
Abstract
Background/Objective
Underserved populations have worse access to neurologic care and higher risk for worse headache disease burden. We embedded a neurology clinic offering headache services within a primary care clinic treating an underserved population in Boston, Massachusetts, United States. We describe the results of a retrospective review of 1439 outpatient visits during the first three years of operation.
Methods
Electronic medical record data on demographics, visit types, diagnoses, and medications were extracted and summarized from patient visits completed at the embedded neurology clinic from October 2, 2020, to January 5, 2024. We also reviewed clinic utilization and consult completion rates.
Results
Over three years, the embedded neurology clinic completed 1439 visits, of which 687 (47.6%) were new patient visits. The consult completion rate was 73.7% (244/331). Patients had a mean age of 52.1 (SD 17.5) years, were 78% women, 68% Hispanic ethnicity and 53% Medicaid/Medicare (public) insurance. The most common diagnosis was a headache or facial pain disorder (46.2%), with migraine diagnoses representing 1/3 of all new patient diagnoses. Of patients diagnosed with migraine, 26.6% were diagnosed with chronic migraine in new patient visits, 48.1% were prescribed an American Academy of Neurology guideline-concordant migraine preventive medication (1/3 of those prescriptions for a CGRP mAB or OnabotulinumtoxinA), and 52.6% were prescribed a guideline-concordant migraine-specific abortive medication (triptan, dihydroergotamine, or gepant).
Conclusion
Embedding neurologic services within community health centers is a promising model to provide access to headache care for patients from underserved populations. One-third of patients seen received a migraine diagnosis that made them eligible for targeted, disease-specific treatment. Longitudinal studies are needed to evaluate the impact of embedded clinics on migraine-related disability and healthcare utilization.
This is a visual representation of the abstract.
Introduction
Underserved populations concurrently face poorer access to medical care and a higher risk for worse headache disease burden due to environmental factors.1–3 This problem exists in all countries and all healthcare delivery systems. While the barriers to optimizing headache care differ internationally, there may be common strategies for improving headache treatment in underserved populations in line with practice recommendations.4,5 In the United States, there are notable regional and population-based disparities in access. 6 Patients who identify as Black, Hispanic, Native American/American Indian, or live in rural areas or have lowincome are less likely to be treated in neurology and headache clinics and more likely to seek care for headache in primary care and acute care settings, where migraine is less likely to be recognized and effectively treated. 3 7–10 Long-term strategies are needed to improve access and quality of headache care for underserved populations. 11
Despite having a high proportion of patients with complex medical comorbidities, community health centers (CHCs) typically do not offer specialty clinics, including neurology or headache clinics. The most vulnerable patients often face many barriers to receiving care off-site or in the hospital setting; thus, providing embedded neurology care makes headache treatment more accessible to patients.12,13 Previously, primary care physicians in our academic hospital system reported a desire for direct contact with headache physicians either by asking patient-specific questions or by embedding a neurologist in the clinic. 14 With this knowledge and our objective to improve access to neurologic care for underserved populations, we approached the leadership at Brigham and Women's Southern Jamaica Plain Community Health Center (SJPCHC), a hospital-licensed CHC in Boston, Massachusetts. Community Health Centers have operated since the 1960s in rural and urban areas of high need to provide comprehensive health services and currently provide care for 1 of 10 US residents. 15 The primary care team from SJPCHC reported a high volume of headache presentations, and concerns over a low consult completion rate, with only 1/3 of requested neurology consults completed. 16 In October 2020, we embedded our neurology and headache-specific services within the internal medicine practice of SJPCHC to improve outpatient neurologic and headache care for their patients. We previously described the establishment and early experiences of this innovative project. 16 Here, we report a descriptive analysis of the first three years of the clinic's function through patient demographics, visit types, diagnoses, and migraine-specific prescriptions.
Methods
Clinical setting
Southern Jamaica Plain and Brookside Community Health Centers are licensed by Brigham and Women's Hospital (BWH) with the mission of providing healthcare and addressing social determinants of health for a diverse population of patients, of whom a high percentage identify as Hispanic and are enrolled in public health insurance (Medicaid/Medicare). 17 The on-site departments include internal medicine, pediatrics, obstetrics/gynecology, and behavioral health. The CHC's are accessible by public transportation or within walking distance for nearby residents. Most staff are bilingual in English and Spanish and many identify as members of the patient communities the clinics treat. Video interpreter services are available on demand and are required for interactions where staff and clinicians are not proficient in the patient's preferred language. Together, SJPCHC and Brookside CHC serve 20,0000 adult and pediatric patients and complete over 100,000 patient visits per year. They are fully integrated within the larger BWH/Mass General Brigham (MGB) health system and prior to this specific embedded clinic, clinicians would typically request a neurology consultation at one of the nearby BWH/MGB Department of Neurology outpatient offices, approximately 3 km away.
Embedded neurology services
Starting on October 2, 2020, an attending neurologist with headache specialty training (AV), based at one of the nearby BWH Department of Neurology offices, conducted consultations and follow-up visits within the SJPCHC either alone or with neurology residents (including MN). Adult patients (18 or older) were referred by primary care clinicians (physicians, nurse practitioners, or physician assistants) from SJPCHC or Brookside CHC. The consultation request was made by a primary care clinician who sent an electronic message to front desk staff with the reason for the consult, along with a level of acuity (routine vs. urgent). Patients were then scheduled within the neurology clinic's timeslots (initially one full day a week in the first year and a half, then expanded to one and a half days per week to meet increasing demand). Primary care clinicians continued to have the option to place a neurology consult request in the preexisting system-wide referral system. At the time of scheduling, new patients were encouraged to be evaluated in person so that a neurological exam could be performed. Follow-up patients were given the option of a telehealth visit, with a video visit preferred. Telephone visits were permissible if video visit was not possible (i.e., due to barriers in internet access, patient age, or cognitive ability). The neurology services were entirely embedded into the preexisting SJPCHC facilities and operations of the Internal Medicine practice. Upon check in, patients would have vitals checked and medical assistants would review and offer vaccinations as part of the primary care check-in process. During patient visits, the electronic medical record (EMR) was utilized by staff and clinicians to access health information, write patient notes, enter ICD-10 billing diagnoses and order medications. New specialty specific procedures were integrated into the health center's framework for the administration of onabotulinumtoxin A for chronic migraine, nerve blocks, and the prescription of CGRP inhibitors (not previously prescribed at this site). Both general neurology and headache specialty diagnoses and treatment were provided. Referral to subspecialty outpatient neurology clinics within our healthcare system was made for complex patients (i.e., patients with refractory to multiple antiepileptic drugs) or if it was felt that patients would benefit from comprehensive clinics (i.e., neuroimmunology clinic).
Data extraction and review
Electronic medical record data on demographics, insurance status, and ICD-10 billing diagnoses made during visits were extracted from patient visits completed at the embedded neurology clinic within SJPCHC from October 2, 2020, to January 5, 2024. Variables of interest were extracted from the EMR into an Excel spreadsheet by JR. The data were deidentified, stored in a secure server, and analyzed by AV using SAS Software, version 9.4. All data that were recoded (diagnoses that were categorized or medications that were classified by medication type) were double-checked by MN. The study was approved by the Institutional Review Board at BWH.
We created summary tables to describe characteristics of the patient population, the type of clinic visit, and the diagnoses made. Data from the first patient visit were used to report patient demographic characteristics. Gender, race, ethnicity, and preferred language were self-identified by patients. Missing data are noted in table legends. For continuous variables (such as age), mean and standard deviation were presented, otherwise summary data were presented in counts and percentages. To summarize the types of diagnoses encountered, individual visit diagnostic codes (which were ICD-10 billing codes) were reviewed by two neurologists (AV and MN) who agreed on the neurologic subspeciality classification (i.e., headache, cognitive, neuromuscular). A non-neurologic/other category included unspecified paresthesias, gait impairments due to orthopedic causes, or symptoms directly attributable to another medical illness—e.g., hypoglycemia from diabetes. All diagnoses billed for during the visit were recorded, which may have resulted in multiple diagnoses for one patient. Diagnostic codes were also reported if a routine preventive vaccine was administered during the neurology visit.
Results
Clinic utilization and visit types
Over the first three years of the embedded neurology clinic's function, there were 1439 visits, of which 687 (47.6%) were new patient visits. The mean number of visits per patient was 2.25 (SD 1.80). Of the patients who had follow-up visits, 334 (44.4%) had one follow-up visit, 163 (21.6%) had two follow-up visits, 102 (13.5%) had three follow-up visits, and 153 (20.3%) had four or more follow-up visits. Few patients seen in follow-up (1.3%) had 10 or more follow-up visits over three years. The number of total visits increased each year (408 visits in year 1, 449 visits in year 2, and 582 visits in year 3). The percentage of follow-up visits also increased each year (40.4% year 1, 53.7% year 2, and 59.5% in year 3) (Figure 1). Most visits were conducted in-person (78.4% overall, 86.7% new patient visits, 70.4% follow-up visits) (Figure 1). The percentage of phone visits was higher for follow-up visits than new patient visits (comprising 25.0% of follow-up visits vs. 7.6% of new patient visits). The percentage of video virtual visits was low overall (4.9%). Review of the calendar year 2023 revealed that the utilization rate, or the percentage of consults requested and subsequently completed, was at 73.7% (244/331 new patient visits). Reason for noncompletion was equally divided between patient canceled visits (13.9%) and no shows (12.4%). The no-show rate for follow-up visits was similar to new patient visits (12.3%).

Annual visit volumes were: 408 visits (40.4% follow-ups) in year 1, 449 visits (53.7% follow-ups) in year 2 and 582 visits (59.5% follow-ups) in year 3.
Patient population
Demographic characteristics from first patient visits are reported in Table 1. Patients had a mean age of 52.1 (SD 17.5) years and 78% of patients had female sex listed. Two-thirds (68%) of patients identified as Hispanic and approximately three-fourths identified as a race other than White (Other 47%, Black or African American 14%, Declined 10%, and 1% or less for other race categories). Of those who chose other or declined to respond, 95% identified with Hispanic ethnicity. The most common languages used during medical visits were English (57%) and Spanish (42%). Over half (53%) of patients were insured by public payors (Medicare/Medicaid), and the remainder (47%) were insured by commercial insurers. Almost half of the patients (49%) lived in Jamaica Plain, where the clinic is located, or in a bordering area of Boston defined as a high priority neighborhood.
Demographic characteristics of patients evaluated in the embedded neurology/headache clinic in Southern Jamaica Plain Community Health Center during the first three years of operation.

Demographics were recorded from the EMR during the first patient visit. Gender, race, ethnicity, and preferred language are patient-identified. Data were missing for: gender (n = 181), sex (n = 14) race (n = 20), insurer type (n = 1), and preferred language (n = 3).
Counts (%) of the top ten diagnostic categories from 1585 diagnoses made during new patient and follow-up visits in the embedded neurology/headache clinic at Southern Jamaica Plain Community Health Center, October 2020–January 2024.

Diagnoses were obtained from ICD-10 codes, and patients may have had more than one diagnosis coded during a visit. There were 764 diagnoses made during new patient visits and 821 made during follow-up visits. “Other chronic pain” included chronic neck or back pain, unless there was a neurologic feature such as radiculopathy (which would then be labeled neuromuscular). Neuropathy included generalized large fiber or small fiber neuropathy (due to identifiable causes or idiopathic). A comprehensive table including diagnoses made in <2% of visits may be found in Appendix A.
Diagnoses
While a diverse range of neurological conditions were diagnosed, headache/facial pain diagnoses represented approximately half of all diagnoses (46.2% of new patient visits and 57.8% of follow-up visits) (Table 2 and Appendix A). This was followed by cognitive disorders (10.2% of new patient visits, 7.9% of follow-up visits) and non-neurologic/other diagnoses (5.8% of new patient visits, 5.3% of follow-up visits) (Figure 2 for top 10 diagnostic categories and Appendix A for a complete list of diagnostic categories).
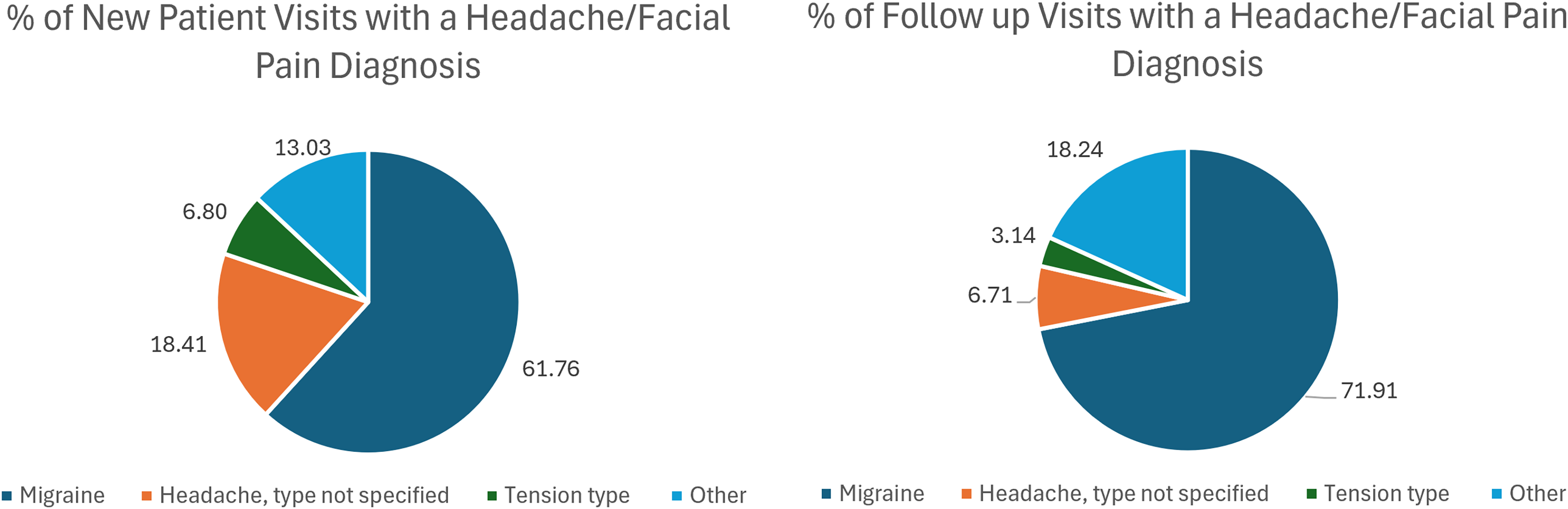
There were 353 headache diagnoses made in new patient visits and 477 made in follow-up visits. Headache diagnoses coded as “Other” were : Posttraumatic Headache (1.70% of new patient visits, 3.70% of follow-up visits), Cluster Headache (1.42% of new patient visits, 1.89% of follow-up visits), Cervicogenic headache (3.12% of new patient visits, 1.47% of follow-up visits), Trigeminal Neuralgia (1.13% of new patient visits, 2.10% of follow-up visits), Occipital Neuralgia (1.70% of new patient visits, 2.31% of follow-up visits) other headache syndrome (2.52% of new patient visits and 2.52% of follow-up visits), Other neuralgia (<1% of new patient visits, 1.26% of follow-up visits). Headache diagnoses rarely made (<1% in new patient and follow-up visits) included: NDPH, Primary stabbing headache, Hemicrania Continua, Intracranial hypotension, Nummular headache, Primary thunderclap headache, TMJD, Idiopathic Intracranial Hypertension.
Migraine was the most common headache diagnosis, representing 61.8% of headache diagnoses during new patient visits and 71.9% of headache diagnoses in follow-up visits. Non-specific headache diagnoses comprised 18.4% of headache diagnoses during first visits and 6.7% during follow-up visits. Tension-type headache was diagnosed in 6.8% of first visits and 3.1% of follow-up visits. Other headache/facial pain disorders together represented 13.0% of diagnoses during the first visit and 18.2% of follow-up visits (Figure 2 for diagnosis-level percentages). Chronic migraine represented 26.6% of migraine diagnoses during initial consults and 35.1% of follow-up visits (Table 3). Among initial visits with a migraine diagnosis, status migrainosus was diagnosed in 17.9% of visits, and intractable migraine was diagnosed 11.5% of visits (rates for follow-up visits were somewhat higher at 22.2% and 14.0% respectively). Aura was diagnosed in 17.5% of new patient visits and 9.1% of follow-up visits with a migraine diagnosis.
Migraine characteristics obtained from migraine diagnostic codes made at first patient and follow-up visits.
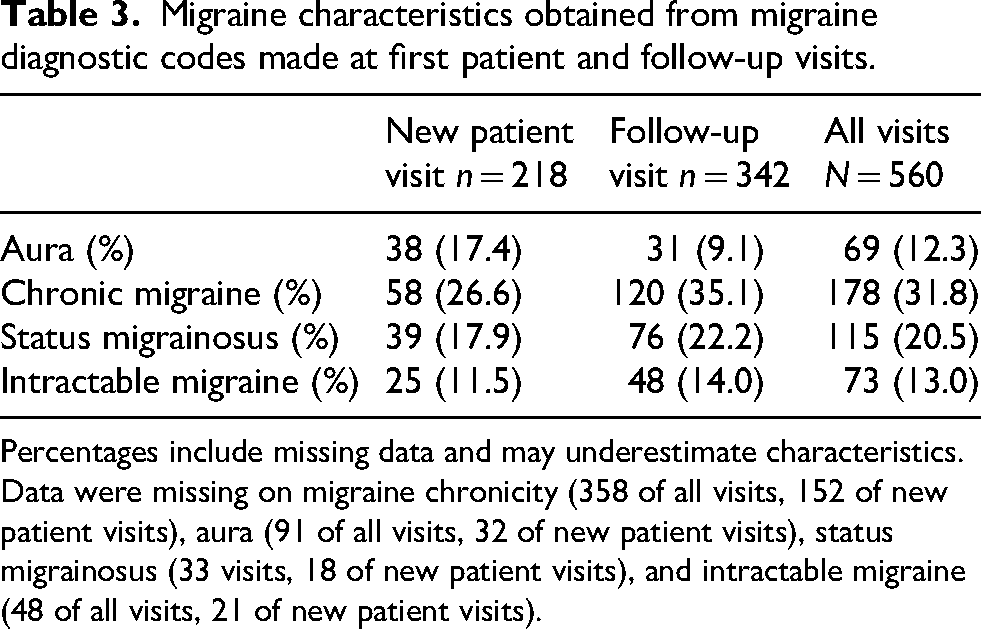
Percentages include missing data and may underestimate characteristics. Data were missing on migraine chronicity (358 of all visits, 152 of new patient visits), aura (91 of all visits, 32 of new patient visits), status migrainosus (33 visits, 18 of new patient visits), and intractable migraine (48 of all visits, 21 of new patient visits).
Medications
Approximately half of patients with a migraine diagnosis were prescribed a Level A/B efficacy migraine preventive medication not previously prescribed, with CGRP mAB or OnabotulinumtoxinA (performed at the clinic) representing 1/3 of these prescriptions (Table 4).18,19 Half of patients diagnosed with migraine (52.6%) were prescribed a migraine-specific abortive medication (triptan, DHE, or gepant), with sumatriptan prescribed to 37.2% of patients with migraine
Counts (percentages) of 266 patients with migraine receiving newly prescribed migraine preventive and abortive medications, alongside referent AHS/AAN level of evidence and Massachusetts public payor (MassHealth) insurance access information.
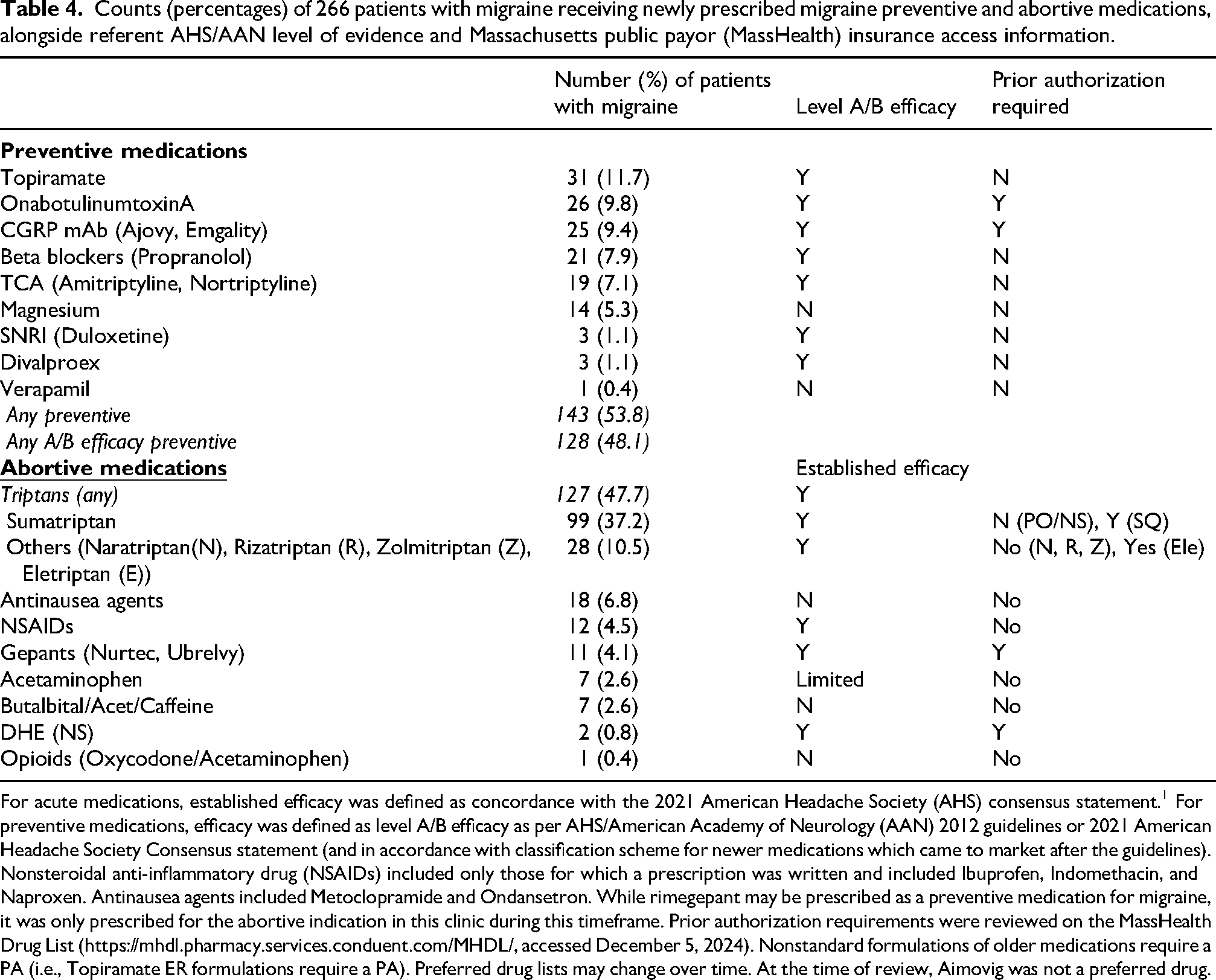
For acute medications, established efficacy was defined as concordance with the 2021 American Headache Society (AHS) consensus statement. 1 For preventive medications, efficacy was defined as level A/B efficacy as per AHS/American Academy of Neurology (AAN) 2012 guidelines or 2021 American Headache Society Consensus statement (and in accordance with classification scheme for newer medications which came to market after the guidelines).
Nonsteroidal anti-inflammatory drug (NSAIDs) included only those for which a prescription was written and included Ibuprofen, Indomethacin, and Naproxen. Antinausea agents included Metoclopramide and Ondansetron. While rimegepant may be prescribed as a preventive medication for migraine, it was only prescribed for the abortive indication in this clinic during this timeframe. Prior authorization requirements were reviewed on the MassHealth Drug List (https://mhdl.pharmacy.services.conduent.com/MHDL/, accessed December 5, 2024). Nonstandard formulations of older medications require a PA (i.e., Topiramate ER formulations require a PA). Preferred drug lists may change over time. At the time of review, Aimovig was not a preferred drug.
Discussion
We describe the first three years of patient visits from an innovative and generalizable embedded neurology clinic within a primary care setting in Boston, MA, USA, with a high proportion of patients from underserved populations. Previous synchronous neurology-primary care visits have been successfully piloted to improve access, but to our knowledge, our embedded clinic is the first model describing high utilization, diagnostic specificity for primary headache disorders, and utilization of migraine-targeted treatments for underserved populations in this setting. 13 Our data demonstrate the feasibility of this model through high visit completion rates, high diagnostic specificity for headache disorders, and access to migraine-specific medications for patients within their medical home.
Clinic utilization and visit types
The clinic was well utilized and facilitated access to neurology consultation, as demonstrated by the high completion rate for new consults (double of that previously reported for off-site, within system neurology consults), an annual increase in visit volume and percentage of follow-up visits, and a no-show rate lower than that reported for general neurology and headache clinics.20,21 This is notable because half of our population are insured by public insurance (Medicare/Medicaid), which has been associated with higher risk of no-show. 21 Our impression is that integration within a CHC optimizes utilization by addressing population-specific barriers in accessing care. The bilingual staff at SJPCHC, many of whom share identities with the patient population, create a culturally competent and welcoming clinical setting. Easy accessibility to video interpreters on-site is important for specialists who lack fluency in the patient's primary language. The location of the health center makes it accessible for many patients to walk or use public transportation. If needed, providers or patients could request assistance for transportation (such as vouchers for ride-share or medical transportation services) or other social determinants of health needs through embedded clinic resources.
Consistent with prior studies in underserved populations in neurology, telehealth visits were more likely to be conducted by phone (rather than with video).22,23 In addition to the slower escalation in video visits during the initial years of the clinic's formation during the COVID pandemic, language barriers (i.e., need for interpreter services, apps not initially translated into Spanish), patient age, lack of access to high-speed internet, and patient difficulty in finding a private or professional appearing space to conduct a video visit were likely contributors.
Patient population
Our data on ethnicity and race reflect the health centers’ patient population and include a high proportion of patients who identify as Hispanic, prefer to speak Spanish during medical visits and are insured by public payors. 17 These demographics contrast with the primarily non-Hispanic White populations treated in tertiary headache clinics in the United States. 24 The percentage of women seen at the embedded neurology clinic (78%) was similar to that reported in tertiary headache settings (71–87%) and higher than general outpatient neurology clinics.25–27 The high percentage of women may be explained by both referral bias for migraine given the neurology attending was a headache specialist but may also reflect national trends of higher rates of chronic migraine in Hispanic women. 3
Diagnoses
Headache/facial pain diagnoses were the most prevalent diagnoses, with migraine the single most common diagnosis. While this is consistent with what is seen in outpatient general neurology clinics, the proportion is higher than expected. 25 This may be because the clinic was integrated within a primary care setting, in which headache diagnoses are frequently managed or because the clinic was led by a neurologist with headache specialty training, which encouraged clinic providers to make headache-related referrals. The next most common diagnoses were cognitive disorders and non-neurologic diagnoses (i.e., a patient whose gait impairment may have been attributed to hip or knee osteoarthritis).
Despite a significant amount of missing data on migraine chronicity, a chronic migraine descriptor was coded in one-quarter of migraine visits. Diagnostic specificity for headache disorders improved in follow-up visits, as would be anticipated with headache disorders which are based on retrospective patient recall. Coding of aura was less than that reported in the general population. It is possible that this was due to lower recognition of these symptoms by physician or patient due to lower medical literacy or limitations in translation services.
Nonspecific headache diagnoses at first consultation were equally distributed between chronic and episodic frequency. Not captured in this analysis were rates of imaging for headache disorders at presentation and their indications, including patient desire for imaging.
Medications
A high-level efficacy migraine preventive medication was initiated in half of patients diagnosed with migraine (Table 4).18,19 This is much higher than what has been reported in ambulatory care visits for migraine, especially for Hispanic patients. 10 Affordability, insurance coverage requiring stepwise therapy, and limited prior use of preventive medications are barriers to access to onabotulinumtoxinA and CGRP inhibitors over older less expensive preventive treatments. While prior authorization paperwork presents a barrier to headache medication access in all US clinical settings, primary care clinics are overburdened by requests for novel medications for a diverse number of chronic conditions. When we started this clinic, we made targeted 1:1 headache education efforts for on-site medical assistants preparing these prior authorizations. Since the completion of this study, the completion of prior authorization paperwork has become centralized within the institutional primary care offices which has reduced burden on clinic staff.
Similarly, half of patients with migraine received a migraine-specific abortive medication (triptans, gepants, or DHE), most commonly sumatriptan. These prescription rates are much higher than rates reported in ambulatory care settings for ethnic and racial minorities (15.3–19.4%). 10 One study of female patients treated in the Emergency Department at Montefiore Hospital in the Bronx, NY, which included a high proportion of non-White Hispanic and Black patients, reported that triptans were prescribed to <2% of the population (compared to antiemetics at 50% and nonsteroidal anti-inflammatory drugs [NSAIDs] at 34.5%), reflecting the influence of clinical care setting over prescription practices. 9 Rates for gepant prescriptions in our clinic were low (around 4%), and trend with disproportionate lower rates of gepant prescriptions for patients who are Black or Hispanic. 28 Our impression is that our low prescription rates of gepants are likely explained by insurance and financial barriers (i.e., prior authorization requirement to have ineffective documented response with at least two triptans and potential for higher copay on average than triptan). Rates of opioids and combination analgesic prescriptions were exceedingly low, in contrast to US ambulatory data. 10 This was an intentional effort by a headache-fellowship-trained neurologist, consistent with guidelines. The proportion of patients using an NSAID is an underestimate, as our methods only captured prescribed medications.
The known impact of migraine-specific preventive and abortive medications cannot be overstated. For patients initiated on a migraine-specific medication this includes an improvement in quality of life and a reduction in emergency department visits, unnecessary head imaging, and use of abortive migraine medications. 29 Initiation of cost-effective sumatriptan in patients previously not receiving triptan therapy reduces migraine-related disability and migraine-related medical and pharmacy costs.30,31 Avoidance of opioids and combination analgesic prescriptions may prevent medication overuse headache.
Model feasibility and generalizability
Embedding neurology and headache services within the SJPCHC has been a promising strategy to deliver neurology and headache specific care for underserved populations in a primary care setting. We consider our model an embedded clinic as it represents specialty services distinct from and not traditionally available in a primary care setting, such as a CHC. Our model differs from multispecialty clinics (where various specialists share office staff and resources, but not in a primary care setting) and multidisciplinary specialty clinics (designed to provide comprehensive care for a disease state).
We acknowledge that this model may have unique advantages that facilitate its implementation. One advantage of our model is that the health centers are hospital-licensed and completely integrated into a larger health system which facilitated the neurologist's contract and compensation (receiving equal compensation for services as at other outpatient neurology sites). The financial structure is overall advantageous to the health center, as the reimbursement for a specialist consultation is more favorable than a follow-up visit with a primary care clinician, and the revenue for specialty care stays within the health center. Neurologists in the US desiring to work at a federally qualified CHC will need to understand their institution's financial operations to ensure adequate compensation and revenue generation for the health center. Rural and non-academic affiliated CHCs may offer a unique opportunity to expand headache care. We recommend that individuals interested in supporting these centers establish a meaningful dialogue with clinical and administrative directors in which they discuss financial and other barriers for inclusion of a neurologist on site. In the United States, specialty services are reimbursed at higher amounts than primary care, so we have found our model to be favorable financially for the health center. Countries with national health systems may have stronger avenues of communication via shared record and referral systems which could facilitate embedded services within CHCs. Conversely, they may have lower specialist access and lower overall compensation within the public health system that may disincentive this embedded model. Low-income countries face a staggering paucity of neurologists and may need to utilize different ongoing strategies, including emphasis on education of on-site frontline clinical staff, support of neurology training programs, and teleneurology.32–34
On the other hand, we encountered challenges in implementation, including staff unfamiliarity with specialized headache treatments, busier clinics over time, and administrative concerns regarding transferring additional clinic sessions from the department of neurology clinics to the CHC. 16 Our physical location within the CHC allowed for formal and 1:1 education of clinicians and office staff. We also developed protocols for OnabotulinumtoxinA acquisition, transport and safety with pharmacy and nursing staff. Busier clinics are an ongoing problem, which is somewhat relieved by additional assessments by supervised neurology residents.
Oversaturation of one provider is a concern which we have attempted to mitigate through shared-care models, inclusion of supervised neurology residents as valuable team members who conduct new patient visits, creation of urgent visit slots, and referral to other neurologic subspecialty clinics for complex care management. The shared-care model includes requests for primary care physicians to refill novel migraine medications or continue an established plan for stable patients, availability for curbside consultations on an as-needed basis (which, at times, has avoided the need for a neurologic consultation), small group education on neurologic diagnoses and treatments (including by neurology colleagues), and involvement in CHC meetings and events. We also worked with on-site administrative staff to create new visit types to facilitate scheduling (i.e., urgent slots and procedure visit). We initially review schedules/urgent patient requests weekly with a designated staff member, who became familiar with typical time needs for procedures, etc. and provider comfort with double-booking patients. Lastly, some patients are referred to neurology subspecialty clinics or the nearby headache center, where there are more headache specialists available.
Strengths/limitations
Our study has a number of strengths. We were able to characterize clinic use over a three-year period, with thousands of visits, giving a complete picture of patient characteristics, diagnoses, and visit types and frequency. Clinic procedures ensure that all visits and corresponding diagnoses are recorded. Limitations include modest amounts of missing data (such as on gender, ICD-10 code specificity for migraine descriptors), and the fact that information comes from a single CHC, which is similar to federal qualified CHCs but may differ in patient population and other aspects of care that could reduce generalizability to other settings. The SJPCHC is a hospital-embedded clinic within a large healthcare system, which may facilitate access to imaging or staff who may complete prior authorization paperwork. We also did not have data on nonprescribed NSAID use, which may provide an incomplete picture on overall medication practices. Secondary headache disorders may have not been additionally coded to the primary etiology (for example, headache attributed to a cervical dissection may have been coded as a cervical dissection for billing purposes).
Conclusion
Over three years, the embedded neurology clinic provided care in 1439 visits to patients within a CHC, which serves a large proportion of patients from underserved populations. The clinic was accessible and well utilized, with high referral completion and low no-show rates. The clinic had high diagnostic specificity for headache disorders, which represented half of the diagnoses made. The clinic provided high-quality evidence-based migraine preventive and abortive medications and avoided the prescription of nonspecific, controversial, or lower evidence medications in a patient population that is more likely to get nonspecific treatments.
Future directions include research on neurologic outcomes, impact upon primary care providers, and comparisons with other models of headache care. Long-term prospective studies may assess the impact of this intervention on patient populations (i.e., headache burden, migraine-associated disability, and satisfaction of treatment), the healthcare system (including cost–benefit analyses of use of migraine-specific treatments and acute care utilization), and primary care clinicians (neurologic diagnostic comfort and prescriptions of headache-specific treatments). Finally, comparative studies with long-standing models of tertiary headache care would inform strengths/weaknesses of each model.
Clinical implications
Embedding headache specialty services within a primary care setting may improve access and quality of care to patients with headache disorders from underserved populations.
The embedded clinic model provided high-quality evidence-based migraine preventive and abortive medications and avoided the prescription of nonspecific, controversial, or lower evidence medications in a patient population that is more likely to get nonspecific treatments.
Variations of this model may be generalizable to other healthcare settings in order to optimize headache care.
Footnotes
Ethical considerations
The study was approved by the Institutional Review Board (IRB) at Brigham and Women's Hospital.
Consent to participate
Consent was waived by the IRB.
Consent for publishing
Yes, all authors agree to publish.
Author contributions
Conceptualization by AV, MN, PM, and EL. Data acquisition and analysis by AV, JR, and MN. Manuscript and table preparation by AV and MN. Manuscript was reviewed for content and approved by all authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data used for this article was acquired through a clinical database and deidentified. Aggregate and summary data are available for review upon request.
Appendix
Counts (%) of all diagnostic categories from 1585 diagnoses made during new patient and follow-up visits in the embedded neurology/headache clinic at Southern Jamaica Plain Community Health Center, October 2020–January 2024.