
Abstract
Background
: The trigemino-cerebrovascular system is recognized as a key anatomical structure playing a crucial role in the pathophysiology of migraine. It is also well established that the herpes simplex virus (HSV) resides within the trigeminal ganglion. Previous studies have emphasized the role of infectious inflammatory conditions in migraine. We hypothesize the potential involvement of HSV infection in migraine pathology.
Method
This study employed a case–control design to investigate the association between plasma HSV type 1 and 2 IgM and IgG antibodies and migraine. A total of 111 subjects were selected from patients referred to the Neurology Clinic at Tehran's Shariati Hospital, including 57 migraine cases and 54 healthy controls. Participants completed questionnaires covering demographic data and migraine severity. Blood samples were collected from all participants, and HSV-1 and HSV-2 IgM and IgG antibody levels were assessed using the VIRCELL Herpes Simplex Virus I and II ELISA IgG/IgM kit.
Results
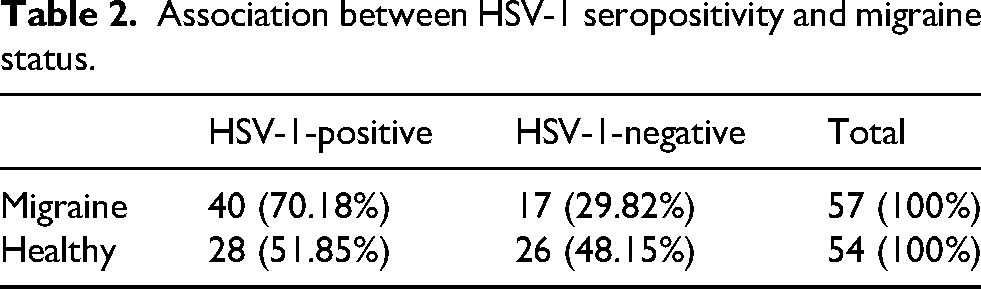
The prevalence of HSV-1 seropositivity was 70.18% (40 of 57) in participants with migraine, which was significantly higher compared to 51.85% (28 of 54) in the control group (p = 0.48). HSV-1 seropositivity was associated with a 2.185-fold increase in the odds of having migraine (OR = 2.185, 95% CI: 1.002–4.762). However, the quantitative analysis of HSV-1 IgG levels in relation to migraine severity scores did not show statistical significance.
Conclusion
The observed association strengthens the hypothesis of the potential role of HSV in the pathophysiology of migraine. Our findings suggest that targeting HSV-1 could be a promising strategy for developing new treatments for migraine prophylaxis.
This is a visual representation of the abstract.
Introduction
Migraine, a complex interplay of genetic, biochemical, and anatomical factors, is characterized by altered central neuronal processing, including cortical hyperexcitability and spreading cortical depression. 1 The activation of the trigemino-cerebrovascular system serves as a key relay point for pain signals through the release of calcitonin gene-related peptide (CGRP), leading to vasodilation, inflammation, and ultimately migraine pain. 2 Multiple studies have shown that various infectious inflammatory conditions are linked to an increased risk of developing migraine.3,4
Herpes simplex virus type 1 (HSV-1), a widespread pathogen infecting approximately 65% of the general population, establishes latency in the trigeminal ganglion. 5 Herpes simplex virus type 2 (HSV-2) is also known to reside inside the trigeminal ganglion. 6 Therefore, there is a growing suspicion that there might be a link between chronic HSV infection and migraine.
Additionally, HSV-1 and HSV-2 can lead to a range of neurological complications. 7 These complications may include conditions such as herpes simplex encephalitis, which is characterized by severe inflammation of the brain and can result in neurocognitive deficits, seizures, and even death. 8 Moreover, Freilinger et al. reported two cases with a history of migraine in whom HSV-2 meningitis triggered particularly severe attacks of migraine. 9 Napier et al. also reported a case of migraine treated with famciclovir. 10 Both of these case reports have supported the hypothesis that there is a probable association between HSV infection and migraine.
Considering the suspected role of HSV in migraine pathophysiology, we hypothesize that HSV infection could be a contributing factor to migraine development. Hence, we aim to verify the association between HSV-1 and HSV-2 serology and migraine and investigate whether the severity of migraine is correlated with HSV infection status.
Methods
The current study employed a retrospective case–control design to investigate the association between migraine and HSV-1 and HSV-2 serology. This observational study was designed and reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.
Study participants
All participants were selected from patients referred to the Neurology Clinic at Tehran's Shariati Hospital between 2022 and 2024. A total of 111 subjects, all aged between 18 and 65 years old, were recruited, comprising 57 individuals with migraine (cases) and 54 healthy individuals (controls) who were matched for age and sex during the participant recruitment phase. The exclusion criteria included any participants with immunological deficiencies, sinus thrombosis, brain tumors, or a history of brain-related medical issues and surgeries. Demographic data, including gender, age, drug history, and past medical history, were collected to provide a comprehensive understanding of our subjects. Written informed consent was obtained from all participants after a detailed explanation of the study, including the collection of blood samples, was provided. This study conformed to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Tehran University of Medical Sciences (IR.TUMS.SHARIATI.REC.1402.099).
Measurements
Interview-based questionnaires were designed to collect demographic data such as age, gender, past medical history, and drug history. The Headache Impact Test-6 (HIT-6) and headache severity scores were calculated via interviews conducted by a fourth-year neurology resident. The diagnosis of migraine headache was confirmed according to the International Classification of Headache Disorders, 3rd edition (ICHD-3), published in 2018. 11 Additionally, patients in the migraine group were assessed for migraine characteristics using the Migraine Disability Assessment (MIDAS). The severity of headache was assessed using a Visual Analog Scale (VAS), a widely validated and reproducible tool for quantifying subjective pain intensity. Patients were asked to rate their current headache pain on a 10-point scale, where 0 represented no pain and 10 represented the worst pain imaginable. Subjects were also asked for any history of herpes sores.
Blood samples were collected from all participants using standard venipuncture techniques. Each participant's blood was drawn into sterile tubes. The samples were immediately transported to the laboratory under controlled conditions to ensure sample integrity. Upon arrival at the laboratory, the blood samples were centrifuged at 3000 rpm for 10 min to separate the plasma from cellular components. The plasma was carefully extracted and stored at −8°C until further analysis. HSV-1 and HSV-2 antibody levels (IgG and IgM) were assessed using the VIRCELL Herpes Simplex Virus 1 and 2 ELISA IgG/IgM kit (IgG-1 recombinant). The procedure was carried out according to the manufacturer's instructions. In the end, the raw titers were adjusted by dividing the raw titer by the mean titer of healthy samples, considering any titer above 1.1 positive, less than 0.9 negative, and any titer between ambiguous. Ambiguous data underwent triple verification to ensure accuracy. To further extend our test results and determine the eligibility of quantitative testing, a dilution test series was conducted on HSV-1 and HSV-2 qualitative ELISA. The objective was to ensure the kits could report HSV-specific antibodies in a linear pattern for quantitative analysis. The process involved creating serial dilutions of anti-HSV-1 and anti-HSV-2 IgG provided in the kits and then comparing the optical density results to these standards. The substrate was carefully extracted from the ELISA kit with a micropipette and deposited in the microplate wells. Then, the substrate was diluted on a logarithmic scale to a factor of 4 (log 4). The optical density was then measured using a spectrophotometer. According to the results from the spectrophotometer, a linear pattern emerges for HSV-1 IgG at concentrations exceeding 0.35 and for HSV-2 IgG at concentrations above 0.08, making both suitable for quantitative evaluation. Laboratory personnel were blinded to the case/control status of the samples throughout the analysis; samples were coded, and their status was not revealed until after all analyses were completed.
Statistical analysis
Data analysis was performed using IBM SPSS software version 27.0. Descriptive statistics were used to summarize the demographic and clinical characteristics of the participants. The association between HSV-1 and HSV-2 seropositivity and migraine was evaluated using chi-square tests for categorical variables and independent t-tests for continuous variables. Also, logistic regression analysis was employed to adjust a variable between two groups. Correlation analyses were conducted to investigate the association between quantitative variables. A p-value of less than 0.05 was considered statistically significant. A brief summary of the study methodology is illustrated in Figure 1.

Study methodology overview.
Results
Demographics and basic characteristics
For the study, 111 participants were recruited, comprising 57 migraine cases and 54 healthy controls. Table 1 presents the baseline demographic characteristics of both groups. The migraine and control groups had mean ages of 35.2 ± 7.0 years and 32.2 ± 9.1 years, respectively. The gender distribution was also similar between the two groups, with 29.8% (17 of 57) males in the migraine group and 31.5% (17 of 54) males in the control group (p > 0.05).
Baseline demographic characteristics.

Values in parentheses show the lower and upper range of the parameter. *P-value <0.05 migraine vs. healthy subjects.
Furthermore, the severity of headaches was compared between the two groups. The migraine group had significantly higher severity scores, with a mean of 4.3 ± 2.3, compared to the control group, with a mean of 1.1 ± 1.3. It is essential to note that none of the participants exhibited active signs or symptoms of a herpes infection. However, 32 (28.8%) subjects in the study population reported a history of sores in the mouth or genital areas, with 18 (31.6%) of them having migraine.
HSV results
Table 2 illustrates the association between HSV-1 IgG seropositivity and migraine status. The chi-square test revealed a statistically significant relationship between migraine and HSV-1 seropositivity (χ2(1) = 3.9, p = 0.048). The Phi coefficient, which measures the strength of this association, was calculated to be 0.2. However, HSV-1 IgM was negative across all the populations in this study. The odds of having migraine were 2.185 times greater among individuals who were seropositive for HSV-1 compared to those who were seronegative (OR = 2.185, 95% CI: 1.002–4.762).
Association between HSV-1 seropositivity and migraine status.
Additionally, within the migraine subjects, comparisons of age, gender, MIDAS, HIT, and severity scores were performed between HSV-1-positive and -negative groups. All comparisons were found to be statistically insignificant, except for age. The age of participants in the HSV-1 group was significantly higher compared to those in the HSV-1 negative group (Table 3). Also, a history of sores was significantly more prevalent among HSV-1-positive patients. However, a positive sore in past history was not significantly associated with positive migraine status (p = 0.551).
Comparison of demographic characteristics between HSV-1-positive and -negative groups in migraine subjects.

In the subgroup of participants who were both migraine sufferers and HSV-1 seropositive, the association between quantitative HSV-1 values and various migraine-related measures (MIDAS, HIT, severity) was investigated. The Pearson coefficient between HSV-1 IgG and MIDAS, HIT, and severity was calculated as −0.221 (p = 0.172), −0.041 (p = 0.801), and −0.153 (p = 0.346), respectively. The analysis revealed very weak associations across all measures; however, these associations were statistically insignificant.
Quantitative analysis revealed a higher yet insignificant HSV-1 IgG titer in migraine subjects (2.09 ± 0.59 in healthy subjects vs. 2.52 ± 0.67 in migraine subjects; p = 0.133).
From the entire population, only two samples tested positive for HSV-2 IgG: one from the healthy group and the other from the migraine group. Similar to HSV-1, HSV-2 IgM was also entirely negative among the studied population.
Discussion
Considering that both migraine and HSV infections are prevalent conditions and recognizing that both primarily affect the trigeminal ganglion, we hypothesized a potential association between these two entities. Building on our hypothesis that HSV-1 and HSV-2 may play a role in the pathophysiology of migraine, we conducted a comprehensive case-control study to explore this association. Our findings indicate that migraine subjects were significantly more seropositive for HSV-1 compared to controls. However, despite these associations, we did not find a significant relationship between HSV antibody levels and migraine severity scores, such as MIDAS, HIT, and overall severity.
Recent advances in understanding the pathophysiology of migraine have highlighted several novel mechanisms, particularly involving the trigeminal ganglion. The trigeminal ganglion plays a crucial role in migraine by housing neurons that release CGRP, which triggers vasodilation and inflammation, contributing to migraine pain. 12 Cortical spreading depression (CSD), a wave of neuronal and glial depolarization, sensitizes the trigemino-vascular system, exacerbating pain transmission. Additionally, serotonin depletion has been shown to worsen CSD-evoked pain, further implicating the trigeminal ganglion in migraine pathophysiology. 13
Emerging research also points to the involvement of mechanosensitive receptors and mitochondrial dysfunction in the trigeminal neurons, which amplify nociceptive signals. 14 In 2013, LaPaglia et al. conducted RNA-Seq analyses on postmortem human trigeminal ganglia to understand molecular factors contributing to migraine and headaches. They revealed significant expression of migraine susceptibility genes in neurally enriched regions and an association between HSV-1 transcripts in the ganglia and blood antibody levels. 15 A 2018 case report documented the successful treatment of severe migraine headaches with famciclovir and celecoxib, both of which have antiviral activity against HSV. The study concluded that this combination was effective both as an abortive and prophylactic therapy, suggesting a synergistic effect in treating migraine disorder. Napier et al. hypothesized that migraine might be linked to the reactivation of latent HSV in the trigeminal ganglion. 10
In recent decades, there has been growing attention to the potential role of herpesviruses in neurodegenerative diseases.8,16,17 Previous studies have linked HSV-1 and HSV-2 infection to Alzheimer's disease, identifying neurodegenerative markers in human neuroblastoma cells.18,19 Regardless of whether an individual is symptomatic or asymptomatic after HSV infection, the virus's lifelong presence can alter cellular processes essential for normal neuronal function, 20 potentially leading to brain pathology in some seropositive individuals. The proposed factors linking HSV to neurodegenerative diseases include its modulation of apoptosis-related pathways, disruption of autophagy processes, induction of mitochondrial dysfunction, and oxidative stress. Specifically, HSV-1 alters DNA damage response and produces immune cell-mediated neuroinflammation. 5
Most recently, a study by Zheng et al. conducted on the NHANES database investigated the association between HSV-1 and HSV-2 and severe headaches. 21 Compared to our study, several key differences and similarities emerge. Most importantly, Zheng et al. found a significant link between HSV-2 seropositivity and severe headache or migraine, strengthening our hypothesis (OR = 1.22, 95% CI: 1.03–1.46, p = 0.0443). However, the population epidemiology of HSV in Iran differs from that in the USA. In Iran, HSV-2 seroprevalence (6.5%) tends to be notably lower than in the USA (11.9%). 22 Both case and control groups in this study had similar demographics, which ensured a more homogeneous comparison and reduced confounding factors. We also conducted a more comprehensive evaluation of patients, utilizing tools such as the MIDAS and HIT scores to assess migraine severity more thoroughly. Furthermore, our study focused exclusively on migraine, providing a more targeted analysis, whereas the referenced article included both migraine and severe headaches, encompassing a broader spectrum of headaches.
The population examined in this study demonstrated a complete absence of HSV-1 and HSV-2 IgM and presented no signs or symptoms indicative of herpes. These findings collectively imply that the population does not exhibit either an active infection or viral reactivation, suggesting that HSV may have established a chronic presence within their nervous systems. Considering previous literature,5,6 latent herpes virus resides in the trigeminal ganglion.
Alongside the notable association observed between HSV-1 IgG levels and migraine status based on our results, we may suggest that the chronicity of HSV may contribute to the onset of migraine attacks in affected individuals. Nevertheless, to corroborate this assertion, a comprehensive cohort study including subjects with active HSV infection might be helpful.
Another result warranting discussion is the significant association between a history of herpetic sores and HSV-1 IgG seropositivity, which aligns with the understanding that clinical manifestations serve as indicators of viral exposure and the subsequent immune response. However, the absence of a significant association between a history of sores and migraine status, while contrasted with the significant association between HSV-1 IgG seropositivity and migraine, raises intriguing questions regarding the underlying mechanisms. One plausible explanation is that HSV-1's latent infection in the trigeminal ganglion may influence migraine development independently of clinical symptoms. 23 Latent HSV-1 has the potential to induce subtle inflammatory responses or alter neuronal excitability without producing overt sores. These subclinical effects could contribute to the sensitization of trigeminovascular pathways involved in migraine attacks. 20 The discrepancy between clinical history and serological evidence suggests that reliance solely on patient-reported symptoms may lead to an underestimation of the impact of HSV-1 on migraine pathology. Serological testing offers a more comprehensive assessment of viral exposure and its potential neurological effects. Furthermore, studies have indicated the presence of HSV-1 RNA in the trigeminal ganglia of individuals devoid of a history of herpetic lesions, 15 thereby supporting the notion that asymptomatic latency may influence neurological conditions. This latent presence could play a role in the activation of glial cells and the promotion of neuroinflammation, both of which are key factors in migraine pathogenesis. Moreover, despite the significant qualitative association, the quantitative results showed higher mean concentrations of both HSV-1 and HSV-2 in the migraine group without reaching statistical significance. This discrepancy might be explained by the variability in viral load and the episodic nature of both HSV reactivation and migraine attacks. It is also possible that while the presence of HSV-1 qualitatively influences migraine, the viral load itself does not have a direct linear relationship with migraine severity or frequency. This highlights the importance of considering both qualitative and quantitative aspects in viral studies related to neurological conditions.
Another important observation is that the age of the HSV-1-positive group was significantly higher than that of the negative group, aligning with epidemiological data showing increased HSV-1 prevalence with age. This may be due to cumulative virus exposure, as HSV-1 is often acquired in childhood and remains for life. Older individuals might also be more likely to experience reactivation of latent HSV-1, contributing to the association with migraine. These findings emphasize the need to consider age as a confounding factor in studies of HSV infection and migraine. 24
The current study has some strong points. To the best of our knowledge, this is the first case–control study to investigate the association of HSV serology with migraine. Another key feature of our research is the inclusion of the clinical signs of HSV infection. We gathered data on previous HSV sores and assessed their association with migraine status.
Regarding our limitations, the relatively small sample size and convenience sampling limit the generalizability of our findings. As mentioned before, the seroprevalence of HSV differs in various countries and ethnicities; thus, a multi-ethnic study is necessary to confirm whether HSV-1 and HSV-2 play the leading role in triggering migraine. The sample size was measured based on HSV-1; however, a larger sample size is required for the evaluation of HSV-2. A study involving several patients with symptomatic HSV can also shed light on certain gray areas we discussed earlier. Also, as a case-control study, it cannot establish causation between HSV infection and migraine, which may require longitudinal studies for further validation.
Conclusion
In this small, single-center exploratory study, we observed a possible association between HSV-1 seropositivity and migraine. Given the limited sample size and potential selection biases, these findings require confirmation in larger, prospectively designed, multi-center studies before any clinical or therapeutic implications can be inferred.
Clinical implications
The study identified significant associations between HSV-1 seropositivity and migraine, suggesting potential involvement of HSV latency in migraine pathophysiology.
Despite qualitative associations, no significant relationship was found between HSV antibody levels and migraine severity metrics, such as MIDAS or HIT scores.
The study's limitations, including small sample size and regional seroprevalence differences, highlight the need for larger, multi-ethnic cohort studies.
Footnotes
ORCID iDs
Ethical approval
This study conformed to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Tehran University of Medical Sciences.
Consent to participate
Written informed consent was obtained from all participants after a detailed explanation of the study, including the collection of blood samples, was provided.
Consent for publication
Yes.
Author contributions
Azam Ahangar Darabi: project administration (lead), data acquisition, conceptualization (supporting), methodology (supporting). Sadaf Agahi: writing—original draft (lead), data curation (lead), analysis and interpretation of data (lead). Ali Kermanpour: writing—review and editing (equal), data acquisition, analysis, and interpretation of data (supporting). Ahmadreza Niavarani: methodology (lead), design (lead). Nazila Malekian: conceptualization (supporting), supervision (supporting), writing—review and editing (equal). Siamak Abdi: conceptualization (lead); supervision (lead); writing—review and editing (equal), validation (lead).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data supporting this article is available from the authors upon request.