
Abstract
Background
Studies reveal that migraine is often under-recognized, misdiagnosed and inadequately treated in the primary care setting.
Objective
The objective of this article is to assess primary care providers’ (PCP) knowledge and needs regarding migraine diagnosis and management.
Methods
We held semi-structured group interviews and distributed a brief questionnaire to PCPs in our hospital network. Building on the information from the interviews, we developed a comprehensive survey assessing PCPs’ knowledge about migraine. Descriptive analyses were performed.
Results
The initial interviews and brief questionnaires revealed that PCPs are aware of the prevalence of migraine but are uncertain about the details of management. Eighty-three of 120 physicians completed the comprehensive survey. Only 47% would order imaging for a new type of headache, 31% for worsening headache, and 35% for a headache unresponsive to treatment. Only 28% were familiar with the American Academy of Neurology guidelines on preventive treatment and 40% were familiar with the Choosing Wisely Campaign recommendations on migraine treatment. Just 34% were aware that opioids can cause medication-overuse headache. Non-pharmacologic treatment was not usually recommended. PCPs favored educational opportunities involving direct contact with headache physicians (56%).
Conclusions
PCPs are not universally aware of the specific recommendations for managing migraine patients. Future work should focus on innovative ways to provide decision support and education for PCPs caring for migraineurs.
Introduction
Despite the fact that migraine accounts for about 5 million to 9 million primary care office visits per year in the United States (US) (1), medical students have an average of one hour of preclinical and two hours of clinical teaching in headache (2). Once they complete medical school and residency, primary care providers (PCPs) receive little formal education on headache. PCPs have limited time with patients, and initial headache consultations are often time consuming (3). Perhaps for these reasons, studies indicate that few migraineurs are being actively managed by their PCPs (4,5). With the advent of health care reform and the changing health care environment, the medical home model, population management bundled care, and accountable care organizations (6), it is important and timely to study and implement methods to optimize neurologic care in the primary care setting. PCPs are the first line of care for illness and are typically the physicians from whom patients seek treatment for migraine (7).
Many studies suggest that migraine care provided by PCPs is sometimes suboptimal. One study showed that among 176 migraineurs in a primary care office, 105 (59.7%) were not recognized as having migraine (8). Migraineurs who consult PCPs for migraine may not receive a correct diagnosis (9) and/or may not receive adequate treatment (10). For example, a significant proportion of PCPs prescribe simple analgesics and nonsteroidal anti-inflammatory drugs (NSAIDs) for migraine (even for severe attacks), rather than migraine-specific treatments (10). Furthermore, a minority of patients who qualify for preventive treatment actually receive treatment (11,12). The average delay between migraine diagnosis and the start of preventive treatment is 4.3 years (11). In addition, about one-third of patients surveyed believed that the information PCPs provided on migraine treatment was inadequate (13). This is troublesome because satisfactory outcome at the initial consultation has been associated with an improved likelihood of effective management of migraine (4).
There have been few studies investigating how to improve migraine education in the primary care setting (14–16). In order to better design an effective educational intervention, we decided to study primary care physicians’ knowledge and perception of their needs.
Methods
The knowledge and needs assessment was conducted in two phases. First, we conducted semi-structured group interviews and administered brief questionnaires to PCPs in one internal medicine practice in our hospital network. Second, we used the information from the semi-structured group interviews to design a comprehensive survey administered to PCPs in the largest internal medicine group in our hospital network. The study was approved by the Partners Healthcare Institutional Review Board.
Study participants and settings
Semi-structured group interviews
Primary care physicians in a community hospital affiliated with a large tertiary care academic medical center were recruited for participation in the study. These physicians typically have a weekly noon conference, and we asked them to devote 15 minutes of one noon conference time to our semi-structured group interviews. All of the PCPs in attendance for the scheduled noon conference meeting participated in the interviews. We provided lunch as a token of appreciation for participation. MTM, EL and HS led three concurrent 15-minute semi-structured group interviews using a structured outline of topics for discussion (see Appendix A). PCPs were asked about their perception of knowledge gaps in migraine diagnosis and treatment, and about difficulties encountered in diagnosing and treating migraine patients. The leaders of the semi-structured group interviews recorded the responses. At the end of the interviews, PCPs completed a short questionnaire that collected background information. After the semi-structured group interviews, the moderators met as a group to review the results of the semi-structured group interviews. The first author (MTM) then reviewed and synthesized moderator comments and impressions. She sought clarification from moderators about any areas of uncertainty.
Comprehensive survey
Comprehensive survey question topics.

The survey was reviewed for clarity and completeness by two board-certified internal medicine physicians and two board-certified neurologists. An expert in survey design was consulted to help develop the survey, and to ensure that the answers to the questions could be analyzed appropriately. The survey is found in Appendix B.
The survey was distributed via email using Research Electronic Data Capture (REDCap) to all of physicians in the largest primary care office within Brigham and Women’s Hospital (17). REDCap is a secure, Web-based application designed to support data capture for research studies. The primary care practice is composed of resident physicians and attending physicians who see approximately 18,000 unique patients and 50,000 visits annually. This practice was selected for its size, the mix of attending physicians and resident physicians, and because the physicians in this practice are familiar with research investigating innovative, multidisciplinary approaches to care, including the practice of embedding subspecialists. For example, the clinic already has a diabetologist, a psychiatrist, social workers, and a clinical pharmacist. Participants were told the purpose of the study, and were informed that it had been approved by a review board. Reminder emails were sent to non-responders. As an incentive, physicians who completed the survey were entered into a raffle to win gift certificates that in total amounted to a value of $50. The survey was online for three weeks, and the PCPs received multiple reminder emails if they had not responded to the initial survey request.
Statistical analysis
Data were collected by REDCap and descriptive analyses were performed using the statistical software IBM SPSS for Windows, version 21 (18).
Results
Group 1
Semi-structured group interview results
Semi-structured group interview participants.
One interviewee did not complete the brief questionnaire so only sex, which was recorded by the moderators, is included for all 11 participants; the remaining answers are based on 10 brief questionnaires.
Group 2: Comprehensive survey results
Survey participants
Characteristics of comprehensive survey respondents.

PGY: postgraduate year.
Knowledge
Comprehensive survey results: Knowledge questions.

Questions were open ended with a place to write in the correct percentage.
NSAIDs: nonsteroidal anti-inflammatory drugs.
Half (54.2%) were aware that barbiturates cause medication-overuse headache, and one-third or less were aware that other medications including narcotics, NSAIDs and Tylenol can also cause MOH.
A total of 40.3% were familiar with the Choosing Wisely Campaign of the American Board of Internal Medicine Foundation (ABIMF) recommendations to limit opioid use and imaging in migraineurs except in particular cases; 27.8% were familiar with the Choosing Wisely Campaign of the ABIMF recommendations for prescribing preventive medications for migraine.
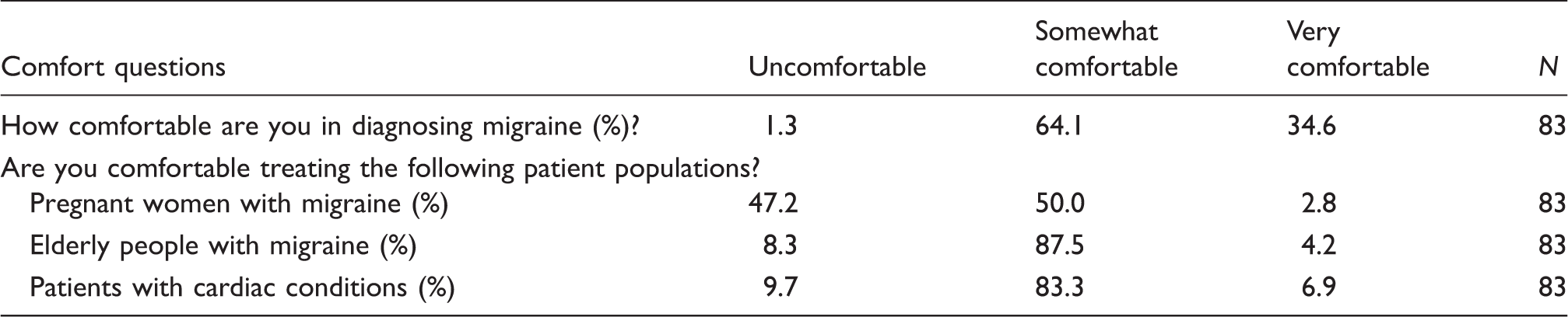
Diagnosis
Comprehensive survey results: Comfort questions.
Workup
Comprehensive survey results: Practice questions.

All of the conditions listed are generally accepted indications by headache specialists for ordering an MRI scan of the brain. MRI: magnetic resonance imaging.
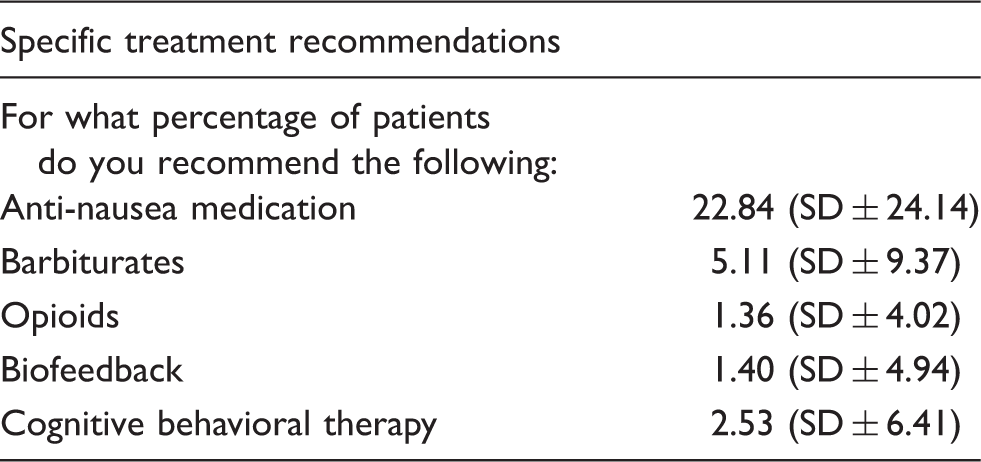
Treatment
Comprehensive survey results: Treatment recommendations.
The majority (60.16% ± 16.48%) of physicians believe that patients find their treatment for migraine effective.
Education
Comprehensive survey results: Educational opportunities for improving migraine knowledge.

Discussion
In this detailed examination of PCPs’ migraine knowledge and needs assessment, several themes emerged. 1. PCPs know that migraine is prevalent, that MOH exists and that depression and anxiety are comorbid conditions. 2. Even physicians practicing in a top academic medical center have gaps in their knowledge. For example, many were not familiar with the indications for ordering an MRI scan of the brain, with medications that cause MOH or had incomplete knowledge of evidence-based non-pharmacologic treatments for migraine. 3. PCPs were unfamiliar with the AAN/American Headache Society guidelines and the ABIMF Choosing Wisely recommendations. 4. They prefer educational mechanisms targeted at increasing contact with neurologists and headache specialists.
The semi-structured interview discussion revealed that PCPs generally think that they are comfortable diagnosing and managing migraine but that after delving into specific issues, they become less comfortable. Their knowledge base is limited. This informed our design of the comprehensive survey. The following discussion highlights the areas of discrepancy between PCPs’ beliefs and knowledge and the evidence-based guidelines/generally agreed on expert recommendations.
In the comprehensive survey, close to four-fifths of PCPs had said that they had made a diagnosis of MOH. Yet, only about half (54%) were aware that barbiturates cause MOH and only about one-third (34%) were aware that narcotics cause MOH despite the fact that these two classes of medication are the biggest culprits for MOH (20).
PCPs stated that about a quarter of migraineurs have depression and about a quarter of migraineurs have anxiety. Yet only about 50% of PCPs in the comprehensive survey assess for anxiety and only about 60% of PCPs in the comprehensive survey assess for depression in their migraine patients. This is problematic because it is thought that there is a bidirectional relationship between migraine and depression and anxiety (21). Presumably, treatment of their psychiatric comorbidities would also help with treatment of migraine though only initial studies are first showing this at the current time (22). Further research must assess the discordance between the knowledge and the implementation of a screening tool into clinical practice. Possibilities to be explored include inadequate time, uncertainty about appropriate screening tools, and uncertainty about what to do if patients screen positive.
PCPs were also less familiar with red flags or reasons that might warrant imaging. Although overuse of imaging studies for headache is considered a serious problem (23), our results suggest that underuse may also be a problem. In fact, our results support the recent findings of a cross-sectional study examining neuroimaging utilization tendencies (24). In this study, red flags for intracranial pathology were not associated with an increased use of neuroimaging. In our study, fewer than half of the physicians (47%) said that they would obtain an MRI scan of the brain for a new type of headache. One-quarter (25.3%) said that they would not order an MRI scan of the brain for a migraineur with neurologic symptoms. In addition, only about one-third of PCPs said that they would order an MRI scan of the brain for headache not responding to treatment or worsening of the headache. These four conditions are situations in which some headache experts might say that imaging is necessary for headache patients in a headache subspecialty setting. While not all primary care patients with a new headache or headache not responding to treatment may need head imaging, these results suggest that further exploration of PCP recommendations for neuroimaging may be necessary. Also, despite the concern about physicians ordering too much imaging, our findings indicate that the physicians might not actually be ordering imaging studies in situations where imaging may actually be warranted.
Prior research has shown that close to 40% of migraineurs need preventive therapy but only 13% of them actually receive it (25). In order to close this gap, we felt that it was necessary to determine PCPs’ awareness of the guidelines for preventive therapy. Unfortunately, few PCPs (27.8%) knew about the AAN guidelines for prescribing preventive medications. This is a key element in migraine management because migraine-preventive medications decrease the number and severity of headache attacks and reduce disability (26). Also, many were unaware of the ABIMF’s Choosing Wisely recommendations to limit opioid use and imaging in migraineurs except in particular cases. A significant amount of effort is made to develop these guidelines. Thus, public health efforts must be targeted at educating physicians and patients about such guidelines, which are intended to improve the care of migraine patients. Research in conditions other than headache has not consistently demonstrated improvement in clinical improvement as a result of increased adherence to treatment guidelines (27). Similarly, the extent to which adherence to guideline-recommended treatment would improve most outcomes in patients with headaches is unknown. There is, however, some evidence to suggest that adherence to treatment protocols for management of medication-overuse headache does result in patient improvement (28).
One-third of PCPs did not know that the AAN evidence-based guidelines of non-pharmacologic treatment included CBT, biofeedback and relaxation training. This is concerning because Holroyd et al. showed that a combination of pharmacologic and non-pharmacologic treatment is most effective for treating migraine (29). Despite the remaining two-thirds recognizing that CBT and biofeedback are evidence based, they are not referring patients for these treatments. This may be because there are systemic barriers to obtaining these evidence-based treatments (30).
PCPs are likely to use resources such as UpToDate® (19) (84%) or speak with other senior physicians (68%) to learn more about a medical topic such as migraine. This is consistent with prior research demonstrating that physicians feel overloaded and desire a quick and easy way to obtain quality information in order to make evidence-based decisions regarding patient care (31).
PCPs favored opportunities for direct contact with headache physicians to ask them patient-specific questions. They also valued lunchtime meetings and embedding neurologists into the primary care office to improve migraine diagnosis and treatment. These results suggest that future work should be targeted at improving direct contact with headache physicians, creating more opportunities for headache specialists to visit PCPs for targeted educational sessions, and developing structures where neurologists are physically working alongside PCPs. We had suggested novel models for using online and telephone resources to improve migraine education and to improve the opportunity for contacting headache specialists. However, perhaps these methods were thought to be too time consuming for the PCPs.
Strengths of the study
This was a detailed comprehensive survey developed by experts in neurology and internal medicine. The survey was designed based on the brief questionnaire given to PCPs in the semi-structured group interviews. We were able to assess the knowledge and needs of primary care physicians working in a community-based hospital as well as a large academic hospital. We had a great diversity of physicians—from resident physicians to those with more than 30 years of practice. We also had a response rate of 69%, which is high for a survey of physicians (32).
Limitations of the study
This study was confined to one general geographic location (Boston, MA) and results may not be generalizable to other settings. However, because the PCPs interviewed had trained throughout the US, we believe that their responses are reasonably representative of US practice in general. In identifying themes from the semi-structured group interviews, we were forced to rely on the subjective impressions of the moderators. While the leaders of the semi-structured group interviews were able to discuss most or all of the structured outline of topics, the 15 minutes allotted for the sessions may have limited some of the findings. Most of the questions in the comprehensive survey were multiple choice response, although there were opportunities for participants to leave comments. We tried to overcome the limits of quantitative analysis by conducting the semi-structured group interviews beforehand to get a better sense of information that could be missing from using the quantitative approach.
Asking questions to physicians may lead to problems of social desirability bias. Respondents may have difficulty admitting that they have no knowledge in a particular area. Thus, the physicians who chose “somewhat comfortable” may have a large variation in knowledge level, which may have influenced the results. Our study population consisted of physicians at a tertiary care academic medical center. Thus, there is likely responder bias to more evidence-based practicing physicians. We would predict, therefore, that PCPs overall would be even less educated and comfortable in diagnosing and treating migraine.
Areas of future study
There are various educational methods for intervention that might improve migraine diagnosis and management in the primary care setting. Educational methods of intervention that could be studied in the future include: 1. Headache consultants for each primary care practice whom PCPs can call for help. 2. Neurologists embedded in the primary care practice. 3. Headache specialist office hour visits for primary care physicians. 4. Improvement in the content of Up-to-date® (19). In addition, continuing medical education (CME) groups consisting of group meetings, clinical training courses and peer-academic detailing or educational outreach visits might be future models for educating PCPs about migraine diagnosis and treatment.
Conclusion
Our study highlights that PCPs have a sense of the prevalence of migraine and its related psychiatric comorbidities but that they could use help in the details of the workup and management. Future work should target interventions to improve PCPs’ practice and ultimately improve the care of migraine patients.
Clinical implications
The majority of primary care providers (PCPs) are unfamiliar with the existing migraine treatment guidelines. Many PCPs do not know the indications for when brain imaging is necessary. Most PCPs are unaware of the medications which often cause medication overuse headache. PCPs report that they generally do not refer migraine patients for non-pharmacologic treatment. PCPs favor opportunities for direct contact with neurologists whom they can ask clinical questions regarding migraine management
Footnotes
Acknowledgments
The authors would like to thank the following people for their contributions to making this study possible: Dr Elizabeth Seng for her help in developing the semi-structured group interviews, Dr Huma Sheikh for conducting a semi-structured group interview with PCPs, Emma Weizenbaum for help with managing data and using SPSS, and Dr Shelley Hurwitz and the Harvard Catalyst for help with the survey design.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.