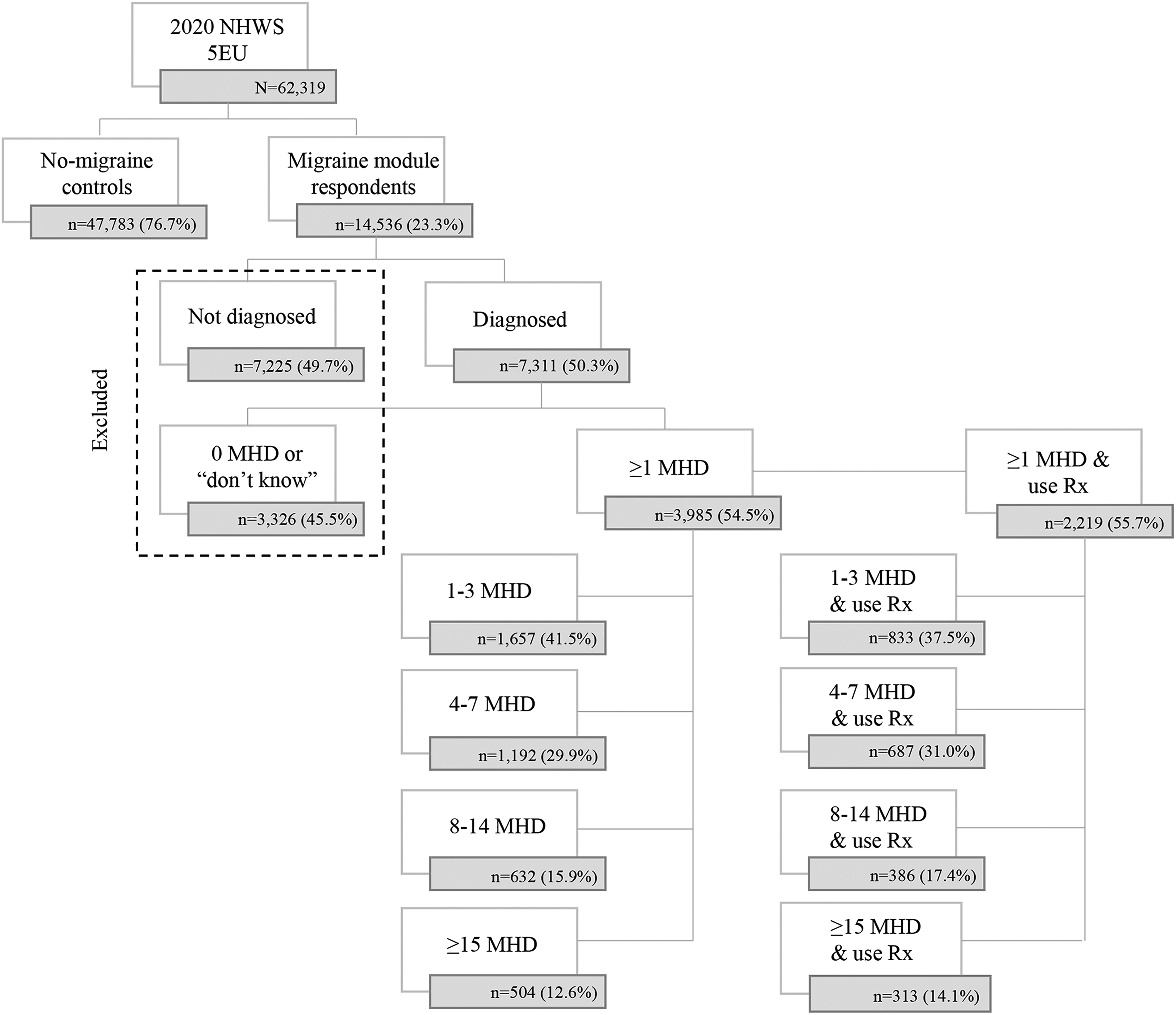
Cohort classifications. MHD, migraine headache days; NHWS, National Health and Wellness Survey; Rx, prescription medication. 5Eur. – France, Germany, Italy, Spain, and the United Kingdom.
As a sensitivity analysis, an additional cohort that consisted of those who were diagnosed with migraine and reported current use of any Rx for their migraine was included. This sensitivity analysis evaluated the potential differences in incremental burden among people with migraine who were currently receiving therapy and those without migraine as a confirmatory approach to the self-reported nature of the migraine diagnosis.
Study measures
This study assessed sociodemographic and general health characteristics, depression, humanistic and economic outcomes.
Sociodemographic and general health characteristics
The demographic variables collected included age, sex, marital status, university education, household income, and employment status. The study also captured general health characteristics including body mass index (BMI), comorbidities defined by the Charlson Comorbidity Index (CCI) (19), alcohol use, smoking behavior, and exercise frequency.
Health-Related quality of life
This study used the Medical Outcomes Study Short Form 12-item Survey (SF-12v2) to evaluate general HRQoL (20). The SF-12v2 generated two summary scores: the Mental Component Summary Score (MCS) and Physical Component Summary Score (PCS) (20). The norm-based algorithm used in the scoring process set the mean of each score to 50 and the standard deviation (SD) to 10. Lower scores indicated poorer health status. A change of 3 points represents the minimum clinically important difference (MCID) for both the MCS and PCS scores.
The EuroQoL-5D (EQ-5D) index score is a health measure that assesses health across five dimensions based on personal preferences and ranges from 0 to 1, where 1 represents full health and 0 is equivalent to death (21). The tool utilized a 5-point rating scale for each dimension. The index score for the UK was calculated using the standard value set for the UK, while the index values for France, Germany, Italy, and Spain were calculated using the crosswalk from the EQ-5D-3L, as a value set for the 5L version is not yet available. The MCID for the EQ-5D index measure is estimated to be approximately 0.074 points (21). The EQ-5D-5L also provided additional measures of HRQoL beyond the index, including the visual analog scale (VAS), which is a single item that allows respondents to rate their health on a scale of 0 (worst) to 100 (best).
Depression
Depression level was assessed using the Patient Health Questionnaire-9 (PHQ-9). The PHQ-9 uses nine items to screen, measure, or monitor a patient's level of depression. The PHQ-9 score ranges from 0 to 27, with higher scores indicating more severe depression. A sum score was used to categorize participants into four depression categories: none/minimal (0–4), mild (5–9), moderate (10–14), moderately severe (15–19), and severe (20–27) (22). The MCID generally used for the PHQ-9 mean score (rather than the defined category) is 5 for general use.
Work productivity loss and activity impairment
The General Health version of the Work Productivity and Activity Impairment Questionnaire (WPAI) was used to measure work productivity loss and activity impairment. The questionnaire consists of six questions that assess four metrics: absenteeism (absence from work due to health issues), presenteeism (health-related functionality exclusive of being physically present at work), overall work productivity loss, and activity impairment (23). The results are expressed as percentages, with higher percentages indicating greater impairment and lower productivity. All participants responded to activity impairment, however, only those who self-reported being employed provided responses for absenteeism, presenteeism, and overall work impairment.
Healthcare resource utilization
Respondents reported the number of times they visited any healthcare provider (HCP) in the past 6 months. HCRU was presented as both the percentage of respondents using each resource and the average number of visits to general practitioner (GP)/family practitioner (FP), neurologists, emergency room (ER), and hospitalizations.
Matching
To ensure the homogeneity among the variables between the PwM and PwoM, the study used exact matching by country and matched on a propensity score. Logistic regression was used to estimate a propensity score, which predicted the presence of migraine for each person in the study sample. Separate regression models were created for each country and included demographic (age, sex, marital status, household income, level of education), health (alcohol use, vigorous exercise, BMI), and clinical (CCI) measures. The greedy matching algorithm was used (24), which required an exact match on country and then a match on the propensity score within a caliper of ±0.1 SD (25). A 1:2 (case:control) matching ratio was used. The match was considered successful if all standardized mean differences (SMD) were less than 0.10 (26).
Statistical analyses
Descriptive statistics (means and SDs) were used to summarize continuous variables (age, CCI); counts and percentages for categorical variables were used to summarize sociodemographic and general health characteristics within study cohorts. Bivariate analyses (chi-square tests for categorical variables and student's t-test for continuous variables) were used to identify variables that were statistically different between PwM and PwoM cohorts.
Results
Respondent characteristics
Pre-matched
The pre-matched demographic, health, and clinical characteristics for PwM (n = 3985) and PwoM (n = 47,783) are presented in Table 1. The majority of the pre-matched demographic characteristics were significantly different between PwM cohorts and PwoM cohort. All variables were significantly different between pre-matched cohorts except BMI and exercise (p < 0.05) (Table 1).
Sociodemographic and general health characteristics in pre- and post-matched cohorts from 2020 Eur. NHWS data.
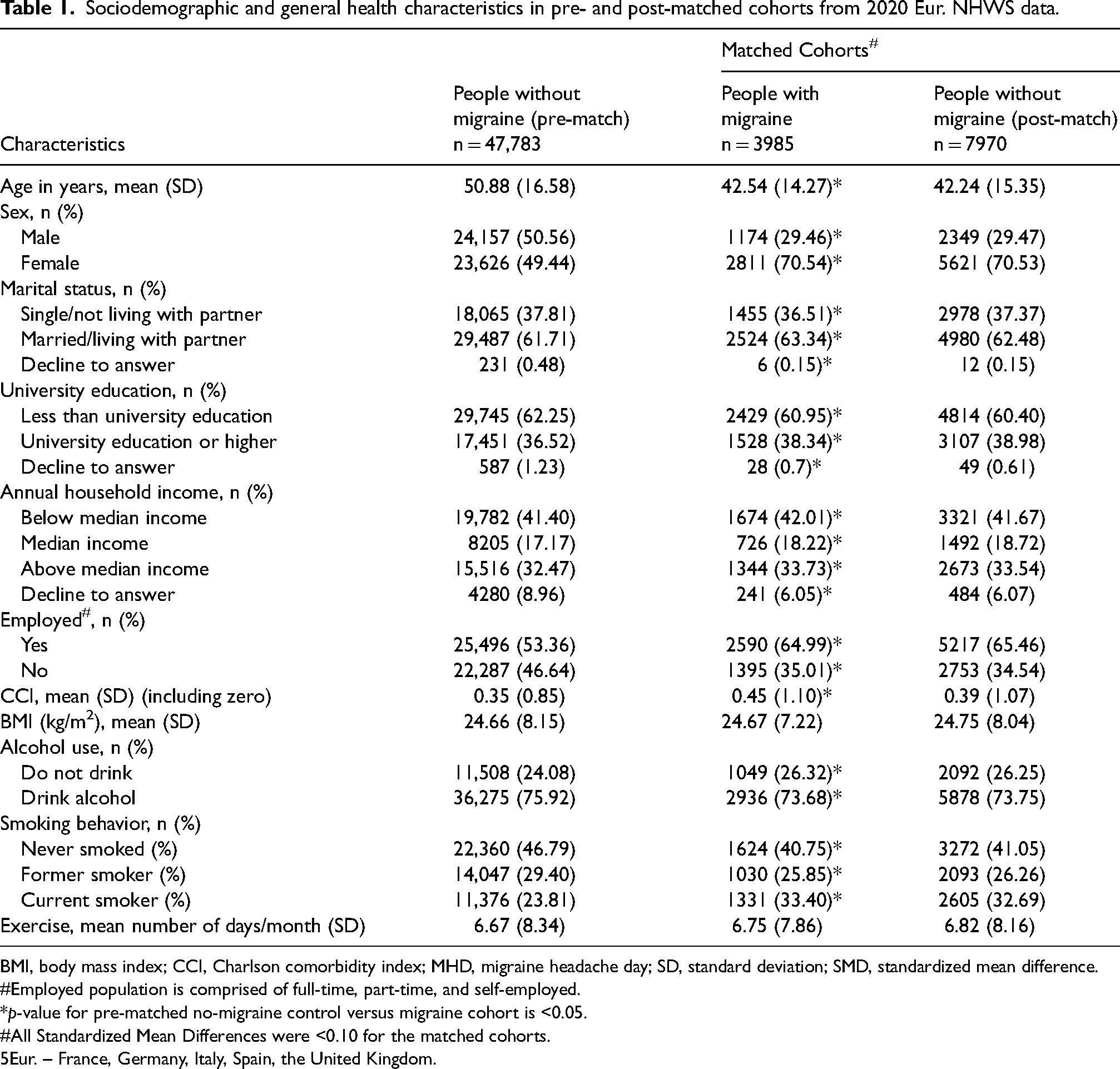
BMI, body mass index; CCI, Charlson comorbidity index; MHD, migraine headache day; SD, standard deviation; SMD, standardized mean difference.
Employed population is comprised of full-time, part-time, and self-employed.
*p-value for pre-matched no-migraine control versus migraine cohort is <0.05.
All Standardized Mean Differences were <0.10 for the matched cohorts.
5Eur. – France, Germany, Italy, Spain, the United Kingdom.
Post-matched
A successful 1:2 match with SMDs <0.1 for each variable was conducted on the complete PwM samples (no loss of cases) with the PwoM group. The mean age of matched cohorts of PwM and PwoM respondents was 43 years, and the majority of respondents were female (71%), married (63%) and had less than a university education (61%). Most respondents were employed (65%) and the mean CCI score was observed to be between 0.39–0.45. Both cohorts had a ‘normal weight’ BMI (25 kg/m2), 74% reported alcohol consumption, 41% of respondents reported never smoking, and on average, both groups exercised for approximately seven days a month (Table 1).
Comparison of people with vs. without migraine
Health-related quality of life
Results from the matched cohorts reported significantly lower SF-12 MCS and PCS (lower scores indicate worse health) for the PwM compared to PwoM (MCS: 40.63 ± 10.07 vs. 44.80 ± 9.80; PCS: 47.83 ± 9.26 vs. 50.98 ± 8.53; p < 0.001) with a difference of 4.2 and 3.2 in MCS and PCS. EQ-5D utility (0.73 ± 0.24 vs. 0.83 ± 0.21) and EQ-5D VAS (65.03 ± 24.64 vs. 73.60 ± 23.44) were also significantly lower in PwM compared to PwoM, representing a difference of 0.1 in EQ-5D scores (Figure 2).
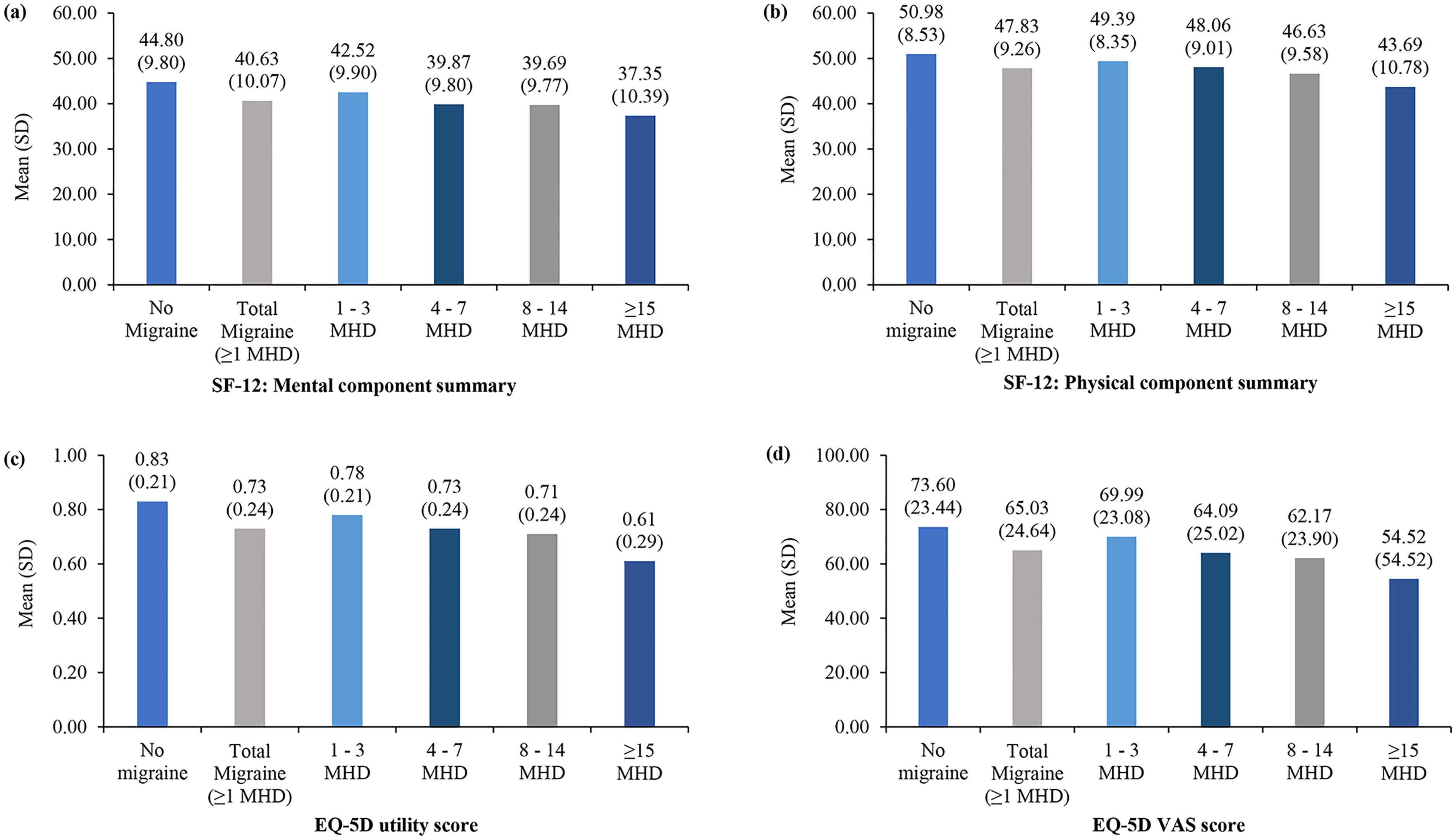
Quality of life in migraine (≥1 MHD), MHD subgroups, and without migraine cohorts in 5Eur. measured by (a) SF-12 MCS, (b) SF-12 PCS, (c) EQ-5D, and (d) EQ-5D VAS scores. EQ-5D VAS, EQ-5D visual analogue scale; MHD, migraine headache day; SD, standard deviation; SF-12, 12-item Short Form Health Survey.
PwM reported significantly higher (worse depression severity) PHQ-9 score than the PwoM cohort (8.96 ± 6.58 vs. 6.07 ± 5.96; p < 0.001). In the PwM cohort, around one-third of the respondents reported mild depression (PHQ-9 score 5–9; 31.42%), however in PwoM, half of the respondents reported none to minimal depression (PHQ-9 score 0–4; 50.87%). The proportions of respondents with mild (PHQ-9 score 5–9; 31.42% vs. 25.26%), moderate (PHQ-9 score 10–14; 19.37% vs. 13.20%), moderately severe (PHQ-9 score 15–19; 11.52% vs. 7.08%), and severe depression (PHQ-9 score 20–27; 8.31% vs. 3.60%) were significantly higher in PwM compared to PwoM (Figure 3).
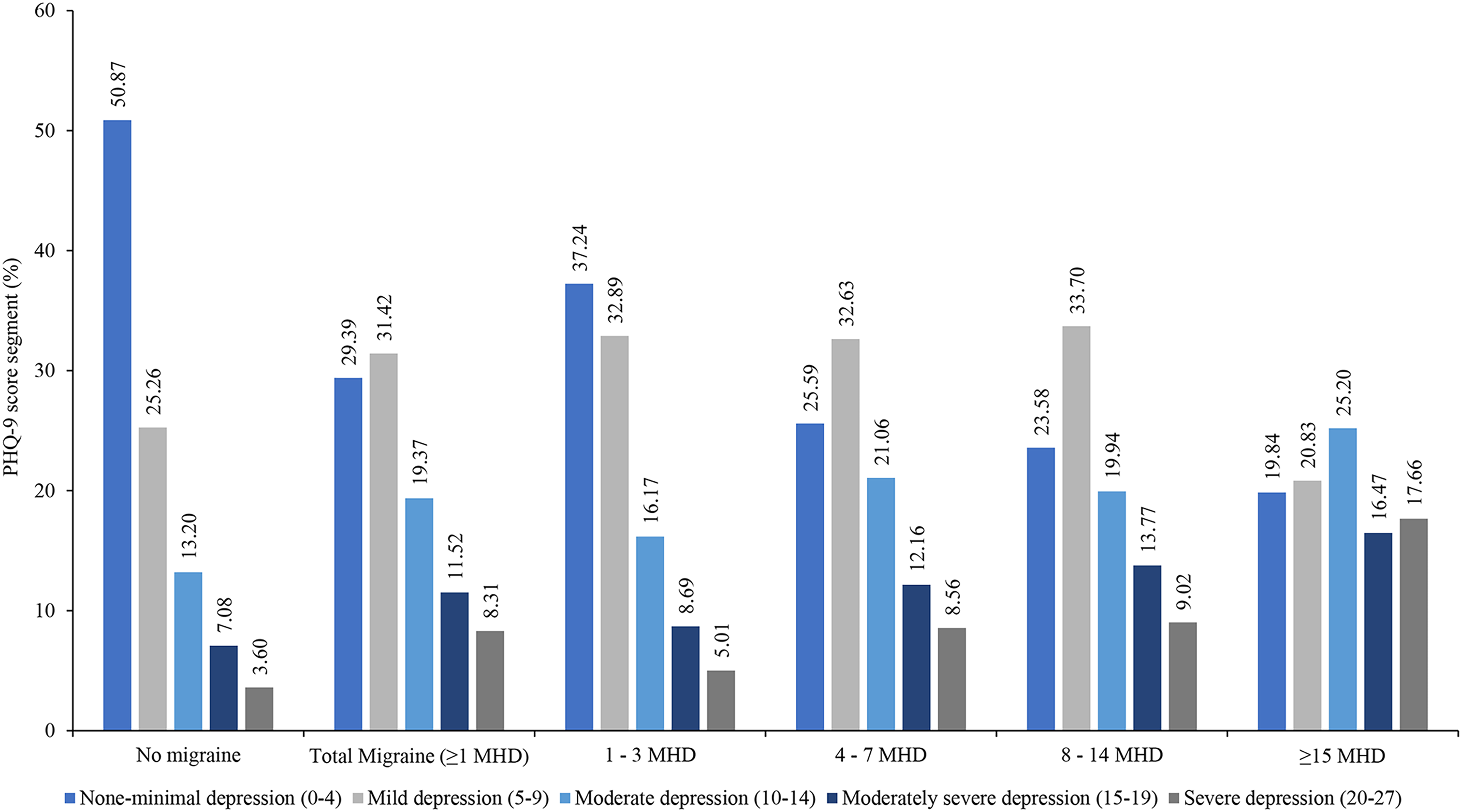
Depression measured by PHQ-9 in migraine (≥1 MHD) cohort, MHD subgroups, and without migraine cohort in 5Eur. respondents. MHD, migraine headache day; PHQ-9, Patient Health Questionnaire-9. 5Eur. – France, Germany, Italy, Spain, and the United Kingdom.
Work productivity loss and activity impairment
Among the employed respondents, PwM reported significantly higher absenteeism (14.36 ± 25.91 vs. 9.47 ± 22.39) and higher presenteeism (34.77 ± 27.88 vs. 21.92 ± 27.17) than PwoM (p < 0.001 for all). The total work impairment (41.59 ± 32.35 vs. 26.96 ± 32.17; p < 0.001) and activity impairment (40.50 ± 28.65 vs. 26.37 ± 28.40; p < 0.001) were significantly higher in PwM compared to PwoM (Figure 4).
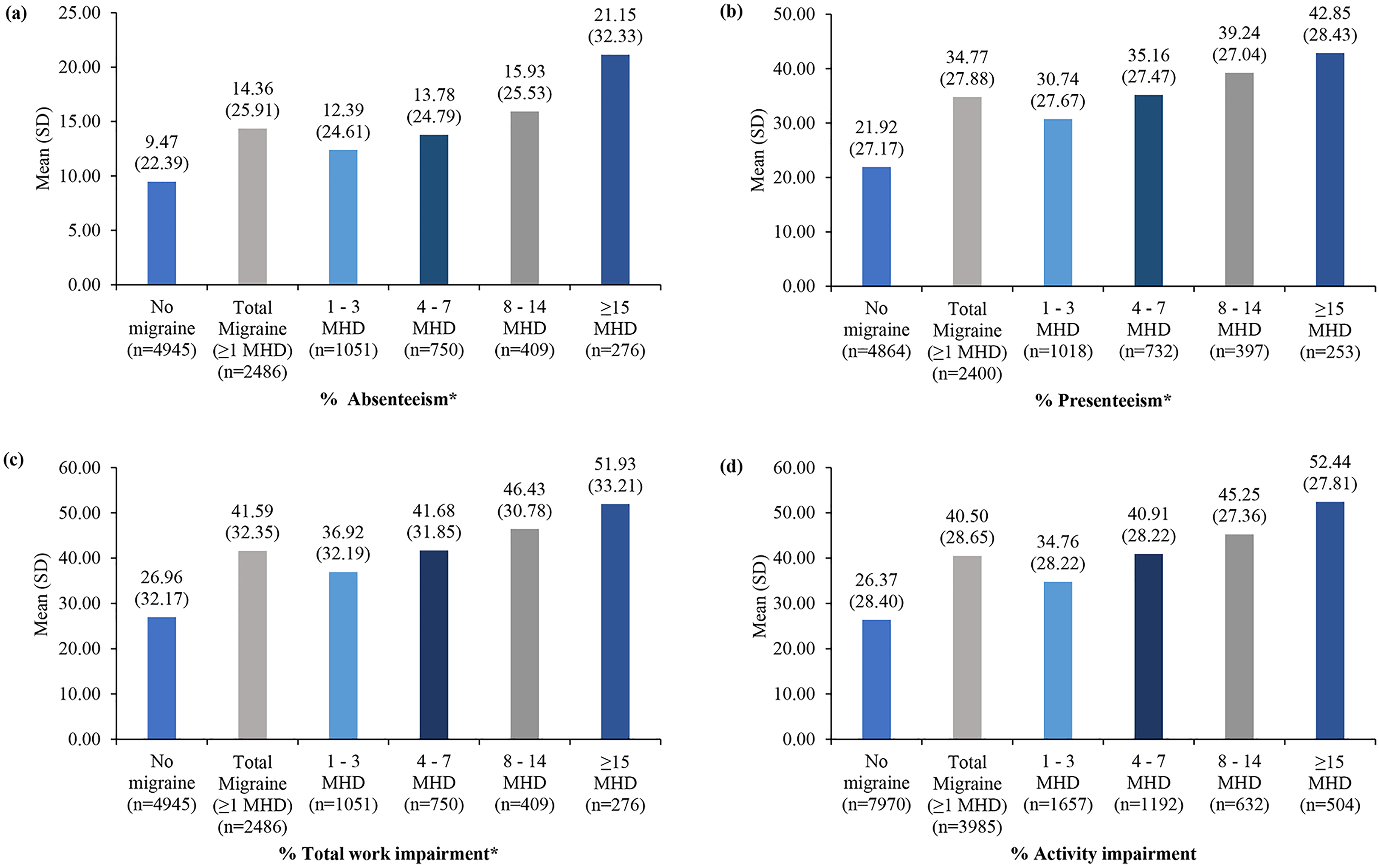
Productivity in migraine and without migraine cohorts: (a) absenteeism, (b) presenteeism, (c) total work impairment, and (d) activity impairment, in 5Eur. respondents. MHD, migraine headache day; PHQ-9, Patient Health Questionnaire-9; SD, standard deviation; WPAI, Work Productivity and Activity Impairment Questionnaire. *Only from employed sample.
Healthcare resource utilization
A significantly higher proportion of PwM reported a visit to a GP/FP (76.19% vs. 59.89%), ER (28.93% vs 16.39%), neurologist (12.12% vs. 3.61%), and hospitalization (15.76% vs. 9.80%) compared to PwoM (p < 0.001 for all). In particular, the mean number of health care visits, including GP/FP visits (2.65 ± 3.47 vs. 1.57 ± 2.55; p < 0.001), ER visits (0.64 ± 1.88 vs. 0.33 ± 1.15; p < 0.001), neurologist visits (0.22 ± 1.04 vs. 0.07 ± 0.56; p < 0.001) and hospitalization (0.32 ± 1.90 vs. 0.22 ± 1.44; p = 0.001) reported in the past six months were significantly higher in PwM than PwoM (Table 2).
Healthcare resource utilization in people with migraine versus matched controls without migraine.
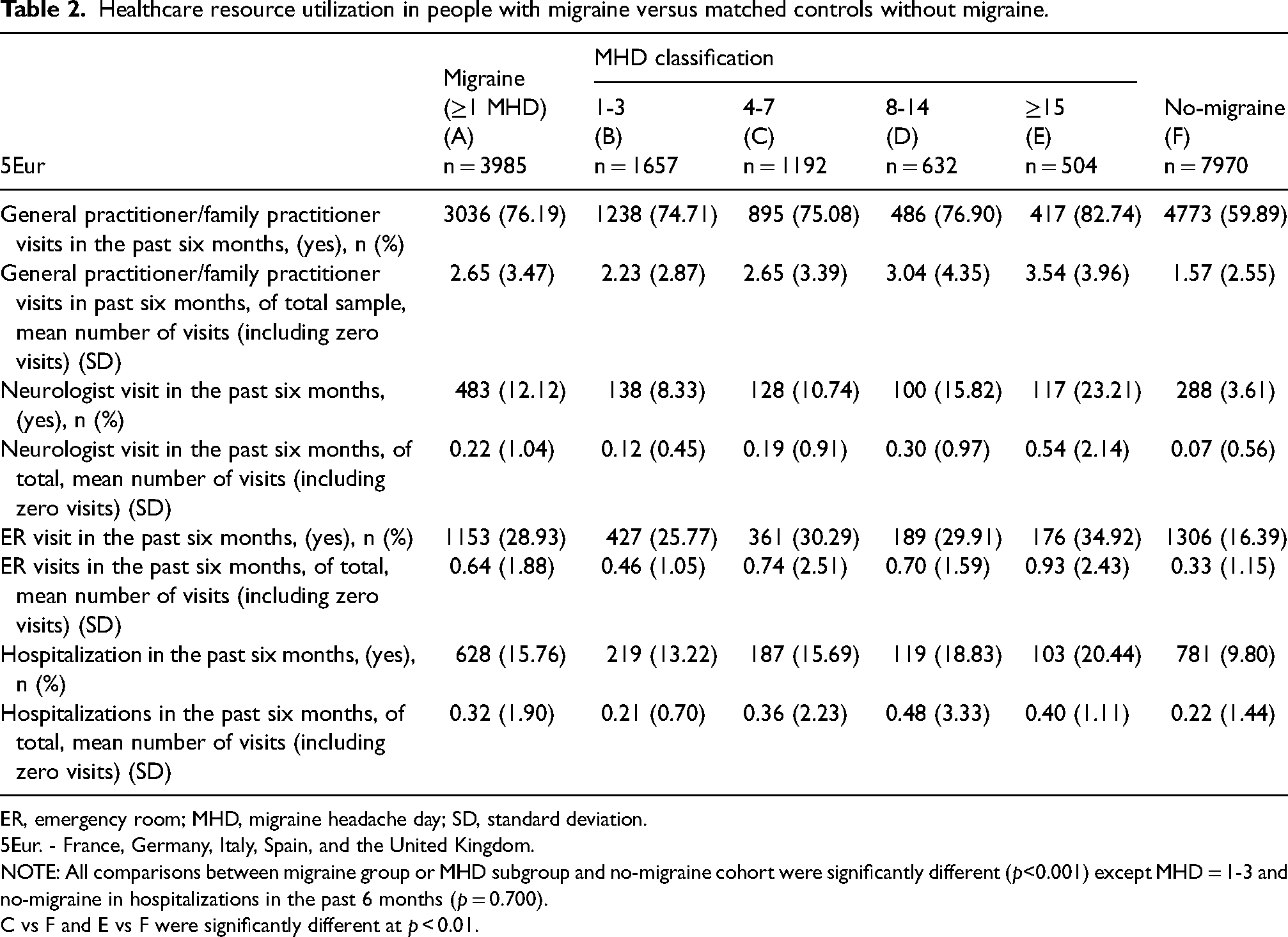
ER, emergency room; MHD, migraine headache day; SD, standard deviation.
5Eur. - France, Germany, Italy, Spain, and the United Kingdom.
NOTE: All comparisons between migraine group or MHD subgroup and no-migraine cohort were significantly different (p<0.001) except MHD = 1-3 and no-migraine in hospitalizations in the past 6 months (p = 0.700).
C vs F and E vs F were significantly different at p < 0.01.
Comparison by MHD categories
Significant decreases in all the HRQoL scores including MCS, PCS, EQ-5D, and EQ-5D VAS were reported across MHD subgroups with respect to the frequencies of MHDs, compared to PwoM (p ≤ 0.001 for all; Figure 2). PHQ-9 scores were significantly higher (worse depression) across MHD subgroups (MHD 1–3: 7.55 ± 6.06; MHD 4–7: 9.33 ± 6.42; MHD 8–14: 9.70 ± 6.55; MHD ≥15: 11.80 ± 7.40) compared to PwoM (6.07 ± 5.96; p ≤ 0.001 for all). The proportion of respondents experiencing mild, moderate, moderately severe, and severe depression was significantly higher across all MHD subgroups irrespective of the migraine frequency (p ≤ 0.001 for all; Figure 3). Similarly, all WPAI measures were significantly higher across MHD subgroups irrespective of the migraine frequency, compared to PwoM (p ≤ 0.001 for absenteeism, presenteeism, total work impairment, and activity impairment for all subgroups; Figure 4). A significantly higher proportion of health care visits, including GP/FP, ER, and neurologist and hospitalization, were also observed across the MHD subgroups compared with PwoM (p ≤ 0.001 for all). The number of healthcare visits (GP/FP, ER, and neurologist) and hospitalizations in the past six months were significantly higher across the MHD subgroups compared to PwoM (p < 0.05 for all), except for mean number of hospitalizations in the migraine (1–3 MHD) cohort (p = 0.700; Table 2).
Comparison of migraine with Rx use versus no-migraine cohort
Results of the sensitivity analysis, which matched and compared those with diagnosed migraine who reported using a Rx versus a no-migraine cohort, were consistent with the primary findings (Online Supplementary Material)
Discussion
This retrospective cross-sectional survey reported significant burden of migraine in terms of worse HRQoL, more severe depression, decreased work and activity productivity, and higher HCRU in respondents who experienced ≥1 MHD compared to matched controls without migraine in 5Eur. using the 2020 NHWS. Study findings demonstrated incremental burden across migraine subgroups (1–3 MHDs, 4–7 MHDs, 8–14 MHDs, and ≥15 MHDs) irrespective of the use of Rx for migraine compared to the matched PwoM.
Results from the propensity score matching based on demographic, clinical, and health characteristics reported significantly lower HRQoL among PwM vs. PwoM, in line with previously published European-based studies (27,28). Specifically, MCS and PCS scores of migraine respondents were significantly lower than PwoM (p < 0.001) with an incremental difference of 4.2 and 3.2, respectively. These results are greater than the previously reported MCID of 3 (29). There was a difference of 0.1 points reported for EQ-5D between the migraine and no-migraine respondents, greater than the MCID of 0.074 points, indicating a clinically meaningful difference (21).
Previous studies have established a strong association between migraine and depression (30–32). This study reported a significantly higher level of depression based on PHQ-9 scores among PwM compared to PwoM. These results agreed with the higher prevalence of depression among PwM than PwoM, with no significant association between the severity of depression and prevalence of migraine (33). However, the relationship between migraine and depression is reported to be bidirectional and unequal (32,33). Hence, it is crucial for HCPs to acknowledge the high prevalence of depression in patients with migraine in order to provide effective care and understand the underlying mechanisms of migraine (32).
Since migraine often affects people during their peak productive years, it can impose a significant decrease in their social functioning and work productivity (7,34,35). This study indicated a significant impact of migraine on work productivity with higher scores of absenteeism, presenteeism, and productivity impairment (p < 0.001 for all scores) in employed PwM than PwoM, which concurs with previous research (7,36). Migraine-related productivity loss is multifactorial, characterized by several factors including pain, migraine symptoms, attack unpredictability, migraine comorbidities, emotional impact, under-diagnosis and under-management, and stigma (36). Our results may highlight the need for development and implementation of workplace programs to support people with migraine, and thereby decrease the costs of migraine-related productivity loss.
PwM also had higher levels of HCRU in terms of the number of visits to GP/FP, neurologists, ER, and hospitalizations in a span of six months compared to PwoM (12,37). Prior research has reported that even in affluent European nations, there is a low proportion of individuals with migraine who seek medical attention. Among those who do, a disproportionate number consult with specialists (38). These results further strengthen the need to improve care for people with headache in Europe, including empowering primary care providers in the management of people with migraine.
Incremental burden of migraine was evident in physical, mental, and overall health status across all subgroups (1–3 MHDs, 4–7 MHDs, 8–14 MHDs, and ≥15 MHDs). Respondents in all migraine subgroups experienced a significant decrease in productivity, likely leading to higher indirect and societal costs compared to those in the PwoM cohort. Findings on the incremental burden of migraine are in concurrence with previous European-based studies (12,16,39,40).
Respondents with migraine receiving prescription treatment reported worse HRQoL, depression, impaired work productivity, and higher HCRU than PwoM (Online Supplementary material). These findings were similar to the overall respondents who experienced migraine regardless of treatment status. Scores for burden measures worsened with increasing MHD among migraine respondents even with Rx use. The substantial disease burden in respondents with migraine despite the use of Rx corresponded with a prior Japanese study which reported a similar burden among Rx and no-Rx patients with migraine. The study also reported that patients taking Rx having worse migraine-related characteristics compared with patients currently not taking any Rx (37). These results indicate unmet needs among migraine respondents which must be considered for future development of migraine therapies.
Even though previous studies conducted in the European region reported the incremental burden of migraine, these studies used either a smaller sample size (16) or lacked the no-migraine control (12). This study used a larger sample size and reported the incremental burden of migraine across all subgroups compared to PwoM. NHWS is representative of the adult population of France, Germany, Italy, Spain, and the UK; therefore, demographics are reflective of the general migraine population in each country and correspond to prior research (3). Overall study findings emphasize the need for enhanced education, more efficient treatments, and comprehensive care to address the substantial burden of migraine on individuals and society. This involves creating more accessibility to specialized migraine care, implementing workplace initiatives to support migraineurs, and empowering primary care providers in migraine management. Future research should explore the effectiveness of newer migraine treatments (e.g., calcitonin gene-related peptide (CGRP) antibodies) in improving both migraine symptoms and associated comorbidities, impact of physician-diagnosed depression and antidepressant medication on QoL, relationship between insurance status and HCRU among migraine patients, considering the subgroup of migraine patients with chronic migraine and medication overuse for assessing the challenges and burdens faced by this population.
Limitations
There are several limitations to consider in this study. Since the data collection for NHWS is cross-sectional and self-reported via an online panel, certain biases may exist. Despite using multiple methods of administration and randomization and matching for age, sex, and diagnosis, certain populations may be underrepresented such as the individuals in the prison system, with severe disabilities, or isolated members of society, similar to other patient-reported surveys. Additionally, there is no independent verification of the reported variables such as diagnosis and medication usage through other data sources like electronic medical records or physician reports. With NHWS being self-reported, recall bias and false reporting (intentional or unintentional) may occur resulting in inaccuracies in data collected. While the NHWS provides valuable insight, a longitudinal study would be necessary to determine the bidirectional effects of the variables examined. With cross-sectional data, causality cannot be inferred from the study results, and certain types of variables cannot be evaluated. Moreover, there was lack of control over the timing of survey completion, potentially introducing variability in responses; individuals experiencing a migraine attack at the time of completion might have reported worse outcomes compared to those who reported during the interictal phase without headache.
Conclusion
Those with diagnosed migraine who had at least one MHD in the past month reported worse productivity, QoL, depression, and increased use of HCRU when compared to a matched sample without migraine. These findings highlight the need for effective management strategies for individuals with migraine to minimize the impact of the disease on their daily lives and overall well-being and to reduce the societal and healthcare burden of migraine.
Article highlights
People with migraine had significantly lower health-related quality of life, increased work productivity loss and higher healthcare resource utilization compared to matched controls without migraine.
Incremental burden was observed across migraine subgroups (1–3 MHDs, 4–7 MHDs, 8–14 MHDs, and ≥15 MHDs) irrespective of the use of prescription medication compared to the matched controls without migraine.
Supplemental Material
sj-docx-1-cep-10.1177_03331024241276415 - Supplemental material for The incremental burden and healthcare resource utilization among people with migraine in Europe: Insights from the 2020 European National Health and Wellness Survey
Supplemental material, sj-docx-1-cep-10.1177_03331024241276415 for The incremental burden and healthcare resource utilization among people with migraine in Europe: Insights from the 2020 European National Health and Wellness Survey by Astrid Gendolla, Joshua D. Brown, Amanda R. Mercadante, Sheila Drakeley, Nikoletta Sternbach, Aaron Jenkins, Karin Hygge Blakeman and Gianluca Coppola in Cephalalgia
Footnotes
Acknowledgments
The medical writing support was provided by Sulekha Shafeeq, PharmD and Shalini Vasantha, PhD, Indegene Limited, Bangalore, India on behalf of Cerner Enviza funded by Pfizer. We would also like to acknowledge Senior Biostatistician, Halley Costantino, for her work quality checking the matched data and formulation of data output.
Author contributions
JDB, ARM, AJ, and KHB are employees of Pfizer, Inc. SD and NS are employees of Oracle Life Science, which was a paid consultant to Pfizer to conduct the study. ARM was an employee of Oracle Life Science at the time of this study. AG reports financial support for ad boards, consulting and speaker honoraria from: Grünenthal, Mundipharma, Abbvie/Allergan, Lilly, Teva, Amgen, Novartis, Hormosan, Stada, Lundbeck, Pfizer, Hexal, Esanumperfood, Medscape, streamed up, Ärztekammer Nordrhein, Ärztekammer Westfalen Lippe, DGS, Regionalbeauftragte der DMKG. GC has received honoraria for participation in clinical trials and contribution to advisory boards or presentations from TEVA, Biohaven, Eli Lilly, Abbvie, and Pfizer. He serves as an Associate Editor for Cephalalgia, BMC Neurology – Pain section, Frontiers in Neurology – Neurotechnology section, Frontiers in Human Neuroscience – Brain Imaging and Stimulation section, and on the Advisory Board of The Journal of Headache and Pain.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
The study protocol and questionnaire for NHWS were reviewed by the Pearl Institutional Review Board and were granted an exemption. Eligible respondents have given their consent to participate in the survey.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was sponsored by Pfizer Inc.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.