
Abstract
Aim
Physiotherapy interventions in migraine patients have been previously studied; however, the evidence supporting their use is still limited. In almost all the studies, migraine patients receive a standardized physiotherapy protocol, regardless of their clinical presentation and the findings of the physical assessment. The aim of this case series is to describe three patients treated with an individualized physiotherapy approach, tailored to their symptom presentation, physical assessment findings, patient preferences, migraine phase, and the overall clinical picture.
Methods
We present three patients with neck pain and migraine without aura who were treated with eight sessions of individualized physiotherapy over a 2-month period. Two of them presented with cervical musculoskeletal disorders (CMDs) without major cervical sensitization. The third one presented with only minor CMDs but had significant cervical sensitization. We describe the clinical reasoning underlying the treatment approach we used for the three patients.
Results
All three patients showed improvement in both migraine and neck pain frequency and disability that lasted over the follow-up period. The improvements matched their global impression of change ratings.
Conclusion
An individualized physiotherapy approach is underpinned by clinical reasoning and is a promising component within overall migraine management.
This is a visual representation of the abstract.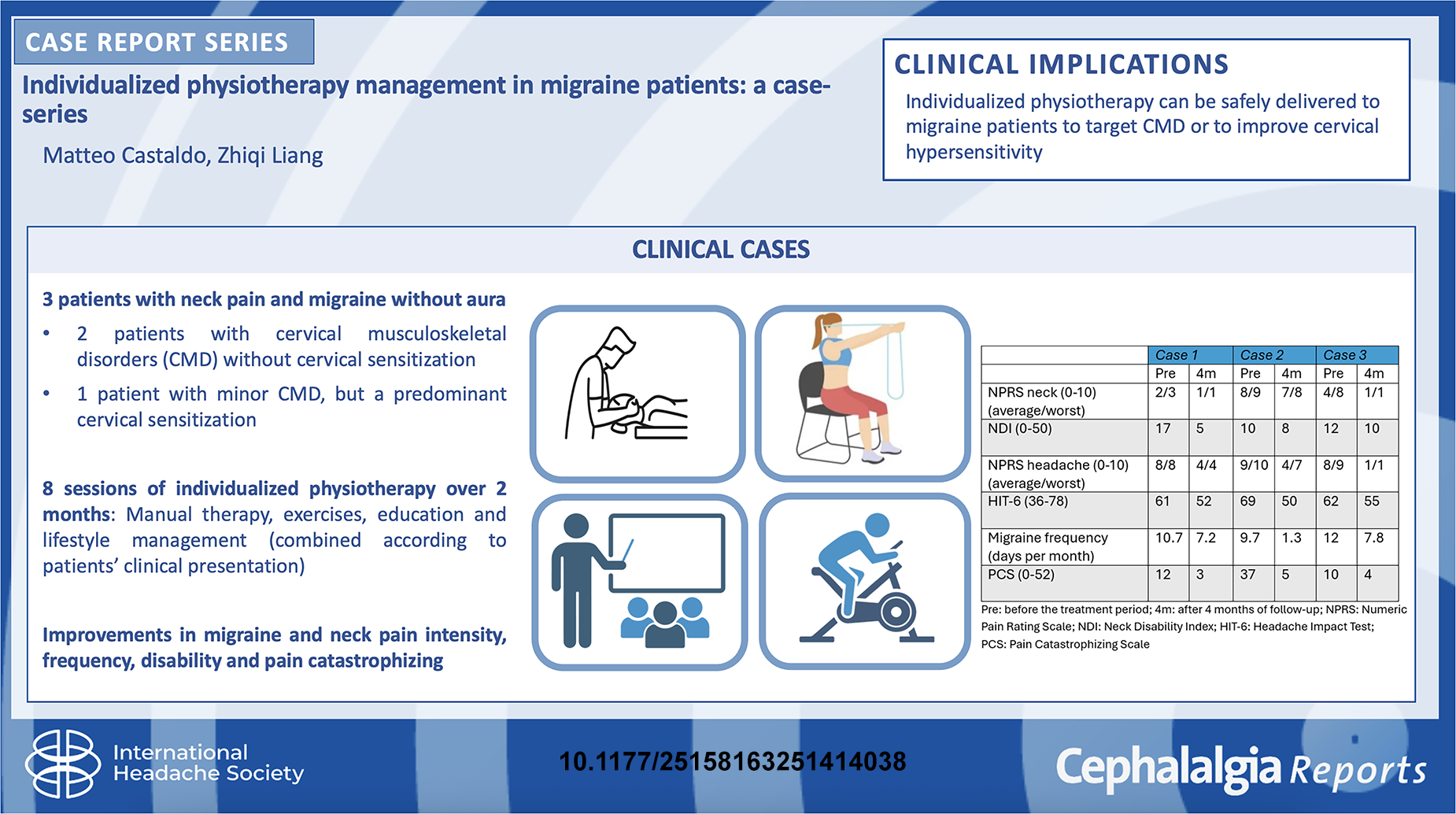
Introduction
Migraine is a heterogeneous neurological condition necessitating management that is person-centered and multidisciplinary.1 The management of migraine is mainly pharmacological, but physiotherapy is widely used.2,3 However, physiotherapy studies often deliver the same protocol to all migraine patients, regardless of the findings of the physical assessment, affecting the results.4
Neck pain is commonly reported by migraine patients but its pathophysiology and contributions to migraine are largely debated.5–7 It can be a prodromal symptom, related to cervical sensitization, or due to cervical musculoskeletal disorders (CMDs). Neck pain and CMDs do not always go together: it has been previously found that 60% of migraine patients can have neck pain but no CMDs,8 suggesting that the cause of neck pain and cervical sensitization can be migraine itself. The physical assessment aims to identify if cervical sensitization and/or CMDs are present. These findings should be evaluated in relation to any other modifiable factors contributing to migraine.
CMDs can increase nociception and peripheral sensitization to the trigeminocervical nucleus (TCN), an area in the brainstem where trigeminal and upper cervical afferents converge.9–11 This neurophysiological link explains why cervical nociception (related to CMDs) can be perceived in trigeminal regions where patients usually experience migraine pain. CMDs cause pain and disability due to impaired cervical musculoskeletal function.12 Therefore, the aim of the physical assessment is to determine the functionality of the musculoskeletal system through a comprehensive examination that includes active movements, manual examination of both joints and myofascial tissues, neuromuscular function, and the neural system. Full details of the physical assessment can be found elsewhere.13,14 Identifying CMDs in migraine can be challenging as cervical sensitization is heightened in some individuals, even during interictal periods,8,12,13 causing neck pain and migraine-like symptoms to be easily reproduced during movements, exercises, and palpation even in the absence of CMDs.8 Physical findings should be interpreted in relation to the overall clinical picture, and if impairments are not just associated with pain and are consistent across movement, articular, and neuromuscular tests, and they correspond to neck pain symptoms and disability reported by the patient, then treatments to address these impairments driving peripheral nociception and sensitization should be prioritized, using appropriate manual therapy techniques as well as specific exercises.
On the other hand, if CMDs are minor or not present, interventions should prioritize addressing central mechanisms of migraine through other modifiable contributors, such as education about their condition and self-management strategies, general exercise, and lifestyle modifications,13,14 all of which can also decrease cervical sensitization if present. For example, myofascial impairments alone (e.g. increased tone, decreased flexibility, trigger points) are unlikely to explain the extent of neck pain reported by some patients as purely related to CMDs, and are more likely indicative of cervical sensitization. Manual therapy can provide short-term pain relief and help reduce cervical sensitization in some cases through pain modulatory mechanisms, but this should align with patient preference and clinical findings of symptom reduction during assessment.
Thus, physical examination to determine the presence of CMDs and cervical sensitization is crucial for understanding the real cause of the neck pain and to identify if the neck contributes to the migraine experience, thereby indicating specific intervention. Alternatively, other strategies to address modifiable contributing factors to migraine should be prioritized.
Our research groups have described how patients can be sub-grouped to help clinicians prioritize treatments according to the presence or absence of CMDs and cervical sensitization.13–17 This process will be illustrated in the next section through case scenarios of three patients with episodic migraine (not under preventive medication) and neck pain who received eight sessions of individualized physiotherapy over a 2-month period as part of a feasibility study (Australian New Zealand Clinical Trials Registry: ACTRN12624000717550). The outcomes included migraine frequency (using an electronic diary), migraine pain intensity (using the Numeric Pain Rating Scale (NPRS)), neck pain intensity (using the NPRS), neck disability (using the Neck Disability Index (NDI)), headache impact (using the Headache Impact Test (HIT-6)), catastrophizing (using the Pain Catastrophizing Scale (PCS)), and global impression of changes. All patients were independently classified as migraine according to International Classification of Headache Disorders (ICHD)-3 criteria18 by two physiotherapists having experience in headache management, using headache features reported by the patients on an online screening survey. Patients not matching the ICHD-3 criteria for migraine were excluded. All patients had also been diagnosed with migraine previously by their general practitioner and or neurologist, to rule out the presence of other primary or secondary headache forms. The presence of other headache forms was an exclusion criterion. For the writing of the manuscript, the CARE reporting checklist has been used.19
Results
Case 1
A 47-year-old woman presented with episodic migraine and neck pain that worsened in the last 4 years due to high stress and sleep problems.
She reported that neck pain was both a migraine prodromal symptom and a trigger; when neck was strained during exercises or prolonged postures, a migraine attack can develop afterward. Physical examination revealed that a CMD was present, and the extent of impairments strongly correlated with her neck pain symptoms and neck functional limitations. No excessive cervical sensitization was detected, as the pain responses during provocative maneuvers in the physical examination were in proportion to the impairments. Therefore, specific treatments to address a CMD was prioritized, using specific manual therapy techniques and neck exercises (including retraction mobility, deep neck flexor, and neck extensor motor control and strengthening), as she was already engaging with aerobic exercises regularly, to target her musculoskeletal impairments. Each session included manual techniques to improve pain and cervical joint mobility, such as posterior–anterior mobilization of the upper cervical spine motion segments, myofascial tissues treatment, side-bending, and rotation mobilization of the mid-cervical spine, traction, and upper cervical flexion. Neck exercises to improve cervical mobility, neuromuscular control and strength were also reviewed and progressed. As the patient wanted to have more information on migraine, its relationship with neck pain, and self-management strategies, individualized education focusing on these aspects was provided. The education was provided both during the manual treatment, including explanations of goals in using pain-free as well as pain-provoking techniques, and with a slide presentation at the end of each treatment session focusing on migraine pathophysiology, individuals’ thresholds for triggering attacks, the TCN, potential contributions of the CMDs, personality characteristics, stress management strategies such as mindfulness. Each session lasted 40 min (one per week), adjusted in a dynamic way according to her clinical presentation (e.g. if she was in the prodromal phase or during a migraine attack, all treatment techniques were pain-free, aimed at diminishing migraine symptomatology).
She had reduced musculoskeletal impairments with long-lasting improvement of neck pain intensity and functionality, headache intensity, and disability, matching her impression of improvement (see Tables 1 and 2).
Baseline characteristics of the three cases.
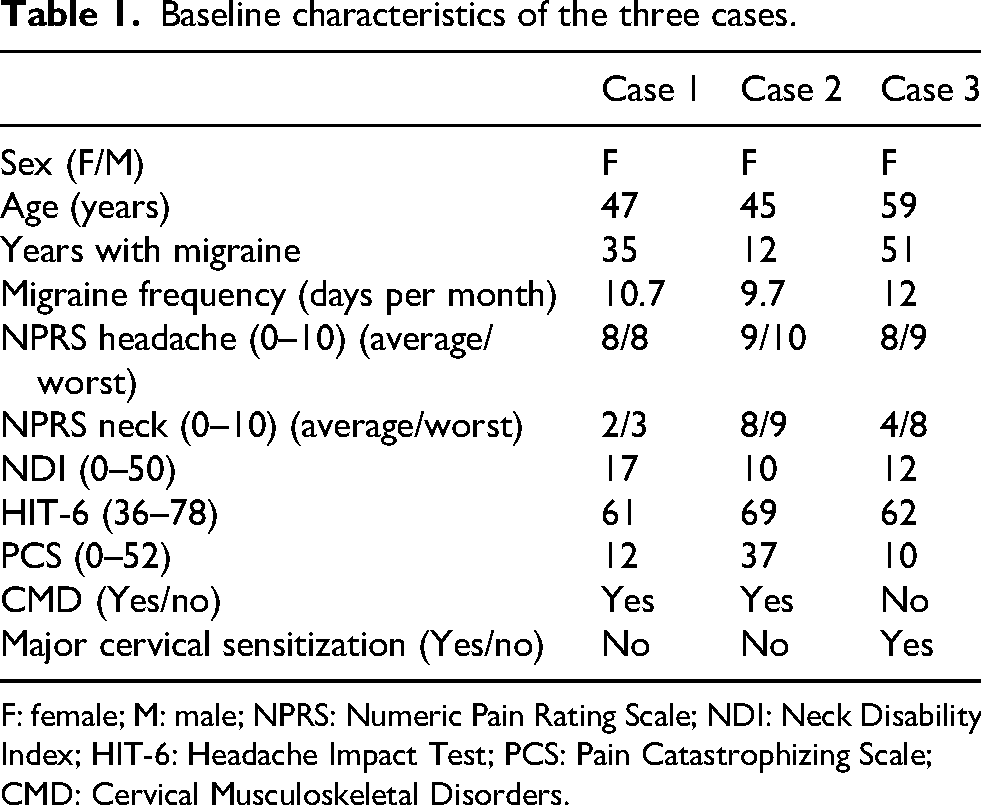
F: female; M: male; NPRS: Numeric Pain Rating Scale; NDI: Neck Disability Index; HIT-6: Headache Impact Test; PCS: Pain Catastrophizing Scale; CMD: Cervical Musculoskeletal Disorders.
Post intervention changes.

Post: end of the treatment period; 4 m: after 4 months of follow-up; 7 m: after 7 months of follow-up; NPRS: Numeric Pain Rating Scale; NDI: Neck Disability Index; HIT-6: Headache Impact Test; PCS: Pain Catastrophizing Scale; CMD: Cervical Musculoskeletal Disorders.
Case 2
A 45-year-old woman presented with episodic migraine and neck pain. She reported suffering for many years (>10 years). In the last year, migraine attacks worsened with accompanying neck pain.
Similar to case 1, she also reported neck pain being both a prodromal symptom as well as a trigger of migraine attacks. During initial assessment, a CMD was also detected and strongly correlated with her clinical presentation, without prominent cervical sensitization. Therefore, specific treatments to address the CMD using manual therapy (see description of manual therapy in case 1) and neck exercises (addressing mobility, and neuromuscular control of deep cervical muscles) were prescribed to target the physical impairments underlying her functional limitations.
In addition to neck-directed treatments, case 2 was also provided with specific education to address pain catastrophizing beliefs. She reported not being able to exercise due to migraine and showed a high score (37 points) on the PCS. Explanations to her included an analogy about the sensitized brain being an “overprotective” brain that can trigger migraine attacks at lower thresholds, that movement and exercise are both safe and beneficial, and that gradual progression of exercise can increase the threshold for exercise-induced migraine attacks, as well as information on the TCN and the role of CMD in her condition. These led to an improvement in PCS score and increased active engagement in aerobic exercise that made her more confident and empowered (“yesterday I pushed really hard in the gym, expecting a migraine attack but it did not come”).
One of case 2’s treatment sessions was 12 h into a migraine attack that was attributed to prolonged neck postures. She was afraid that the migraine attack could worsen with any assessments or treatments to the neck, but it was explained to her that the goal of the session was to reduce her symptoms by applying pain-relieving manual therapy techniques (such as general traction, upper cervical spine traction, retraction, posterior–anterior mobilization of the spine). The techniques were selected and modified according to her immediate symptom responses throughout the session, always aiming to provide optimal symptom-relief and avoid any aggravation. Manual treatment to improve the range of motion due to her CMD was also performed, such as intervertebral mobilization in side-bending and rotation. None of the eight treatments (40 min each, one per week) worsened her headache and she reported that her migraine headache resolved immediately and did not return the same evening or the next day following treatment during the attack.
She had long-lasting improvement in neck pain intensity, headache intensity, and disability, and in PCS, matching her impression of improvement of the overall condition, neck pain and functionality, and headache symptoms (see Tables 1 and 2).
Case 3
A 59-year-old woman presented with episodic unilateral migraine and daily neck pain. She started experiencing a worsening of her migraine frequency a year ago and increasing neck pain and sleep problems (1–2 h sleeplessness per night). On the other hand, she reported neck pain not being related to migraine, and in the first session she frankly admitted she was there just because she worked on the University campus, not expecting any improvement in migraine with physiotherapy.
The physical assessment showed only minor CMD, but prominent signs cervical sensitivity. This was reflected by the absence of musculoskeletal impairments such as passive joint hypomobility. Instead, there was generalized hypersensitivity to neck movements and typical migraine-like pain was reproduced with manual palpation to cervical tissues. She had migraine symptoms on the day of initial assessment, which immediately improved with symptom modifying tests (axial traction, passive retraction), indicating that treatments similar to those tests were likely to have pain modulatory effects on her symptoms. Based on her presentation, improving cervical hypersensitivity was prioritized using education, lifestyle management, mindfulness, and non-specific manual therapy and exercises. Treatments were not primarily aimed at targeting CMD impairments, but manual techniques (such as headache reproduction-modulation, myofascial tissues stimulation) were aimed at reproducing headache-like pain, to activate pain modulatory pathways. An important component to engaging this patient with physiotherapy management was forming a therapeutic alliance through discussion of treatment goals and what physiotherapy could offer. Specifically, that physiotherapy can help identify and address modifiable factors contributing to her condition and provide pain relief through pain modulation via the TCN.
The patient presented during a migraine attack on the second session, which was relieved by manual therapy treatment (in particular with upper cervical spine traction and flexion, retraction, and general traction) and reduced her usual intake of non-steroidal anti-inflammatory drugs in that day and in the following ones, demonstrating how neck treatments could be beneficial for her. Her attitude toward physiotherapy became more positive thereafter and she actively engaged in general exercise and lifestyle modifications which further improved her condition. She also received eight sessions, lasting 40 min each, one every week.
She had a long-lasting improvement in neck pain intensity, headache pain intensity and disability, and in PCS. She changed her beliefs about managing migraine, neck pain, and physiotherapy. This matched her overall impression of improvement, neck pain, disability, and headache symptoms (see Tables 1 and 2).
Discussion
We reported on three patients with different clinical presentations and different physiotherapy treatment priorities. In all three, there were promising improvements in both neck and migraine symptoms, with all patients obtaining >50% reduction in neck and migraine pain intensity, and a reduction in headache frequency (one patient achieving the threshold of >50% of reduction of migraine days)20 in the short- to mid-term. Neck disability also improved, reaching the minimal clinically important difference of >5.5 points reduction21 at some of the time-points. Only in case 3 the maximum reduction was 5 points, slightly less than the cut-off of 5.5 points: however, being the baseline score 12 (in the higher range of mild disability) and the reduction at the score of 7 or 8 in the lower range of mild disability, this could partially be related to a floor effect. Headache impact reached the minimally important changes of 2.5 points22–23 at some of the time-points. It is important to highlight that some of these data showed a fluctuation at the different time-points and did not follow a linear trajectory of improvement, with case 1 showing an initial worsening in PCS followed by an improvement, and case 2 showing an initial improvement in the NDI then increasing almost to the starting score. However, the baseline scores were fairly low (in the moderate or mild ranges), indicating that catastrophizing and neck disability were not the major issues for those patients, and that possibly was present a floor effect.
Positive results are captured by the global impression of change, in which all patients reported improvement at all time-points. Although headache frequency is the recommended primary outcome measure by the International Headache Society, patients with migraine have individualized preferences for a range of short- to long-term outcomes in both migraine and neck pain when attending physiotherapy.24 These results support that applying clinical reasoning to prioritize treatments according to the key aspects of the patient presentation, thereby individualizing management, should be the goal of physiotherapy interventions in migraine. Even when no CMD is present, there can be a role for neck treatments, albeit with different priorities and rationales underlying how and why a technique is applied. Education tailored to the individual, including aims and rationale for physiotherapy interventions, is also essential.
These findings should be interpreted with caution, as this is a small case series with only 7 months of follow-up for some and not all outcome measures, and each patient had a different trajectory in the changes of the NDI, PCS, HIT-6, and NPRS scores. Migraine frequency at 7-month follow-up was not collected, as this was not part of the study protocol. The generalizability of these findings is limited, as this is a small uncontrolled case series, but still supports the role of detailed assessment and clinical reasoning to target peripheral versus central mechanisms, which is not only feasible but necessary for individualized management. Larger clinical trials using this individualized management approach are needed to corroborate our findings, as larger prior physiotherapy trials apply standardized protocols without tailoring of treatments to underlying mechanisms, possibly affecting the results as some interventions were delivered but not a priority in all patients (e.g. delivering manual therapy and exercises when CMD is not present and such treatments not needed).25 Further, a person-centered, individualized approach may be more effective also for enhanced patient engagement, empowerment, and increased self-efficacy.14,24 The individualization of education aligned with these aspects, as the experience and understanding of migraine is highly variable across patients.
Conclusion
An individualized physiotherapy approach is underpinned by clinical reasoning and is a promising component within overall migraine management and should be considered when designing randomized controlled trials studying physiotherapy interventions in migraine.
Clinical implications
Individualized physiotherapy treatments can be safely delivered to patients with migraine.
The therapeutic benefit of physiotherapy interventions depends on the clinical reasoning and the individualization of the treatments, including education and lifestyle management.
Manual therapy and exercises can be used to either target cervical musculoskeletal impairments related to a CMD or improve cervical hypersensitivity through pain modulation.
Footnotes
Acknowledgments
The authors thank all participants and Professor Julia Treleaven and Dr Lucy Thomas for their intellectual contributions and support to the present paper.
Ethical considerations
The project was approved by the local ethic committee and registered in the Australian New Zealand Clinical Trials Registry (no. ACTRN12624000717550).
Consent to participate
All patients included in the study agreed to participate and signed an informed consent.
Consent for publishing
All authors (MC and ZL) agree to publish the article with Cephalalgia Reports.
Author contributions
MC and ZL cooperated in the design of the study. MC has also been delivering physiotherapy sessions to patients included in the study, and ZL made a first interview and assessment with all included patients. Both MC and ZL were actively engaged in writing, editing, and formatting the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the International Headache Society (IHS) Allied Specialties Scholarship 2024.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from Zhiqi Liang upon reasonable request. The data are stored in the University of Queensland’s Research Data Manager (UQRDM) and subject to UQRDM’s access conditions.