
Abstract
Background:
Migraine is underdiagnosed especially by general practitioners and non-neurologists. In our experience, validated screening and diagnosing tools for migraine are generally not used outside neurology. The three-item identification of migraine (ID-Migraine™) is a short and validated screening/diagnosing tool; positive predictive value for migraine is 93% if at least two out of nausea, photophobia, or disability are present.
Aim:
To investigate the diagnostic yield of ID-Migraine™ when applied to the information provided in the referral letters.
Methods:
Retrospective analysis of 95 referral letters of patients referred for undetermined headache who were finally diagnosed with migraine at our Tertiary Care Headache Center.
Results:
Median age was 34 years, and 75% were women. Migraine was suspected by the referring physician in 33% of patients, whereas the remainder were classified as unclear. ID-Migraine™ criteria were fulfilled in 59% of patients with referral diagnosis of suspected migraine and 23% of patients with unclear headache, respectively. Clinical characteristics associated with migraine suspicion were photophobia and other visual symptoms.
Conclusion:
Applying ID-Migraine™ in primary care, emergency departments, or in specialists’ consultations outside neurology might lead to an increased frequency of migraine recognition. Knowledge about and access to those criteria should be increased, especially in the primary care setting.
Introduction
At our University Hospital Headache Clinic, we regularly observe that patients are referred for further evaluation of “undetermined headache,” even though the diagnosis of migraine without aura could have been made solely from the information provided in the referral letter. The reference standard for migraine diagnosis, the diagnostic criteria by the International Headache Society (IHS), 1 are basically never used by our referring physicians. One might speculate that those criteria might not be feasible in clinical practice for many due to lack of time during consultations. Another reason might be that most non-neurologists might not know about their existence. However, other screening/diagnosing tools are only very rarely used either, even though different brief, easy-to-use, and validated tools to screen for migraine in the primary care setting exist, among them the three-item identification of migraine (ID-Migraine™). 2,3 Positive predictive value for migraine is 93% if at least two out of the following three symptoms are present: nausea, photophobia, or disability. 2 ID-Migraine™ was recommended to be used in different settings including the primary care setting. 4
Against this background, we aimed at evaluating the potential diagnostic yield of ID-Migraine™ by analyzing the information provided in the referral letters.
Methods
This retrospective study analyzes referral letters. Inclusion criteria were patients older than 16 years, first-time referral to the Headache Clinic of the University Hospital Bern, referral between May 2014 and October 2017 for evaluation of undetermined headache, and final diagnosis of migraine without aura according to ICHD 3-beta criteria. 5 Since in our experience, migraine without aura is more often misdiagnosed or not recognized than migraine with aura, we have focused on this in our opinion more neglected and obviously more-difficult-to-diagnose disorder.
All patients who presented to the Headache Clinic were asked to sign a written informed consent (i.e. general consent) that allows the use of their health-related clinical data for national and international research projects on investigation, prevention, diagnosis, and treatment of diseases. Only patients who accepted the general consent were included in this study. Exclusion criteria were other final diagnosis than episodic migraine without aura, established diagnosis of migraine prior to referral, lack of general consent, or unavailable referral letter (i.e. not found in spite of extensive search in electronic patient records).
Study data were collected and managed using the REDCap electronic data capture tool hosted at the University Hospital Bern. 6 The following data were collected from the referral letters: gender; age; referring institution (general practitioner (GP), specialist, university hospital, peripheral hospital); specialty of referring physician; referral diagnosis; disability (impairment in social, professional, or familiar functioning); presence of phonophobia, photophobia, nausea, vomiting, dizziness, paresthesia, visual symptoms other than photophobia; aggravation by physical activity; and pain characteristics (intensity, quality, duration, localization, laterality). Furthermore, we evaluated whether IHS criteria for migraine without aura or migraine-specific screening tools were used by the referring doctor.
Ethics review board approval
The study was approved by Swissethics, the Swiss Ethics Committees on research involving humans.
Statistical analysis
Associations between referral diagnosis (suspected migraine or unknown) and clinical variables were assessed using the Wilcoxon rank-sum test for continuous variables, and using the χ 2 or the Fisher’s exact test, as appropriate, for categorical variables. All tests were two-sided with a significance level of 0.05. Statistical analysis was performed using R, version 3.3.1 (R Core Team 2018, Vienna, Austria). Results are expressed as numbers and percentages for categorical variables, and as a median [25th percentile; 75th percentile] for continuous variables, according to their distribution.
Results
During the 42 months’ period, 95 referral letters fulfilled the inclusion criteria (Figure 1).
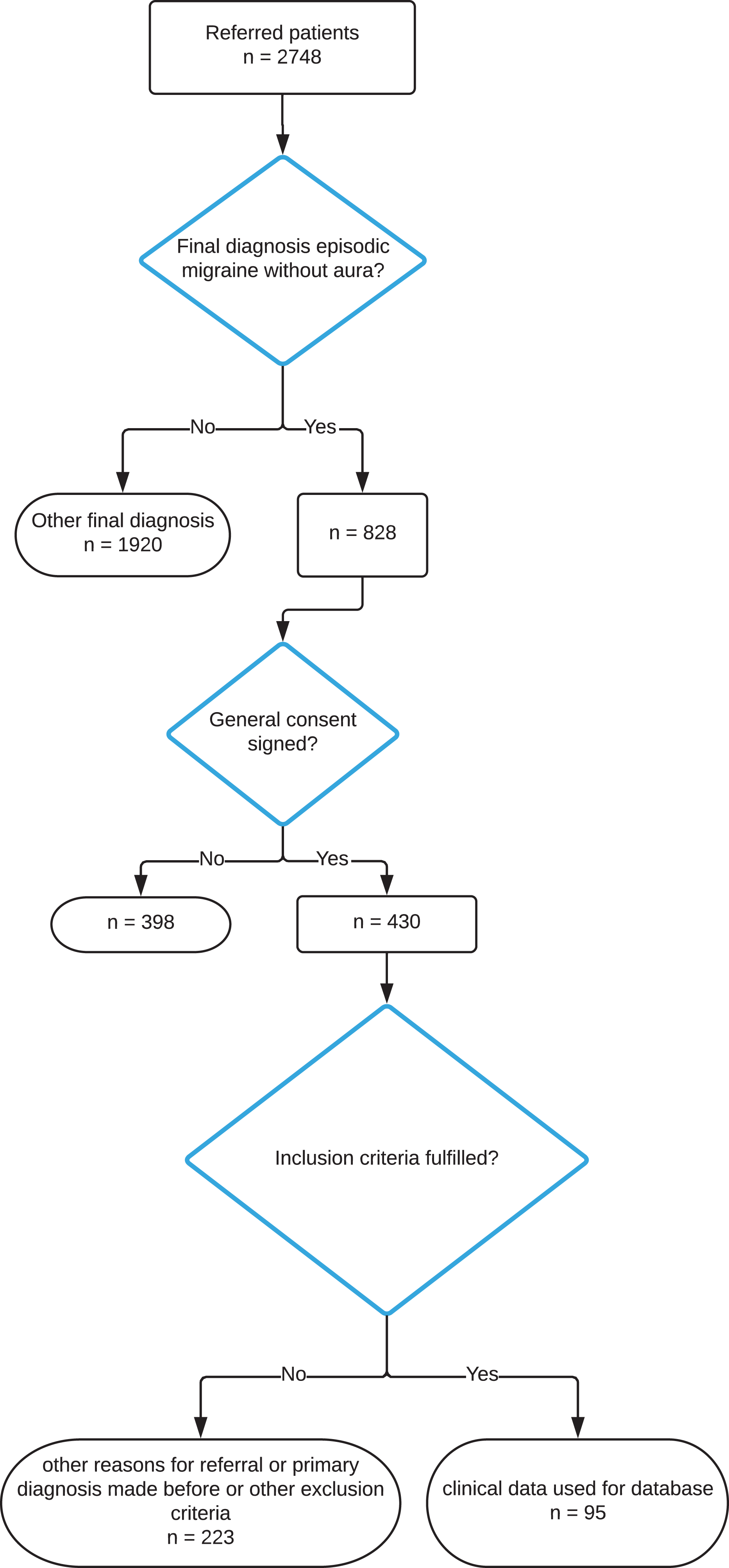
Flow chart illustrating inclusion procedure.
In 32 patients (33.7%), migraine was suspected by the referring physician, whereas in the other patients, the headache disorder was classified as unknown (Table 1). Median age was 34 years, and 71 (74.7%) were women. Most patients had been referred by the University Hospital (n = 48, 50.5%) or GPs (n = 42, 44.2%). Most referrals from the University Hospital came from the interdisciplinary emergency, gynecology, and internal medicine departments. No referring physician indicated the use of any migraine screening or diagnosing tools.
Characteristics of the study population.a
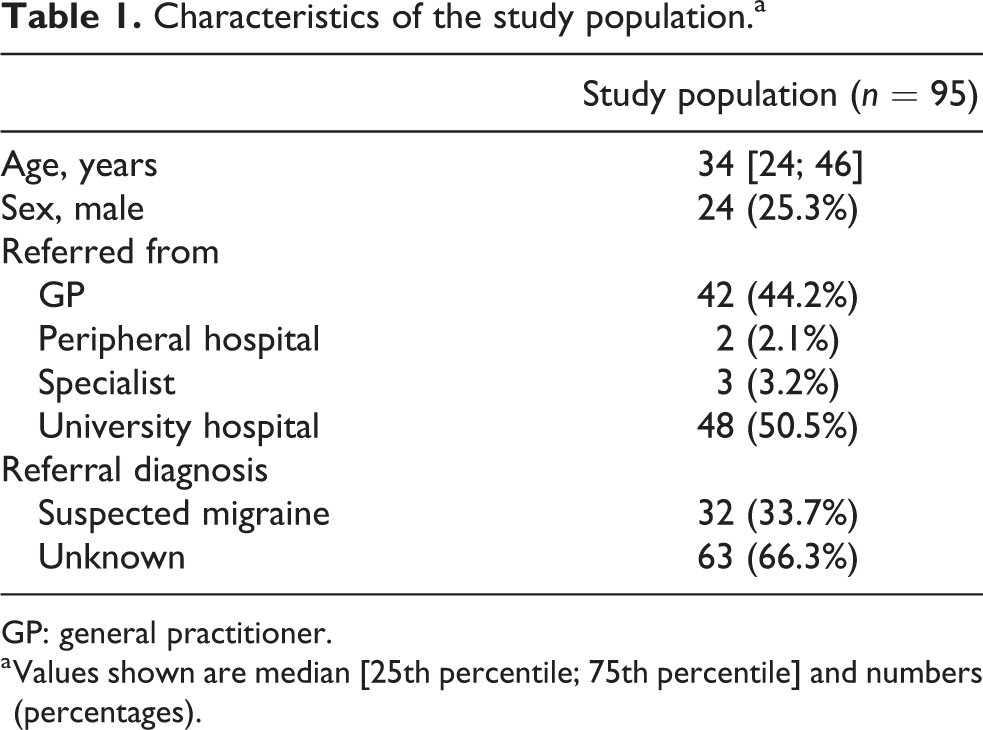
GP: general practitioner.
a Values shown are median [25th percentile; 75th percentile] and numbers (percentages).
Table 2 shows patient characteristics according to referral diagnosis. Headache interference with working, family, or social functions was high in both groups, ranging from 90% to 100%. Photophobia and visual disorders other than photophobia were significantly more frequent in the suspected migraine group. The prevalence of dizziness, nausea, and pulsating pain in that group tended to be higher. Pain intensity, duration, and laterality did not differ significantly between groups.
Characteristics of the study population according to referral diagnosis.a

MD: missing data; NRS: numerical rating scale (1–10/10); ICHD 3-beta: International Classification of Headache Disorders, 3rd edition, beta version; ID-MigraineTM three-item identification of migraine.
a Values shown are median [25th percentile; 75th percentile] and numbers (percentages).
P-values < 0.05 are bold-faced.
ICHD 3-beta criteria for migraine were fulfilled in three referral letters (9.4%) in the suspected migraine group and in two (3.2%) in the group of unknown headache disorder (p = 0.33). ID-Migraine™ criteria were fulfilled in 19 (59.4%) referral letters in the suspected migraine group and in 15 (23.8%) in the unclear headache disorder group (p < 0.001).
Discussion
Although migraine is a very frequent disorder with an enormous burden of disease, 7 it is underdiagnosed by GPs (and other physicians). 8 The reasons for this might be manifold. The results of the present analysis of referral letters of patients referred for the evaluation of “undetermined headache” who were finally diagnosed with migraine without aura according to the IHS criteria 5 indicate that one important reason seems to be a lack of knowledge about key migraine features. This translates into an important percentage of fulfilled ID-Migraine™ criteria when analyzing only the information provided in referral letters, which generally are not very detailed. Referring physicians are not required to provide particular information in referring letters to refer a patient to our headache clinic except for personal data, which leads to great differences as far as information about patient’s conditions is concerned, and which led to the high amount of missing data in our study. Yet referring physicians seem to ask after key anamnestic features such as disability, photophobia, and nausea (i.e. the ID-Migraine™ criteria), but seem to fail to fully recognize their meaning in patients with presumably undetermined/unclear headache: While visual symptoms were associated with suspicion of migraine in the present study, disability and nausea were not. On the other hand, neurologists and neurological societies obviously seem to fail to sufficiently spread the knowledge on practical, short, and validated migraine screening/diagnosing tools such as ID-Migraine™.
In our opinion, the present study setting represents the real-world situation of specialized headache centers, thus our results are likely to be generalizable. One important limitation is the high amount of missing data, also reflecting a real-world situation where amount and accuracy of information provided varies widely.
Conclusion
Applying ID-Migraine™ in primary care, in specialists’ consultations outside neurology, or in other settings where there is no neurologist and a lack of time might lead to an increased frequency of migraine recognition. Knowledge about and access to those criteria should be increased, for example, by awareness campaigns of national headache societies or via patient organizations. Evaluation of key migraine features such as photophobia/visual symptoms, nausea, or disability associated with headache attacks could even be done before consultation, even by a nurse practitioner, probably increasing efficacy during consultation. Also, standardized referral forms to refer patients to the headache clinic could be created, where ID-Migraine™ criteria could be mentioned to help referring doctors with focusing on relevant clinical symptoms and at the same time increasing migraine symptoms awareness.
Clinical implications
Migraine remains an underdiagnosed disorder especially outside neurology.
ID-Migraine™ is an easy-to-use and validated screening tool, and its use should be promoted especially outside neurology consultations.
Footnotes
Acknowledgement
The authors thank Delphine Meier-Girard for statistical analysis.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.