
Abstract
Background and aims
New daily persistent headache (NDPH) is a primary headache disorder characterized by the abrupt onset of continuing and unremitting headache within 24 h of onset. Diagnosis is clinical, requiring exclusion of secondary causes, with limited imaging and treatment data. We assessed the prevalence of nonspecific white matter hyperintensities (WMH) and treatment response in a large retrospective cohort with primary NDPH.
Methods
A retrospective chart review was conducted on 328 patients diagnosed with NDPH by a headache subspecialist over an 8.5-year period. Patients were classified into the migraine phenotype (MP; n = 260) or tension-type phenotype (TTP; n = 50) based on associated features. The presence of WMH reported on MRI scans and acute and preventive treatment responses were evaluated.
Results
WMH were reported in 20.9% of MP patients (33/158) and 18.0% of TTP patients (9/50), p = .658. Acute treatments for the MP and TTP were minimally, if at all, effective. Preventive treatments generally had limited effectiveness. For the MP, the percentages of patients achieving a 30% or greater reduction in headache days per month were the following: desvenlafaxine, 54.5%; venlafaxine, 41.2%; and onabotulinumtoxinA, 27.9%. Venlafaxine was the most effective for the TTP with 25% having a 30% or greater reduction in headache days. Greater occipital and pericranial nerve blocks were mildly effective while surgical procedures were largely ineffective. Up to five day inpatient intravenous regimens with dihydroergotamine produced temporary benefit in 41.7%.
Conclusions
WMH are present in a minority of NDPH patients. Acute treatment is largely not effective. Preventive treatments were more effective in those with MP than TTP with many failures. Future prospective studies with new treatments are needed to identify effective interventions for this often disabling and refractory disorder.
Introduction
Primary new daily persistent headache (NDPH) is a rare disorder defined by the third edition of the International Headache Society (International Classification of Headache Disorders-3) as a continuous and unremitting headache within 24 h of onset present daily and unremitting for more than three months with secondary causes excluded by appropriate testing. 1 To meet the criteria, individuals should have a prior history of infrequent migraine or tension-type headaches to distinguish NPDH from the evolution of a primary headache disorder. 2
Two phenotypic presentations of NDPH have been proposed with treatment based upon the phenotype: a migraine phenotype (MP), with associated symptoms such as nausea and photophobia/phonophobia, and a tension-type phenotype (TTP), lacking such features. 2 Prior studies have found a persistent disorder often not responsive to acute and preventive treatments. Imaging studies, particularly MRI, have reported white matter hyperintensities (WMH) in patients with migraine. However, the significance of such findings in NDPH remains unclear. We hypothesized that there may be a significant difference in the prevalence of WMH in MP as compared to TTP.
This study aimed to assess the prevalence of WMH on brain MRI among patients with MP versus TTP phenotypes of NDPH and real-world effectiveness of acute and preventive treatments stratified by phenotype.
Methods
The coauthor (RE), a neurologist subspecialty certified in headache medicine, used consecutive sampling to perform a retrospective chart review of all patients he had seen in a general neurology outpatient clinic in Houston, Texas from 1 September 2011 through 28 February 2020 (8.5 years) with a provisional diagnosis of NDPH after obtaining an independent review board exemption. 3 Diagnosis was based upon ICHD-3 criteria. A standardized headache intake questionnaire and quality of life measure were not used. A checklist was not used for exacerbating factors. Patients were asked to provide headache intensity using the visual analog scale from 1 to 10 out of 10 and more than one quality of the pain, if present, was recorded. Patients were diagnosed as having the MP if they had associated nausea with or without vomiting and/or light and noise sensitivity and TTP if absent. Evans and Turner provide more information about the methodology. 3
Preventive oral treatments were included if the patient titrated up the dose as tolerable and took the medication for at least six to eight weeks. OnabotulinumtoxinA injections were included if the patient had at least two injections 12 weeks apart using the Phase III REsearch Evaluating Migraine Prophylaxis Therapy injection sites. Anticalcitonin gene-related peptide injectable medications were included if the patient had at least three consecutive months of treatment. Patients were classified as having potential medication overuse headache (MOH) if they met the ICHD-3 MOH criteria. 1
The inpatient intravenous (IV) regimen included dihydroergotamine (DHE) 0.5 mg titrated up to 1 mg as tolerated every 8 h for up to five days which was variably combined with valproate sodium 500 mg IV every 8 h, and ketorolac IV 30 mg bid as needed. DHE pretreatment included metoclopramide 10 mg IV, ondansetron 4 mg IV, or promethazine 25 mg IV every 8 h.
OnabotulinumtoxinA was administered in 31 sites (five units per site) per the Phase 3 Research Evaluating Migraine Prophylaxis Therapy paradigm in the product information.
Greater occipital nerve blocks were performed with 3 cc of 1% lidocaine. Bilateral supraorbital, supratrochlear, auriculotemporal, and greater occipital nerve blocks were performed with 3 cc for the greater occipital nerve and 0.5 cc for the other sites with 1% lidocaine.
To assess for the presence of WMH, magnetic resonance imaging (MRI) scans of the brain were performed as part of routine care to exclude secondary headache on numerous scanners with different field strengths including T1-weighted, T2-weighted, fluid-attenuated inversion recovery sequences, and interpretations by many radiologists with results included from available radiologists’ reports without a re-review and without the use of a standardized imaging protocol. If more than one MRI was done and the reports were available, the last scan was reported.
Statistical analyses
Frequency counts (%) and median [25th, 75th] were used to describe the sample. A chi-squared test was used to examine differences in the proportions between MP and TTP subgroups. Analyses were conducted using R 4.4.1 and RStudio (2024.12.0 + 467) software. The analyses were conducted using all available data during the observation period, and no a priori statistical power calculations were conducted. Where appropriate, p < .05 was used for statistical significance. The statistical analyses were intended to be descriptive, examining apparent differences across presenting characteristics. No attempt was made to adjust comparisons for confounding influences. ChatGPT was used for computation but not statistical analysis.
Results
A total of 328 patients met the ICHD-3 NDPH criteria including 215 (65.5%) female patients with a mean age of onset of 40.3 years (range 12–87 years). The MP was present in 260 subjects and TTP was present in 68. Evans and Turner provide more information about the clinical features. 3
During the observation period, 208/328 patients had available MRI of the brain reports from a radiologist. For the MP, 158/260 patients had available reports and WMH were present on 33 (20.9%). For the TTP, 50/68 patients had available reports and WMH were present on 9 (18.0%). There was no statistically significant difference between MP and TTP prevalence, χ2 (1) = 0.196, p = .658. The median (25th percentile and 75th percentile) latency between the onset of NDPH and the MRI scans in years were as follows: MP, 0.3 [0.2, 0.8]; and TTP, 0.4 [0.2, 1.1].
Tables 1–4 provide acute and preventive treatments for MP and TTP where adequate information was available from treatment provided by prior treaters and Dr Evans.
Acute treatments responses for migraine phenotype.
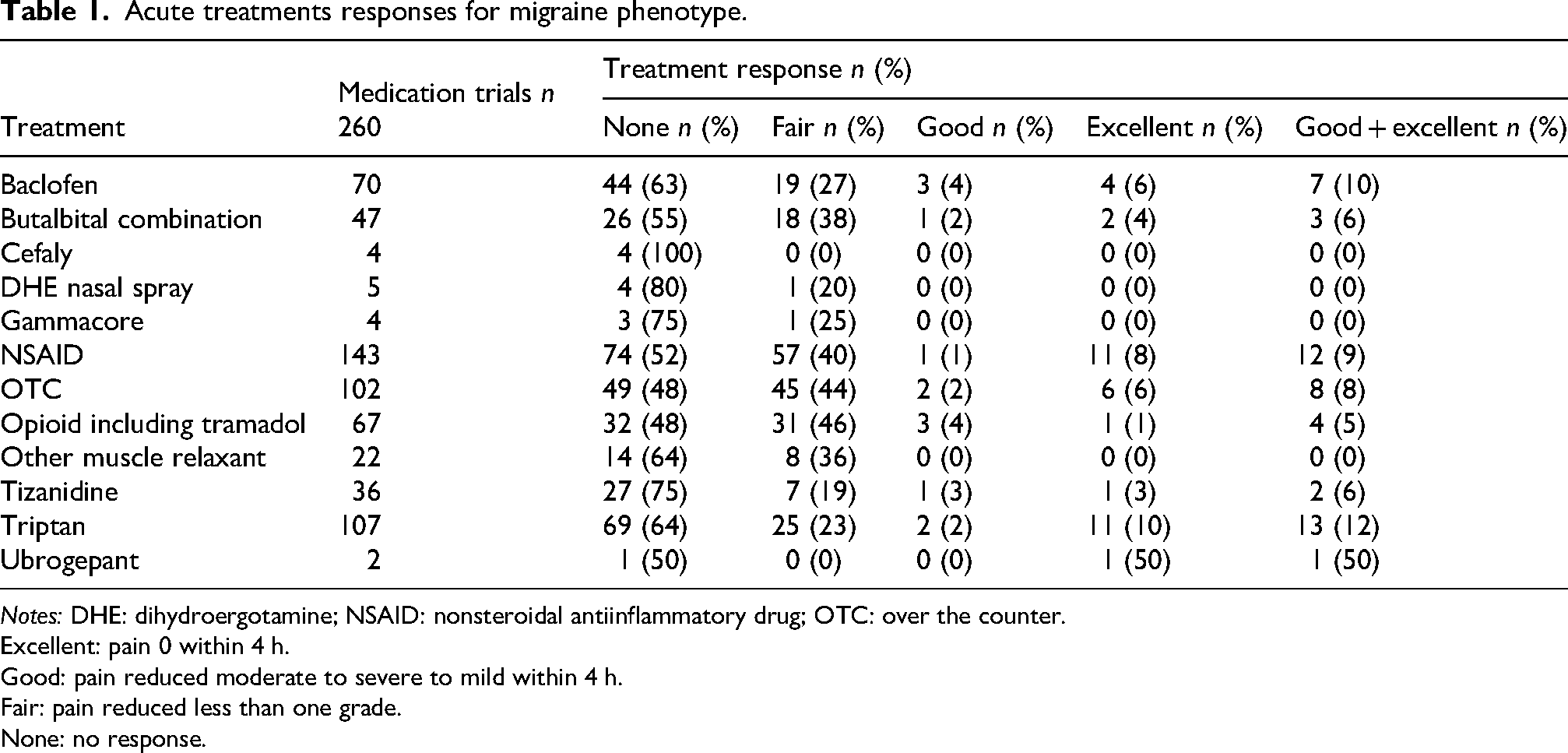
Notes: DHE: dihydroergotamine; NSAID: nonsteroidal antiinflammatory drug; OTC: over the counter.
Excellent: pain 0 within 4 h.
Good: pain reduced moderate to severe to mild within 4 h.
Fair: pain reduced less than one grade.
None: no response.
Acute treatment responses for tension-type headache phenotype.

Notes: NSAID: nonsteroidal antiinflammatory drug; OTC: over the counter.
Excellent: pain 0 within 4 h.
Good: pain reduced moderate to severe to mild within 4 h.
Fair: pain reduced less than one grade.
None: no response.
Efficacy of preventive medications for migraine phenotype.

Notes: PREEMPT: Phase III REsearch Evaluating Migraine Prophylaxis Therapy protocol for injections sites and doses of onabotulinumtoxinA; SSRI: selective serotonin reuptake inhibitor.
No response = N.
Decreased intensity = D.
Daily but not constant = L.
Daily intermittent and less severe = B.
30–49% reduction in headache days per month = F.
≥50–75% reduction in headache days per month = G.
≥75% in reduction in headache days per month = E.
100% reduction for at least one month = C.
Efficacy of preventive medications for tension-type phenotype.
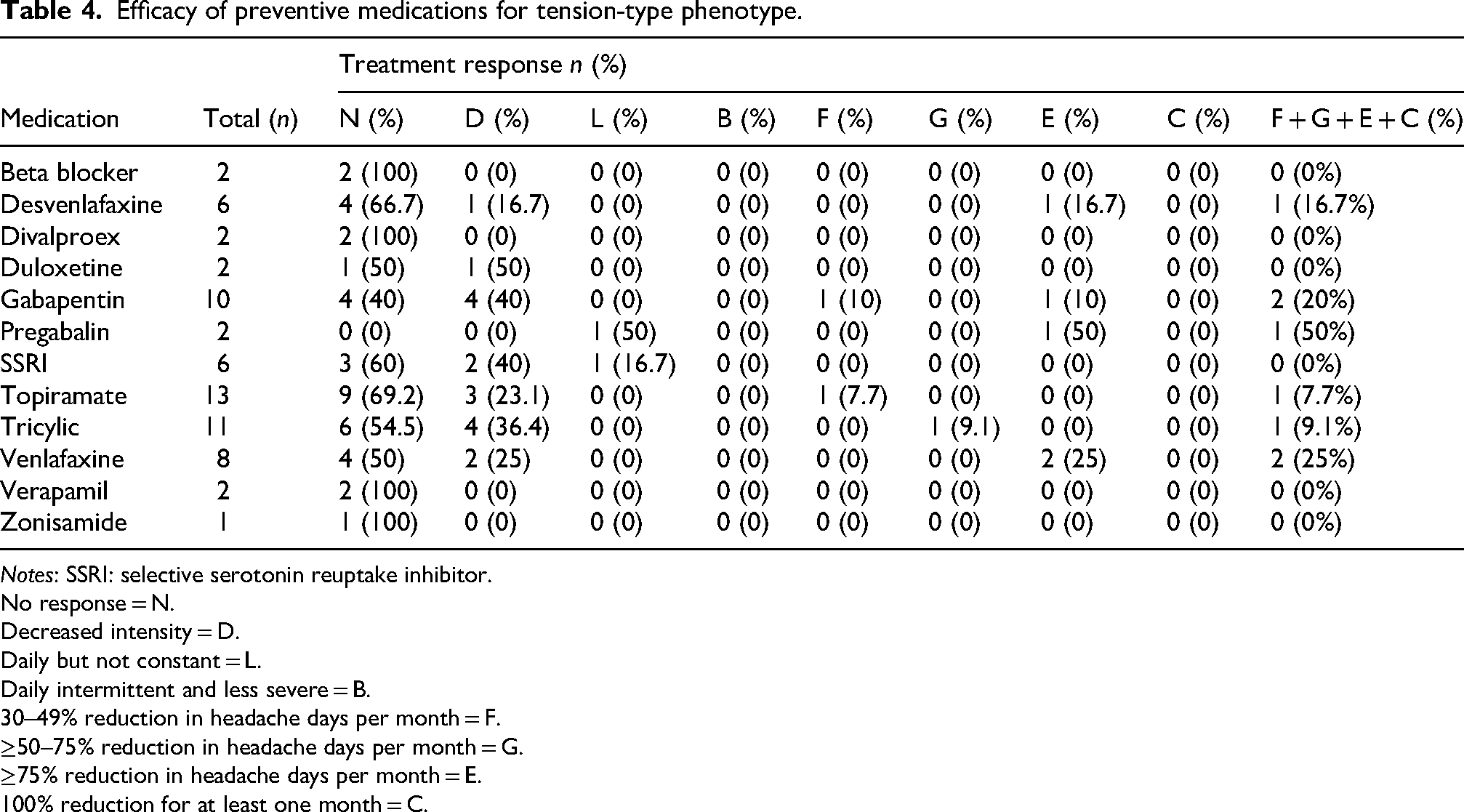
Notes: SSRI: selective serotonin reuptake inhibitor.
No response = N.
Decreased intensity = D.
Daily but not constant = L.
Daily intermittent and less severe = B.
30–49% reduction in headache days per month = F.
≥50–75% reduction in headache days per month = G.
≥75% reduction in headache days per month = E.
100% reduction for at least one month = C.
At the time of the first visit with RE, potential MOH was present in the MP and TTP patients, respectively, as follows: 11/260 patients (6 on opioids, 5 on triptans, and 4 on butalbital combinations) and 2/68 patients (both on butalbital combinations).
Twelve patients with the MP had an inpatient IV regimen. There was no response in 4 (33.3%). A 50% or greater reduction in moderate to severe days was reported in 41.7% following the treatment for the following number of days and patients, respectively: 3, 2; 21, 1; and 30, 2. Pain freedom was present in 16.7% as follows: seven days in one and 14 days in two patients.
Nineteen patients with MP had bilateral greater occipital nerve blocks (3 cc of 1% lidocaine) with 15 having no improvement. A 50% or greater reduction in moderate to severe pain days was reported by four (for seven days in three and one day in one patient).
Four patients with TTP had bilateral greater occipital nerve blocks with two having no improvement. A 50% or greater reduction of moderate to severe pain days was reported by two (for five days in one and 42 days in the other including 20 pain-free days).
Ten patients with MP had bilateral supraorbital, supratrochlear, auriculotemporal, and greater occipital nerve blocks with no response in eight and a 50% reduction of moderate to severe pain days in two patients (lasting two days and 30 days).
Four patients with TTP had bilateral supraorbital, supratrochlear, auriculotemporal, and greater occipital nerve blocks with no response in three and a 50% reduction of moderate to severe pain days lasting 25 days in one.
Nine patients with MP had surgical procedures. Bilateral occipital nerve decompressions in five with the following responses: none in two; daily but not constant in two, and decreased intensity in one. One patient each had the following operations with no benefit: bilateral greater occipital, supraorbital, and auriculotemporal decompression; occipital and supraorbital decompressions; left middle cranial fossa arachnoid cyst; and septoplasty.
Two patients with TTP had occipital nerve decompression with no benefit and one had sinus surgery with no benefit.
Discussion
WMH were present in 20.9% with MP which is less than in primary migraine and 18.0% with TTP which is similar to the prevalence in primary tension-type headaches.
WMH are common in primary migraine. In a meta-analysis of 30 studies, the pooled prevalence rate is 44% with common locations of frontal and parietal lobes. 4 In one study, WMH were present in 16% of those with tension-type headaches. 5
In a prior study of 97 NDPH cases, WMH were present in 13.4%. 6 Migraine-associated symptoms were present in 77% of the subgroup without and 46% of the subgroup with WMH. In another study of 136 patients with NDPH, white matter abnormalities were present in 18 (13.2%). 7
Similar to most prior studies, acute medications were minimally, if at all, effective for the MP (Table 1) and the TTP (Table 2). 8 One small study found some benefit for triptans for the MPH 9 while a large retrospective study found no benefit. 10 In a large retrospective study, triptans were less effective in NDPH than in chronic migraine and tension-type headache. 11 In an internet survey of 340 subjects with NPDH, the three most effective acute treatments reported were hydrocodone, dihydroergotamine injections, and tramadol. 12
For MP, desvenlafaxine, venlafaxine, and onabotulinumtoxinA were the most effective (Table 3) while venlafaxine was the most effective for TTP (Table 4).
Cheema et al. found a poor response to most preventive treatments for NDPH with the most effective, dosulepin, producing at least a 30% improvement in 45.6%. 11 Other studies have also found NDPH to be poorly responsive to preventive medications.7,13
Our study had few patients preventively treated with anti-CGRP medication reflecting the enrollment period of 1 September 2011 through 28 February 2020 (this class of medications first became available in April 2018). In a two-year study of refractory NDPH treated with erenumab every 28 days over a two- to three-year period, 34% (18/53) had an improvement in quality of life. 14 In the internet survey of 340 subjects with NPDH, the three most effective preventive treatments were eptinezumab, atogepant, and rimegepant. 12
In our MP cohort of 42 patients injected with onabotulinumtoxinA, 27.9% had a ≥ 30% reduction in all headache days. In the only prospective study, after two cycles of onabotulinumtoxinA, a ≥ 30% improvement in monthly moderate-to-severe headache days was reported in the following groups: NDPH (59 patients), 34.5%; daily chronic migraine (148 patients), 43.2%, and nondaily chronic migraine (84 patients), 51.2%. 15
Potential MOH was only present in 4.2% of those with MP and 2.9% with TTP. MOH has been previously estimated as occurring in 31% of adults. 8
Up to five-day inpatient intravenous regimens with dihydroergotamine produced temporary benefit in 41.7%. In a pediatric study, admission for DHE infusion produced ≥50% reduction in pain 29.4% and a full resolution in pain in 8% (although the duration of relief was not provided). 16
Occipital nerve and pericranial nerve blocks produced modest improvement in this cohort. However, other studies suggest a reduction in pain in up to 63% of cases.8,17
In this cohort, various surgical procedures were largely ineffective for NDPH. Anecdotal benefit has been reported for greater occipital nerve decompression. 18 There is little evidence documenting benefit of an implanted occipital nerve stimulator. 8
An open-label study suggests that 10 Hz repetitive transcranial magnetic stimulation delivered to the left prefrontal cortex for three consecutive days may produce a significant improvement in pain severity. 19
Strengths and limitations
This study provides valuable real-world evidence from one of the largest NDPH cohorts reported. A key strength is the separation of efficacy data for migraine and TTPs, which is a common and practical approach in headache specialty practices. This offers insights into treatment effectiveness for different presentations of this often disabling and refractory disorder. Similarly, the reports of the presence or absence of WMH also presents real-world findings on multiple MRI scanners and interpretations by multiple radiologists as common in clinical practice. An ideal future prospective WMH study would include imaging on 3 T scanners with interpretation by two blinded neuroradiologists with a third for arbitration using the Fazekas scale. This would allow for the detailed examination of WMH characteristics such as location and total volume, and their association with risk factors (such as vascular, gender, older age), treatment response, developing medication overuse, and by comparing groups with and without WMH.
The retrospective design and the lack of a standardized headache intake questionnaire may have introduced bias. The study was conducted at a single center, which may limit the generalizability of the findings. Outcome data may be inaccurate as headache diaries were not required and adherence with treatments was not confirmed except by asking the patient. Selection bias may be present since patients who stopped medication early due to either nonadherence or poor tolerability were not included in the analysis.
Although response to treatment based upon a retrospective chart review can provide valuable practice insights, the gold standard, of course, is a prospective placebo controlled randomized trial preferably with the use of standardized headache questionnaire, a quality of life measure, and electronic headache diaries. Longer durations of preventive treatment including at least 3 months for oral medications as tolerated (rather than at least six to eight weeks), three or four cycles of anabotulinumtoxinA (rather than at least two cycles), and six months of anticalcitonin gene-related peptide medications (rather than at least three months) might produce greater response rates. As only 17 of the 328 subjects were ages 12–17 when first seen by RE, the findings may not be applicable to children. The gold standard for assessment of WMH on MRI would be a prospective study on three Tesla scanners with standardized imaging protocols with central blinded review with comparison to primary migraine and tension type headache subjects.
Since all of the patients had an onset of their headaches in 2019 or earlier, there were no COVID-19 associated NDPH subjects. There is no prospective data on whether COVID-19 associated NDPH has a different response to treatment than primary NDPH.20,21
Conclusion
WMH in TTP occur with about the same frequency as primary tension-type headache but are present less often than in primary migraine. Treatment for MP and TTP remain challenging, with only modest benefit from acute and preventive medications. Future prospective randomized controlled studies and new treatments are needed to identify effective interventions for this disabling and refractory disorder.
Article highlights
WMH were present in 20.9% with MP (less than in primary migraine) and 18.0% with TTP (similar to primary tension-type headaches.
Acute medications were minimally, if at all, effective for the MP and TTP.
For prevention, desvenlafaxine, venlafaxine, and onabotulinumtoxinA were the most effective for MP and venlafaxine was the most effective for TTP
Footnotes
Consent to participate and institutional review board approval
An Independent Review Board exemption was obtained from Integ Review IRB (Protocol 1953). Consent waived, retrospective review.
Consent for publishing
Yes.
Author contributions
Equally shared.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Available from the corresponding author upon reasonable request.