
Abstract
Background and objectives
Headaches recur in up to 87% of migraine patients visiting the emergency department (ED), making ED recidivism a management challenge. We aimed herein to determine the role of corticosteroids in the acute management of migraine in the ED and outpatient care.
Methods
Advanced search strategies employing PubMed/MEDLINE, Web of Science, and Cochrane Library databases inclusive of a relevant gray literature search was employed for Clinical Studies and Systematic Reviews by combining the terms “migraine” and “corticosteroids” spanning all previous years since the production of synthetic corticosteroids ca. 1950 until August 30, 2014. Methods were in accordance with MOOSE guidelines.
Results
Twenty-five studies (n = 3989, median age 37.5 years, interquartile range or IQR 35–41 years; median male:female ratio 1:4.23, IQR 1:2.1–6.14; 52% ED-based, 56% randomized-controlled) and four systematic reviews were included. International Classification of Headache Disorders criteria were applied in 64%. Nineteen studies (76%) indicated observed outcome differences favoring benefits of corticosteroids, while six (24%) studies indicated non-inferior outcomes for corticosteroids. Median absolute risk reduction was 30% (range 6%–48.2%), and 11% (6%–48.6%) for 24-, and 72-hour headache recurrence, respectively. Parenteral dexamethasone was the most commonly (56%) administered steroid, at a median single dose of 10 mg (range 4–24 mg). All meta-analyses revealed efficacy of adjuvant corticosteroids to various abortive medications—indicating generalizability. Adverse effects were tolerable. Higher disability, status migrainosus, incomplete pain relief, and previous history of headache recurrence predicted outcome favorability.
Conclusions
Our literature review suggests that with corticosteroid treatment, recurrent headaches become milder than pretreated headaches and later respond to nonsteroidal therapy. Single-dose intravenous dexamethasone is a reasonable option for managing resistant, severe, or prolonged migraine attacks.
Keywords
Background
Burden of recurrent migraine
Primary headache disorders are increasingly important causes of disabling public health and socioeconomic burden worldwide (1). In the United States (US) alone, more than 30 million people suffer from migraine (2–4), and an estimated 3 million headache patients visit emergency departments (EDs) annually (4,5). Migraines are often underestimated and misdiagnosed—and thus are under- or mistreated (2,6). Migraine costs the US economy nearly $17 billion annually; direct costs are increased by incomplete pain relief, and repeated ED visits. Lost productivity due to headache accounts for the bulk of the economic burden (7,8).
Studies indicate that post-ED recurrent headaches occur within 24 hours in up to 87% of migraine patients visiting the ED (5,9–15), and more than half of these recurrent headaches are functionally disabling (14,16). Previous history of headache recurrence, longer headache duration, severe baseline pain, and persistent pain at discharge all contribute to post-ED headache recurrence (5,15). Repeated ED visits are a continuing problem in the ED setting (17), making ED recidivism a significant management challenge (17,18). Undertreated or poorly treated headaches (18), “medication-seeking” behavior (18,19), and medication overuse (17) are features associated with the ED-repeater phenotype. Lower headache recurrence rates are found to be significant measures according to patients’ self-reported satisfaction for optimum outcome (20).
Algogenic properties of neurovascular inflammation in migraine
Current evidence indicates that migraine is a neurovascular inflammatory disorder (21–23). It is a dysfunction of sensory processing of painful stimuli (24). Pain is generated either peripherally from trigeminocervical neurons through abnormal activation at primary afferents (25) or centrally due to anomalous modulation at second-order neurons (26–28). Once nociceptive primary afferent trigeminocervical systems are peripherally activated, signals travel orthodromically and neuropeptides are released onto receptors on second-order neurons of the trigeminal nucleus caudalis (23,29,30). The same peptidergic nociceptive primary afferents subserve sensory-efferent functions whereby peptides are likewise released at their peripheral perivascular terminals (30). Neuropeptides modulate neuroregulation of arteriolar vasodilation, inflammation, and smooth muscle changes (23,31). Neurally induced inflammatory discharge of algogenic pro-inflammatory mediators, plasma protein extravasation, meningeal irritation, perivascular edema, and dural platelet aggregation are inherent in animal models of trigeminal ganglion stimulation or pouring pro-inflammatory mediators over animal dura mater (23,32). Vascular and inflammatory changes follow neuronal changes (23,32,33). This complex inflammation-pain interplay is broadly termed “sterile neurogenic inflammation” (SNI) (23,32). SNI contributes to development of hyperalgesia, pain prolongation, and peripheral sensitization of polymodal receptors in animal models (23,26,34). Here, it is important to note that the SNI theory has not been shown to be significant in the human condition of migraine; differences and translational challenges in neuroethological approaches need to be considered. In addition, multiple SNI inhibitors (e.g. neurokinin receptor antagonists (35), neurosteroids (36,37)) have failed to be efficacious for both acute and preventive treatment of migraine. Among neuropeptides, a recent systematic review (38) has shown four clinical studies reporting increased calcitonin gene-related peptide (CGRP) during migraine attacks (39–42), while another three clinical studies found no difference (43–45).
Corticosteroids are the main humoral mediators of stress, and their increased secretion in response to adverse stimuli normally results in a cascade of physiological and behavioral homeostatic mechanisms (46). The term “corticosteroids” embraces two prototypic steroids, i.e. glucocorticoids and mineralocorticoids. By virtue of their physical features of lipophilicity (47–49) and small mass size (ca. 300 Da) (50,51), corticosteroids can readily pass the blood-brain barrier (47–49,52) and participate in a variety of behavioral and physiological processes, as well as taking part in their own secretion (46). In this respect, they serve as messengers between the periphery and brain, and also between the external and internal environments and the brain. Since corticosteroids act against the background of increased monoamine secretion, it is thought that they act to fine-tune the individual’s response to stress (53). Unlike the transient monoamine response, corticosteroids exert sustained actions on cellular activity and behavior, and therefore are essential for ensuring the orchestration of a coordinated adaptive response as well as “preparedness” of the individual to cope with future challenges (53).
Corticosteroids have been used as pain relief adjuvants in different neurological conditions; an adjuvant pain medication should be considered at all stages of the World Health Organization’s (WHO) pain ladder for mild to severe painful conditions (54). Corticosteroids reduce pain by inhibiting prostaglandin synthesis, which leads to inflammation, and by reducing vascular permeability that results in tissue edema (55). Exogenous administration of corticosteroids suppresses excessive stress and inflammatory response from the hypothalamic-pituitary axis (46). Steroid receptors are found in the central and peripheral nervous systems and are responsible for growth, differentiation, development, and plasticity of neurons (55). In particular, corticosteroids reduce spontaneous discharge in an injured nerve, which reduces neuropathic pain (56). Corticosteroids offer extended suppression of SNI (57) and modulate neuroplasticity, thereby reducing pain (56). Corticosteroids have long been used to manage migraine (58–62).
Aim
In this systematic review, we make a pooled analysis and critical appraisal of the published literature on clinical studies of corticosteroid treatment for migraine. Our objectives are to assess the efficacy of corticosteroid administration in the ED and outpatient clinical settings on the primary outcome of reducing headache frequency. We also compared corticosteroid administration to other standard drug regimens. Identification, screening, selection, and inclusion of clinical studies followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) procedures as described within the Methods and materials part of our study.
Methods and materials
A combination of the following search strategies using different search databases was employed to capture our topic of interest, i.e. studies on corticosteroids for migraine management.
A PubMed/MEDLINE search was employed for Clinical Studies Categories and Systematic Reviews on the PubMed Clinical Queries tool combining the terms “migraine AND corticosteroids”; the Boolean logic operator “AND” was applied to connect the two search terms. The Clinical Studies Category was selected for “Therapy,” “Etiology,” “Diagnosis,” “Prognosis,” “Clinical Prediction Guides,” and the scope of the search was made specific to “Broad” to enable sensitivity and specificity search values of 99% and 70% (63), respectively. The PubMed equivalent for this search method was “((clinical[Title/Abstract] AND trial[Title/Abstract]) OR clinical trials as topic[medical subject headings (MeSH) Terms] OR clinical trial[Publication Type] OR random*[Title/Abstract] OR random allocation[MeSH Terms] OR therapeutic use[MeSH Subheading]).” A second PubMed/MEDLINE search was employed for Clinical Studies Categories and Systematic Reviews on the PubMed Clinical Queries Tool combining the terms “migraine AND corticosteroids.” The Clinical Studies Category was selected for “Therapy,” and the scope of the search was made specific to “Narrow” to enable sensitivity and specificity search values of 93% and 97% (63), respectively. The PubMed equivalent for this search method was “(randomized controlled trial [Publication Type] OR (randomized [Title/Abstract] AND controlled [Title/Abstract] AND trial [Title/Abstract])).” A third PubMed/MEDLINE search was employed without using the Clinical Queries Tool. Search terms used were “migraine AND corticosteroids.” Advanced PubMed/MEDLINE search was used by implementing auto-suggested MeSH Terms and Boolean logic operator “AND” as “(migraine[MeSH Terms]) AND corticosteroids[MeSH Terms].” The Cochrane Library Advanced Search strategy was used by adding the search line “Search All Text” and employing the search terms “migraine AND corticosteroids.” A Web of Science Advanced Search was employed by using the field tag “TS” for topic, the Boolean operator “AND,” and parentheses to create our query as “TS = (migraine AND corticosteroids)” on Indexes = CPCI (Conference Proceedings Citation Index), Science Citation Index Expanded (SCI-EXPANDED), Timespan = All years. Results included all languages and all document types. Unpublished studies and a relevant reference search were exhaustively conducted. This enabled us to locate and capture unpublished studies from the gray literature (e.g. conference abstracts or research letters) on our topic of interest, with the goal of elucidating the impact of unpublished studies and ultimately avoiding publication bias of negative or positive studies.
A PRISMA (64) flow diagram describing the selection method is displayed in Figure 1. An additional relevant reference search was made to extract complete previous data on corticosteroids and migraine. Scientific abstracts and several prepublication trial registries for investigations related to the research question were searched. All published studies up to August 30, 2014, were covered; this meant that all clinical studies since the production of synthetic corticosteroids were reviewed. Two authors (YWW and RPC) reviewed each abstract, and where disagreement occurred, discussion and consensus was achieved with input from the third author (AMR). Clinically relevant data, useful evidence-based recommendations, strengths, limitations, and unaddressed areas of selected studies were carefully examined in this review.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram displaying the method of how selection of studies was made.
Comprehensive summary of included clinical studies reviewed.

First author, title of article, name of journal, year of publication, and study setting are described in the first column. The second column provides important methods employed for study design. Outcomes are fully elaborated in the third column. Critical appraisals, clinical bottom lines, Consolidated Standards of Reporting Trials (CONSORT) and Jadad scale are presented in the last (fourth) column. M: male; F: female; IHS: International Headache Society; tid: three times per day; prn: as needed; IV: intravenously; ED: emergency department; VAS: visual analog scale; CI: confidence interval; OTC: over-the-counter; po: orally; ER: emergency room; GI: gastrointestinal; ARR: absolute risk reductions; NSAIDs: nonsteroidal anti-inflammatory drugs; RR: relative risk; OR: odds ratio; DHE: dihydroergotamine; AEs: adverse events.
To help interpret the results of the different studies included, the following methods were applied. For the primary outcome, i.e. frequency of headache, relative risk (RR) ratios were calculated from the numbers of headache events in the control and intervention groups of each study. Where headache recurrence was reported as a dichotomous variable (present/absent), the presence of headache was included as an event for the primary outcome. For adverse events, the number of events in each study group was scored. Absolute risk reductions (ARRs) were calculated by subtracting event rate (headache frequency) in the intervention arm from event rate in the control (or study arm not of primary interest). Numbers needed to treat (NNT) were calculated by dividing 100% by the ARR values. All published studies relevant to our question stem were included and their outcomes were completely assessed so as to avoid publication bias and selective reporting.
Results
A total of 25 studies with an aggregate number of 3989 (median age of 37.5 years, interquartile range or IQR 35–41 years; median male:female ratio of 1:4.23, IQR 1:2.1–6.14) (Figure 7(a) and (b)) patients were found under the combined search methodologies described within the Method and Materials section (Table 1). Four systematic reviews and meta-analyses were found under the Systematic Reviews search (Table 2). Two clinical studies were found from a gray literature search on conference abstracts. Fourteen (56%) studies were designed as randomized, double-blinded, controlled trials. Thirteen (52%) studies were from ED-based settings, while the remaining 12 (48%) were from non-ED-based outpatient settings. Sixteen (64%) studies applied International Headache Society (IHS) headache diagnostic criteria.
Methodological quality of included studies as assessed using the Jadad score. The Jadad score measures adequacy of reported randomization, blinding, and management of withdrawals and dropouts. Fourteen studies (56%) had a Jadad score (63) of 5, and fulfilled the complete CONSORT (64) checklist—indicating rigorous methodological quality; two studies (8%) had a Jadad score 3, and missed blinding from the CONSORT checklist—indicating adequate methodological quality; four studies (16%) had a Jadad score of 0 and did not fulfill any of the CONSORT checklist. Comprehensive summary of included systematic reviews and meta-analysis. Table 2 displays included systematic reviews and meta-analysis (first author, title of article, name of journal, and year of publication in the first column), important results of clinical relevance combined from the statistical analysis (second column), and clinical bottom lines (third column). The systematic reviews by Colman et al. and Singh et al. included the same seven randomized-controlled trials (RCTs); the former further included a meta-analysis of adverse events, while the latter provided symmetric inverted funnel plots to describe the lack of systematic difference and publication bias between the larger and the smaller study effect sizes. The systematic review by Huang et al. included one more RCT than the seven; this study added a meta-analysis elucidating the superiority of adjunctive parenteral dexamethasone compared to placebo with standard abortive therapy. The review by Neill and Brannigan further discussed the weaknesses of three selected RCTs. RR: relative risk; CI: confidence interval; ED: emergency department; IV: intravenously.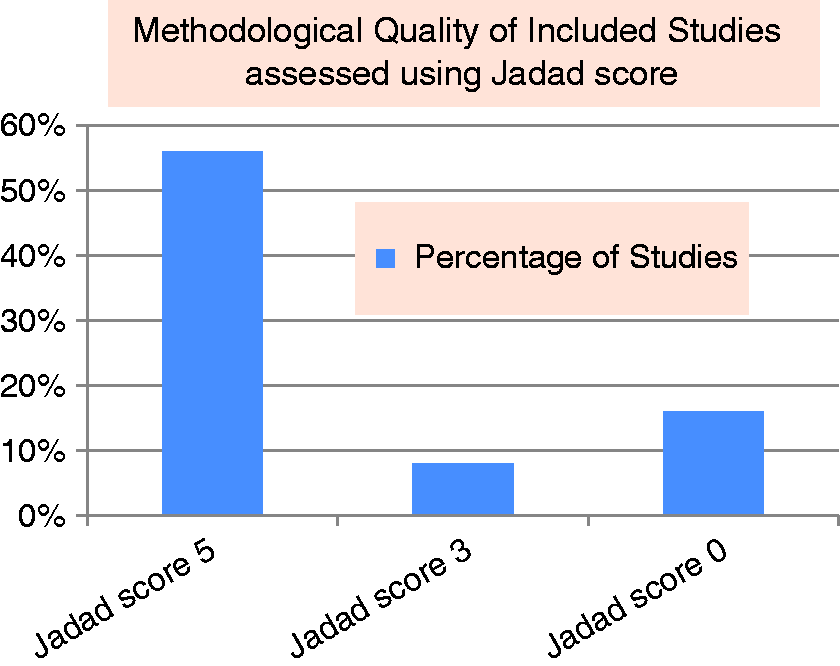

Fourteen studies (56%) had a Jadad score (65) of 5, and fulfilled the complete CONSORT (66) checklist—indicating rigorous methodological quality; two studies (8%) had a Jadad score 3, and missed blinding from the CONSORT checklist—indicating adequate methodological quality; four studies (16%) had a Jadad score of 0 and did not fulfill any of the CONSORT checklist (Figure 2).
(a) Median headache reduction (shown by horizontal dotted lines) was found to range from 30% in 24-hour to 11% in 72-hour respectively following administration of corticosteroids. Error bars indicate interquartile range (IQR) values; two studies each from both 24-hour and 72-hour comparison were found to be outliers to the IQR. (b) Similar to the results displayed on Figure 3a, the Numbers Needed to Treat (NNT) was found to be 3 for 24-hour and 10 for 72-hour headache recurrence.
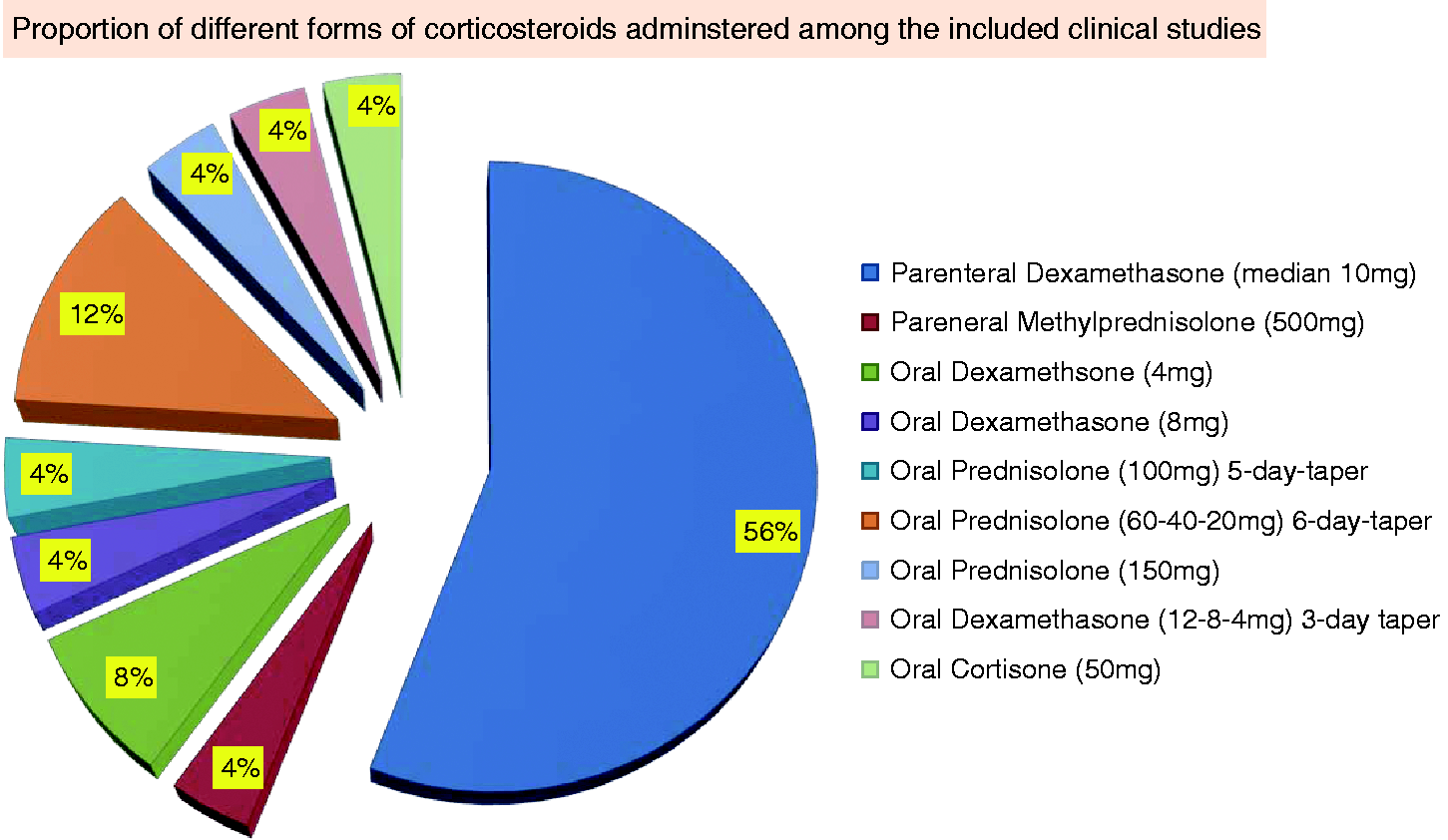
Nineteen studies (76%) indicated observed outcome differences favoring benefits of corticosteroids, while six (24%) studies indicated non-inferior outcomes for corticosteroids. Stratifying the studies to those that addressed headache recurrence (56%) and acute reduction of migraine attacks (68%), respectively, revealed that 78.6% and 61.2% of the studies observed favorable outcome differences indicating benefits of corticosteroids; 21.4% and 38.8% indicated non-inferior outcomes for corticosteroids (Figure 4). Median absolute risk reduction was 30% (range 6%–48.2%), and 11% (6%–48.6%) for 24-, and 72-hour headache recurrence (Figure 3(a)), making the NNT 3.3, and 9.1 for 24-, and 72-hour headache recurrence (Figure 3(b)), respectively. Parenteral dexamethasone was the most commonly used (14 studies, 56%) corticosteroid. Dexamethasone was administered with an average single dose of 12.8 mg (range 4–24 mg; interquartile range 8–16 mg; median 10; mode 8, 10 mg) (Figure 5). All the ED-based studies used parenteral dexamethasone, and showed favorable observed outcome efficacy of dexamethasone. One study used 500 mg intravenous methylprednisolone. Ten of the 13 non-ED-based studies administered oral corticosteroids, nine of which showed favorable observed outcome efficacy. Two studies administered 4 mg oral dexamethasone; one study used 8 mg oral dexamethasone; another study used a five-day course of 100 mg oral prednisolone; three studies used a six-day tapering course of oral prednisolone 60 mg on days 1 and 2, 40 mg on days 3 and 4, 20 mg on days 5 and 6; one study administered pre-treatment with 150 mg oral prednisolone; one study administered a three-day course of oral dexamethasone (4 mg three times per day (tid), twice per day (bid), once per day (qd) each for 1 day); and one study administered a single oral dose of 50 mg cortisone (Figure 6). Parenteral dexamethasone (56%), oral prednisolone (12%), and oral dexamethasone (8%) were the top three common steroid forms administered, in descending order (Figure 6).
Nineteen studies (76%) indicated observed outcome differences favoring benefits of corticosteroids, while six (24%) studies indicated non-inferior outcomes for corticosteroids. Stratifying the studies to those that addressed headache recurrence (56%) and acute reduction of migraine attacks (68%), respectively, revealed that 78.6% and 61.2% of the studies observed favorable outcome differences indicating benefits of corticosteroids; 21.4% and 38.8% indicated non-inferior outcomes for corticosteroids. Dexamethasone was administered with an average single dose of 12.8 mg (range 4–24 mg; interquartile range 8–16 mg, shown by error bars; median 10, shown by the dotted horizontal line; mode 8, 10 mg). Parenteral dexamethasone was the most commonly used (14 studies, 56%) corticosteroid. Oral prednisolone (3 studies, 12%) and oral dexamethasone (2 studies, 8%) were the other two common corticosteroid forms administered. (a) Median (37.5 years) and interquartile range (35–41 years) of the mean age of all participants (both sexes) within the included studies. (b) Median (1:4.23) and interquartile range (1:2.1–6.14) of Male:Female ratio among all participants within the studies included.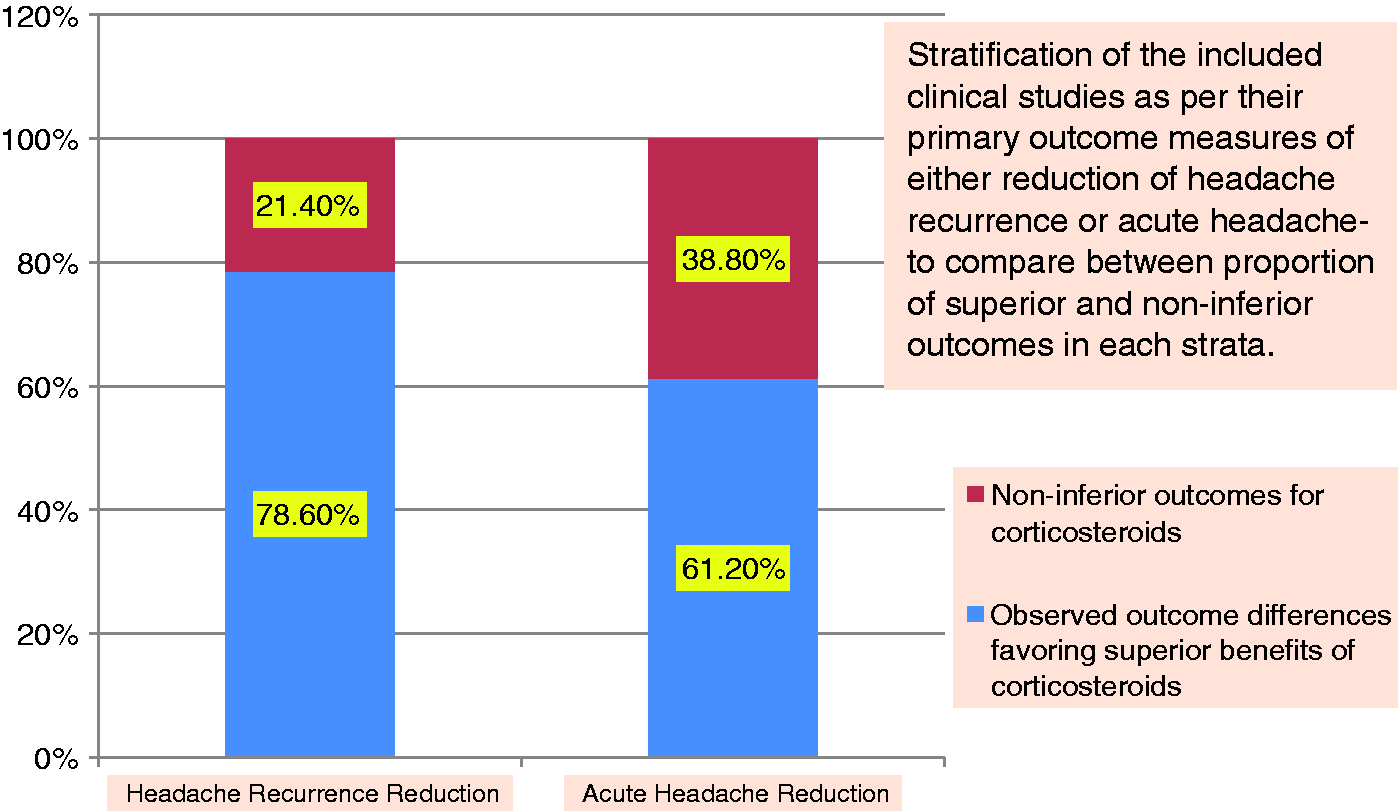


In the systematic reviews and meta-analysis appraised in this study, the objectives and inclusion criteria were clear among all. Relevant sources were searched without restriction by language or publication status. Steps were taken to minimize bias and error by having more than one reviewer independently conduct study selection, validity assessment and data extraction. Appropriate statistical methods were used to combine studies and to assess for heterogeneity and publication bias. Potential biases and sources of confounding were well addressed in the text. Although the trials were small, they were of acceptable quality and their results were consistent. All systematic reviews were well conducted and the authors’ conclusions appear reliable. All systematic reviews and meta-analyses revealed the importance of adjuvant corticosteroids to various abortive medications—indicating generalizability of results. Three meta-analyses showed that a single dose of adjuvant parenteral dexamethasone was associated with 11.1% ARR (absolute risk reduction), NNT of 9, and 26% RRR for 72-hour headache recurrence. The fourth meta-analysis indicated that parenteral dexamethasone delivered the highest efficacy. Adverse effects were tolerable.
Cumulative evidence from our systematic review shows that higher disability, prolonged migraine duration, status migrainosus, incomplete pain relief, and headache recurrence were the settings in which corticosteroids were beneficial. One study indicated that abortive medications that were ineffective prior to dexamethasone became effective subsequently (61). Among the ED-based studies, there was an increased chance of headache recurrence among patients with higher levels of pain at ED discharge than among patients with lower levels of pain at ED discharge; this may indicate that migraine attacks treated when the pain is mild are less likely to recur. One randomized double-blind study showed that adjunctive dexamethasone resulted in higher sustained relief periods as compared to triptan monotherapy (16).
Discussion
Migraine recurrence is commonly observed following “successful” ED management. Various clinical features have been associated with poor pain outcomes after treatment for headache. In the outpatient setting, a patient’s history of headache-related functional disability can be used to predict long-term medication needs prospectively and to decrease the economic burden of illness. Some ED patients cannot access neurology or headache specialty care. Timely primary care appointments can also be difficult to obtain, and ED patients frequently fail to appear for scheduled appointments. Therefore, it is important for the emergency physician to understand the magnitude of post-discharge headache and to identify which patients are most at risk. Having this information can be used to guide choice of medication, discharge instructions, and urgency of specialty referral.
During this study, we did not perform a sub-analysis of outcomes depending on the type of abortive treatment used because, in the real world, different drug combinations are often required and because all patients do not respond to a standard regimen. Lack of standardized abortive therapy could conceivably introduce a bias if one group received different treatment from another. Moreover, patients often know what agents work best for them, and physicians often have treatment preferences. We felt that mandating specific abortive therapies would make the study more complex, and would not emulate clinical heterogeneity in practice. Given the inter-study differences in design, in methodology, and in outcome and efficacy measurands, we were not able to perform statistical heterogeneity and weighted meta-analysis tests.
The fact that dexamethasone recipients suffered fewer severe recurrences and had fewer repeat physician visits (73,74,80,82) suggests that there are quality-of-life and productivity benefits to this therapy; performing formal economic analysis and demonstrating these benefits will further support this notion. While being efficacious in both situations of reducing headache recurrence and acute headache attacks, corticosteroid administration showed higher potency in the former, i.e. controlling headache recurrence (Figure 4).
Parenteral administration within the ED setting using single-dose intravenous dexamethasone at 10 mg shows adequate efficacy in controlling attacks, and transferring care to the outpatient. Parenteral administration can be useful to avoid poor drug absorption secondary to gastric stasis commonly experienced by chronic migraineurs. In the outpatient setting, six to eight short, oral, tapering courses of steroids per year with close follow-up of adverse effects shows efficacy; it is essential to note that corticosteroid administration is intended to control acute, severe attacks in an effort to smoothe transfer of care to better acute care and/or preventive management targets (92).
Being a long-acting corticosteroid with a biologic half-life of 36–72 hours (93,94), dexamethasone should effectively suppress inflammation during the period when patients are most likely to experience a headache recurrence—potentially making it an ideal agent for a one-time administration before ED discharge. At equipotent anti-inflammatory doses, dexamethasone almost completely lacks the sodium-retaining property of hydrocortisone, minimizing unwanted side effects. In our review the incidence of minor effects was rare and was similar to placebo, with no reported severe adverse reactions. That outcomes compare favorably both in the ED- and non-ED settings indicates that convenience sampling is not a likely source of confounding bias; this, in fact, further promotes the generalizability of benefits of steroids for relief of recurrent headache in both outpatient and ED settings.
It is worthwhile to differentiate migraine sufferers presenting to the ED with “the last straw headache syndrome” of consecutive bouts of headaches from those presenting with “the first or worst headache syndrome” alarming the patient and causing the visit to the ED. The former comprise the ED-frequenter migraine sufferers who have been described as sharing certain salient features of emotional decompensation, compulsive preoccupation with symptoms, and occasional manipulative behavior, besides their head pain (19). These “refractory” patients might be victims of misdiagnosis, mistreatment, undertreatment, or overmedication, while the latter present as a more challenging subset of new headache or genuine refractoriness that is difficult to manage with readily available medications. Addressing limitations of current therapy is important while monitoring refractory headaches. Reviewing treatment plans at regular visits and balancing short-term pain relief with longer-term goals of disease management needs to be emphasized. Management of expectations is an increasingly important tool in handling patients with chronic pain in both the ED and outpatient settings.
In patients presenting with frequent migraine attacks, careful selection needs to be made as to which attack to treat aggressively; this may involve less convenient but more effective non-oral medications at the cost of more side effect burden. Always observe for inadequate trial duration, inappropriate dosage and consideration of medication overuse when patients are not doing well. Using a headache calendar or diary to log headache types and frequency, treatment effectiveness, menstrual cycle, ED visits, and other health care visits are essential to the care of migraineurs, especially difficult-to-manage migraineurs.
Dexamethasone causes less fluid retention than other steroids due to the fact that it has less mineralocorticoid effect. Because these headaches often recur over the days and months following ED discharge, the responsibility of the emergency physician includes identifying as yet unmet treatment needs and ensuring successful transition of care of these patients to an appropriate outpatient health care provider. Prior to administering dexamethasone, it is important to remember the various contraindications, i.e. pregnancy, known peptic ulcer disease, diabetes, or systemic fungal infections. Clinicians deciding which medication to prescribe for recurrence can therefore be guided by considerations such as cost, contraindications, adverse effects, and a patient’s previous overall experience with the medication. Careful evaluation and management for opioid administration, barbiturate use, and stressful life events are salient features characteristic of multidisciplinary approaches toward a long-term control of prolonged and refractory migraine. Where resources are available, it is important to use existing opportunities to optimize emergency care of migraine attacks by real-time consultations between the emergency and headache specialty departments.
Steroids have been efficacious for detoxification of overused substances in patients with medication-overuse headache (MOH) (79,95). Concurrent administration of nonsteroidal anti-inflammatory drugs (NSAIDs) and steroids must be avoided to reduce potential risk of gastrointestinal bleeding. Comparison between titration versus bolus dosage of dexamethasone administration can affect headache recurrence and other outcome measures. Some of the studies reviewed herein defined headache recurrence as 24 hours after headache relief from the study drug, while others used a 48-hour or longer timepoint. Panel A (available online) provides commonly applied definitions of recurrence and efficacy measures; these terms are inter-related and their consistent use can help enhance daily practice and research methods.
Conducting mega-trials and mega-studies has its own challenges of operational limitations in organizing resources for longer durations, recruiting larger number of study patients, and securing funding. For these reasons, performing systematic reviews and pooled analysis provide perceivable options to assess accumulating evidence and aggregate data from different studies addressing similar question. Locating studies from literature database searches was the most important component while preparing this systematic review. One of the limitations we faced was the inconsistent availability of variables, and outcome and efficacy measurands across the different included studies. Future studies can benefit by providing consistently available data so that weighted meta-analysis, heterogeneity statistics, and meta-regressions can accurately be computed, and trends and interactions can easily be detected. Forthcoming studies can elucidate further on the efficacy differences between different dosages of oral and parenteral corticosteroid administration, and mixture parenteral infusions. Our recommendations include conducting full clinical studies expanding to other migraine patient populations apart from prolonged migraine attack cohorts and emergency settings.
Broader global utility
In lower-resource emergency settings or on an outpatient basis, where the burden of migraine is increasing and where triptans and parenteral infusion forms of emergency abortive headache medications (e.g. intravenous magnesium, dihydroergotamine, levetiracetam, and valproic acid) (1,96,97) are unavailable, corticosteroids provide efficacious and low-cost therapeutic options to control prolonged and highly disabling migraine attacks. Corticosteroids are readily and inexpensively accessible both in oral and parenteral forms in lower-resource clinical settings; hence, our study can be help optimize their application in a clinically relevant manner.
Conclusions
Our literature review suggests that with corticosteroid treatment for acute migraine attacks, recurrent headaches decrease, become milder than pretreated headaches and then may respond to nonsteroidal therapy. Intravenous dexamethasone provides a reasonable option for managing resistant, severe, recurrent or prolonged migraine attacks in the ED. Our recommendations are consistent with the literature review and include up to six to eight administrations of corticosteroids per year with follow-up of adverse effects. Although documented by fewer studies, we consider it is reasonable to use oral dexamethasone on an outpatient basis in similar settings. It can be beneficial to provide a one-time dexamethasone administration before ED discharge to a headache specialist for long-term management. Reasonable and achievable goals of pain reduction should be made clear to the presenting patient in the ED setting or in the office during the initial visit.
Clinical implications
Studies indicate that post-emergency department (ED) recurrent headaches occur within 24 hours in up to 87% of migraine patients visiting the ED. With corticosteroid treatment, recurrent headaches become milder than pretreated headaches and later respond to nonsteroidal therapy. Corticosteroids provide a reasonable option for managing resistant, severe, prolonged or recurring migraine attacks.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.