
Abstract
Background
In Eastern Europe, migraine imposes a substantial yet heterogeneous burden, ranking second among neurological disorders in disability-adjusted life years (DALYs) according to Global Burden of Disease (GBD) estimates.
Methods
To capture context-specific challenges, we conducted a regional case study with experts from Moldova, Ukraine, Romania, and Serbia, analysing epidemiology, healthcare organization, barriers to care, access to medications, education, awareness, and advocacy.
Results
Despite established primary care systems and neurological expertise, migraine care relies heavily on specialists, leaving diagnostic and treatment gaps at the primary level. Access to therapies is uneven: while analgesics and triptans are broadly available, modern options (anti-CGRP monoclonal antibodies, gepants, botulinum toxin, neuromodulation) remain restricted by cost, reimbursement, or availability. Awareness is insufficient, stigma persists, and structured education in headache medicine is scarce. Advocacy initiatives exist but remain fragmented and underfunded.
Conclusion
Migraine in Eastern Europe is prevalent but under-recognized, with persistent barriers to timely diagnosis and effective care. Addressing these gaps requires national policies prioritizing migraine, improved education and training, broader access to evidence-based treatments, and stronger advocacy. Regional collaboration, supported by the International Headache Society, offers a pathway toward equitable and modern headache care.
This is a visual representation of the abstract.
Introduction
In Eastern Europe (Figure 1), the burden of migraine is substantial yet heterogeneous across countries. According to Global Burden of Disease (GBD) estimates, migraine ranks second among neurological disorders in terms of disability-adjusted life years (DALYs) in the region. 1 Although DALY figures are similar to those in Western Europe, the real-world impact of migraine in Eastern Europe may be heightened by systemic barriers, including underdiagnosis, limited access to modern preventives, socioeconomic constraints, and urban–rural disparities in healthcare access.1,2

Eastern Europe map.
The global age-standardized prevalence of migraine reached 14,246.5 cases per 100,000, marking a 1.6% increase since 1990. Migraine is most prevalent in adults aged 20–59 years, ranking as the second leading cause of neurological DALYs in this age group. It disproportionately affects women, with a female-to-male ratio of 1.62, indicating that women are 62% more likely to experience migraine than men. 3
In
In
In
In
Taken together, these findings illustrate the considerable yet variably quantified burden of migraine across Eastern Europe, with both shared and country-specific challenges shaping clinical care and public health priorities.
Methodology: To address the limited comparative data on migraine care in Eastern Europe, neurologists and headache specialists from the Republic of Moldova, Ukraine, Romania, and Serbia contributed structured national analyses. Each author independently reviewed national sources and clinical practice frameworks over a three-month period (May–August 2025), drawing on published studies, national reports, locally presented data, and specialist clinical expertise. Country-specific information was organized across predefined domains: epidemiology, organization of services, barriers to care, availability and access to evidence-based treatments, education and training of healthcare providers, public awareness, advocacy initiatives, and future priorities. The individual reports were subsequently synthesized to identify shared regional trends as well as country-specific characteristics influencing migraine care. A narrative literature search was conducted using PubMed/MEDLINE, Google Scholar, and national databases. Search terms included: “migraine,” “headache services,” “access to care,” “treatment gap,” “CGRP,” and country names (“Moldova,” “Romania,” “Serbia,” “Ukraine”). Reference lists of relevant papers and national neurology/headache society documents were also screened. Publications in English and local languages were considered. This narrative consensus approach allowed integration of published evidence and real-world clinical practice insights to characterize the current landscape of migraine care in the region and to identify opportunities for improvement in health policy, clinical practice, and professional education.
Ethics: No patient-level data were collected, and ethical approval was not required
Organization of services
In Eastern Europe, the organization of migraine care follows a broadly similar model, with general practitioners or family doctors acting as the first point of contact. Patients presenting with headaches are initially evaluated in primary care, and those with suspected migraine or severe and refractory forms are referred to neurologists, most often in outpatient clinics or hospital departments. Hospital admission is generally reserved for acute debilitating attacks or complications. However, within this common framework, each country demonstrates specific features that shape access and quality of care.
In
In
In
In
All four countries have established clinical guidelines for migraine management, and all have adopted nationally available translations of the International Classification of Headache Disorders, 3rd edition (ICHD-3). These guidelines are implemented in routine neurology practice and incorporated into professional training. In contrast, guidance for other primary headache disorders may be less comprehensive or unevenly applied across the region.
Barriers to care
Despite the shared healthcare structures across Eastern Europe, patients with migraine face significant barriers in obtaining timely diagnosis and effective treatment. At the primary care level, family doctors are usually the first point of contact, but formal training in headache medicine is minimal, and diagnostic frameworks such as ICD-11 or ICHD-3 are rarely applied. As a result, migraine is often diagnosed by exclusion rather than by structured criteria, with imaging investigations overused and patient education tools, such as headache diaries, largely absent.
In
In
In
In all four countries, migraine is sometimes perceived as a stress-related or benign condition, which contributes to stigma, underdiagnosis, and delayed care. The use of non-evidence-based remedies, including herbal preparations, homeopathy, and pharmacist-recommended analgesic combinations, remains common, particularly in rural settings. These cultural perceptions and therapeutic practices may postpone consultation with headache specialists and initiation of guideline-based treatment.
In all four countries, migraine care is primarily neurologist-led, with limited involvement of other allied health professionals in routine headache management. Nurse practitioners do not have an independent clinical role in headache care, and structured nurse-led headache services are not established. Psychologists and psychiatrists are involved mainly in cases with comorbid anxiety, depression, or chronic pain, but formal multidisciplinary headache clinics are uncommon. Access to psychological services is frequently limited, and referrals are often constrained by availability, cost, or long waiting times. Overall, multidisciplinary models of care remain underdeveloped across the region.
None of the four countries currently has dedicated tertiary paediatric headache centres; however, paediatric patients with complex or refractory headache disorders are typically managed within paediatric neurology departments in tertiary hospitals.
Telemedicine is not formally implemented for headache or migraine care in the four countries. Remote neurology consultations may occur informally in isolated situations (e.g., phone or electronic communication between patients and providers), but structured telemedicine platforms, reimbursement pathways, and dedicated tele-headache programs are not currently established. As a result, telemedicine does not play a routine role in migraine management across the region.
Together, these barriers highlight the complex interplay of systemic, economic, geographic, and sociocultural factors that hinder migraine care in Eastern Europe. Despite differences in context—such as war-related disruptions in Ukraine, financial constraints in Moldova and Romania, or regulatory prescribing limits in Serbia—common challenges include inadequate training at the primary care level, insufficient access to specialists, lack of reimbursement for modern therapies, and persistent stigma. Addressing these barriers will require coordinated policy, education, and advocacy efforts to improve equity and quality of migraine care across the region.
Availability and use of evidence-based treatments
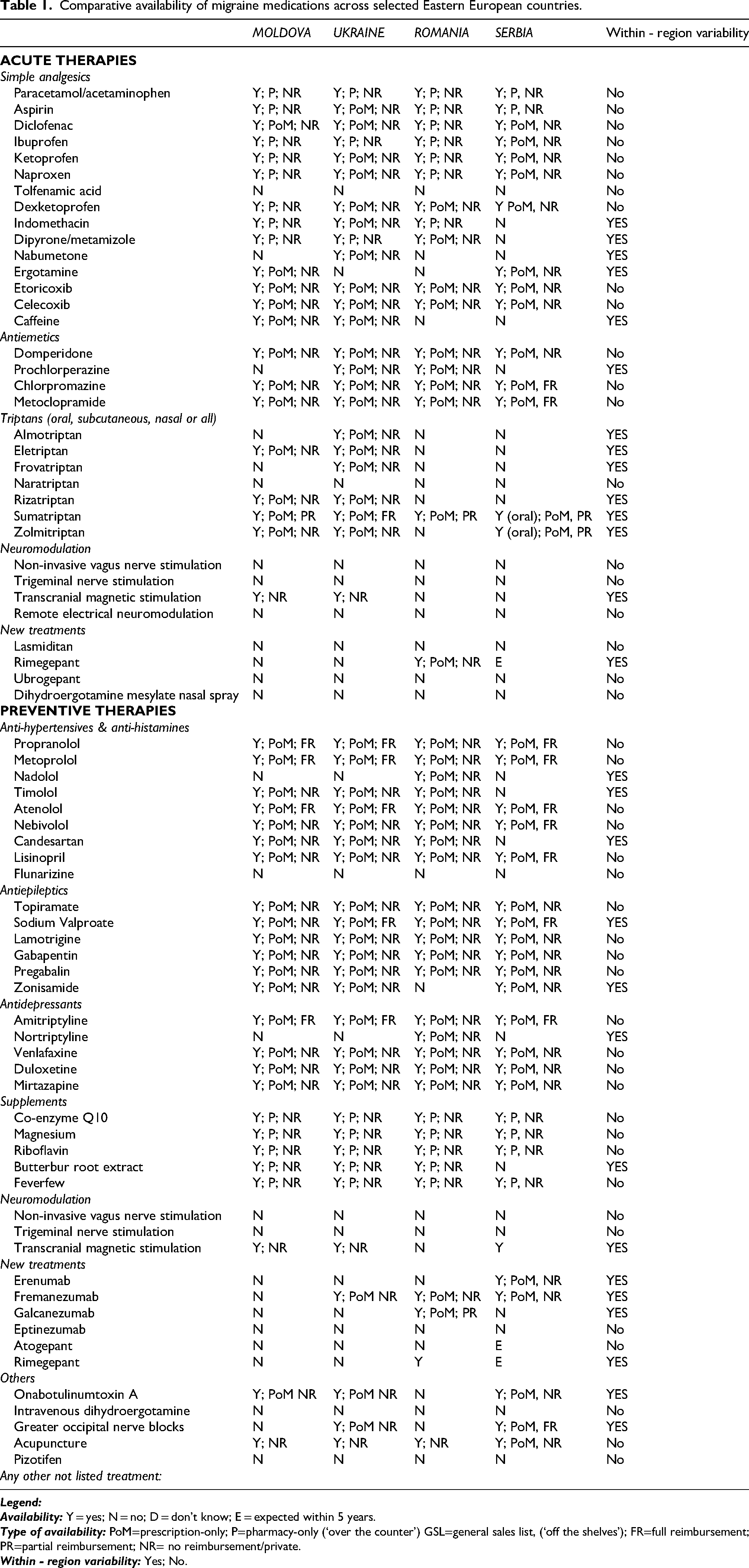
In Eastern Europe, evidence-based migraine treatments are formally available, yet their utilization remains uneven and constrained by fragmented reimbursement systems, geographic disparities, and limited neurological workforce capacity. As part of this work, we conducted a structured analysis of the availability of acute and preventive medications in line with current international clinical practice recommendations22,23 and based on the comparative framework proposed by the International Headache Society (IHS). 24
All findings from this analysis are summarized in Table 1, which provides a comparative overview of availability and accessibility across the region.
Comparative availability of migraine medications across selected Eastern European countries.
In
In
In
In
Taken together, these findings show that while essential analgesics and some triptans are widely available across Eastern Europe, significant gaps persist in access to migraine-specific and preventive therapies. Reimbursement limitations, high out-of-pocket costs, and uneven distribution of modern treatments such as anti-CGRP monoclonal antibodies or botulinum toxin A mean that many patients remain undertreated. This patchwork availability underscores the need for harmonized national policies, broader reimbursement schemes, and integration of evidence-based guidelines to ensure equitable migraine care in the region.
Education in migraine
Education in migraine and other headache disorders across Eastern Europe remains limited, both in undergraduate medical training and in postgraduate specialization. In most countries, headache disorders are covered only briefly in medical school neurology curricula, typically integrated into general lectures on neurological diseases. Exposure during residency is more substantial but often oriented toward life-threatening or more visible conditions such as stroke or epilepsy, leaving migraine underemphasized. Dedicated headache subspecialty training and formal certification are lacking across the region. Continuing medical education (CME) is provided sporadically through national conferences, symposia, and occasional workshops, but headache medicine is rarely prioritized compared with other neurological topics.
In
In
In
In
Overall, migraine education in Eastern Europe is fragmented, underdeveloped, and heavily reliant on individual societies or international initiatives. The lack of structured national curricula and certification frameworks represents a major barrier to strengthening capacity in headache medicine. Building coherent educational strategies, supported by professional networks and international collaboration, remains a key priority for improving migraine care across the region.
Advocacy and initiatives
Public advocacy for migraine and other headache disorders across Eastern Europe has expanded unevenly, with most initiatives emerging only in the past decade and varying widely between countries. At a societal level, migraine is still frequently underestimated and perceived as a “common” rather than a disabling neurological disease, which contributes to its low prioritization in national health strategies. Large-scale, coordinated national campaigns remain rare, but important steps have been taken through the efforts of professional societies, specialized centres, and patient organizations.
In
In
In
In
Taken together, these examples show that while advocacy is still at an early stage in the region, the last few years have seen increasing professional and patient involvement. Sustained, nationwide efforts will be essential to overcome stigma, strengthen patient advocacy, and integrate migraine into broader public health agendas.
Future directions
Future strategies to improve migraine care in Eastern Europe must address gaps in education, access to treatment, infrastructure, and advocacy. A common priority across the region is to enhance headache training at all levels of medical education, including undergraduate curricula, residency, and continuing medical education, while creating pathways for specialized certification. Expanding the workforce with clinicians trained in headache medicine is critical, particularly for rural and underserved areas. Another shared priority is the integration of modern, evidence-based therapies into reimbursement schemes to reduce inequities in access. Investment in public awareness campaigns is needed to combat stigma and elevate migraine as a legitimate public health concern. Finally, digital health, telemedicine, and artificial intelligence hold promise for bridging geographic barriers, supporting diagnosis, and personalizing treatment.
In
In
In
In
Overall, future progress in Eastern Europe depends on aligning education, reimbursement, and innovation with international standards, while tailoring strategies to local healthcare realities. A coordinated regional effort—integrating clinical, policy, and technological innovations—offers the best path to narrowing disparities and reducing the migraine burden in this part of Europe.
Additional suggestions
The International Headache Society and the global headache community have a pivotal role in supporting countries in Eastern Europe to overcome structural, educational, and resource-related barriers to optimal headache care. Across the region, shared priorities include the expansion of education and training opportunities, improved access to evidence-based treatments, and greater advocacy for the recognition of migraine as a public health priority. Collaborative initiatives at both regional and global levels can foster sustainability and equity in headache care.
In
In
In
Collectively, these measures—education, research collaboration, guideline dissemination, advocacy, and equitable access—would strengthen local health systems and ensure that advances in headache medicine are implemented in diverse healthcare contexts, reducing disparities and improving outcomes for patients in Eastern Europe.
Strengths: This work provides a unique regional perspective on migraine care across four Eastern European countries, integrating national data, expert clinical insight, and health-system context. To our knowledge, this is the first structured comparative analysis from this region describing organization of care, treatment access, education, and barriers in real-world practice. The involvement of headache specialists from each country ensures that the findings reflect local clinical realities and health-system constraints, supporting relevance for policy, clinical practice, and future regional initiatives.
Limitations: This analysis draws primarily on previously published national data and reports, complemented by expert clinical insight from each participating country. Although this enhances contextual accuracy, variability in data availability, collection methods, and reporting systems limits direct cross-country comparability. In areas where granular epidemiological or health-system data were lacking, expert clinical experience was used to contextualize real-world practice. The review was narrative and non-systematic, and it did not include patient-level data or formal health-economic modelling. Despite these considerations, combining published evidence with specialist input provides a comprehensive and clinically meaningful overview of migraine care in Eastern Europe.
Conclusion
Across Eastern Europe, migraine remains a highly prevalent but under-recognized neurological disorder that imposes a significant individual and societal burden. Despite the presence of well-structured primary care systems and established tertiary neurological expertise, headache care in the region continues to rely heavily on neurologists, leaving large gaps in diagnosis and management at the primary care level. Access to migraine-specific therapies is limited: while analgesics and triptans are available in all four countries, modern treatments such as anti-CGRP monoclonal antibodies, gepants, botulinum toxin, and neuromodulation remain restricted by cost, reimbursement policies, or lack of availability.
Public and professional awareness of migraine is still insufficient, perpetuating stigma and delaying diagnosis and effective care. Educational opportunities in headache medicine for both general practitioners and neurologists remain fragmented, with limited structured training or certification programs. Patient advocacy initiatives are emerging, but their reach is variable and often underfunded. (Table 2)
Comparison of migraine management across selected Eastern European countries.

*Workforce numbers are approximate, based on national neurology workforce reports, professional society estimates, and regional expert knowledge. Figures for Ukraine reflect pre-war estimates; current availability is impacted by conflict-related displacement and resource limitations.
Taken together, these shared challenges highlight the need for national policies that recognize migraine as a major public health priority, supported by improved education, broader access to evidence-based therapies, stronger advocacy, and the integration of digital health solutions. Regional collaboration, reinforced by the International Headache Society and the global headache community, can play a key role in addressing disparities, fostering knowledge exchange, and accelerating progress toward modern and equitable headache care in Eastern Europe.
Article highlights
Migraine care in Eastern Europe is mainly delivered by general practitioners and neurologists within general healthcare systems, while specialized headache centres remain limited across the region, including in Romania and Moldova. Regional priorities focus on strengthening headache education for healthcare professionals and improving the affordability and accessibility of migraine-specific treatments, particularly highlighted in Ukraine and Romania. Successful initiatives include the translation and joint implementation of ICHD-3 in Romania and Moldova, partial reimbursement of therapies in Ukraine and Romania, and the development of tertiary headache centres in Serbia. Advocacy and awareness efforts by national societies and patient organizations (e.g., Romania, Moldova, Serbia) are reducing stigma, promoting education, and supporting the adoption of modern treatment strategies.
Footnotes
Acknowledgements
The authors thank the national headache societies and clinical collaborators from Moldova, Ukraine, Romania, and Serbia for their contributions to data collection and regional insights. No external funding was received for this work.
Consent to participate
Not applicable for this review.
Consent for publishing
The authors consent to publishing the article with Cephalalgia Reports.
Author contributions
Conceptualization: All authors
Methodology: All authors
Writing – Original Draft: All authors
Writing – Review & Editing: All authors
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
All authors declare no conflict of interest.
Data availability statement
The data used for this article may be obtained from the authors with a reasonable request.
Open practices
Not applicable