
Abstract
Although new daily persistent headache (NDPH) is considered to be one of the most refractory headaches to pharmacological treatment, the effectiveness of drug-based treatment, and the prognosis of NDPH have not been well studied. The purpose of this study is to evaluate the effectiveness of pharmacological treatment of NDPH. Seventeen men and 13 women who met the IHS diagnostic criteria for NDPH, were treated for five years from November 1997 to October 2002, and whose headache conditions were entirely available for reference as of October 2003 were investigated in Toyonaka Municipal Hospital. Mean age at onset 35.0 years (range 13-73 years). The onset of headache occurred in relation to a stressful life event in six (20%) patients and any precipitating events could not be identified in 24 (80%) patients. For treatment, muscle relaxants were first administered and if no effect was observed, tricyclic antidepressants, selective serotonin reuptake inhibitors, and antiepleptic drugs were subsequently administered. Results of the drug-based treatments in the 30 cases were ‘very effective’ for eight (27%) cases, ‘moderately effective’ for one (3%) case, ‘mildly effective’ for six (20%) cases, and ‘not effective’ for 15 (50%) cases. According to the survey on the phone for the patients who did not improve to the level of ‘mildly effective’ or better and did not come back to our institution as of October 2003, there were no cases found to have spontaneously improved to the level of ‘mildly effective’ or better. These results suggest that NDPH is highly recalcitrant to the treatments with poor prognosis and better treatments are needed.
Introduction
New daily persistent headache (NDPH) is a headache characterized by acute onset (developing over <3 days) and persistency and it occurs in an individual who has scarcely had headache before from birth. The nature of the headache is similar to that of chronic tension-type headache (CTTH), but its acute onset is quite distinctive. There have been only a very few reports closely reviewing NDPH up to now, and not only its cause but also the details of effectiveness of drug-based treatment and of its prognosis are totally unknown. In this study we examined clinical features, effectiveness of drug-based treatment, and prognosis of 30 patients with NDPH whom we diagnosed, treated, and assuredly followed in our hospital.
Methods
The subjects of this study were 30 patients with NDPH (out of 1760 patients with chronic headache who were examined and treated in our hospital for five years from November 1997 to October 2002) who met the IHS diagnostic criteria for NDPH (1) with the duration of one year or more and whose headache condition was entirely available for reference as of October 2003. Secondary headaches (e.g. headache after head and neck injury, persistent headache after intracranial diseases, persistent headache after head and neck surgery, and headache associated with medication overuse fulfilling the IHS diagnostic criteria (1) recognized at the first examination) were excluded. Headache with possible chronic post-non-bacterial infection headache, which developed after viral infection, was also excluded.
For treatment, muscle relaxants (centrally acting: tizanidine, baclofen) were first administered and if no effect was observed, tricyclic antidepressants (amitriptyline), selective serotonin reuptake inhibitors (fluvoxamine, paroxetine), and antiepileptic drugs (valproic acid) were subsequently administered. Results of drug-based treatment were assessed by patients themselves based on the effectiveness in alleviating headache intensity, ranging from 0 (headache-free) to 10 (headache intensity patients always felt on average before treatment). Assessment criteria were: 3 or less for ‘very effective’, 4–5 for ‘moderately effective’, 6–7 for ‘mildly effective’, and 8–10 for ‘not effective.’ We also excluded the patients who did not improve to the level of ‘mildly effective’ or better, did not come back to our hospital as of October 2003 and did not assuredly answer to questions about their headache condition on the phone. Consequently, we selected a total of 30 patients and studied their clinical features, effectiveness of drug-based treatment, and prognosis.
Results
The clinical features and the effectiveness of treatment of all the cases are shown in Table 1. The total of 30 patients consisted of 17 male patients and 13 female patients with the average age being 38.1 years, and the age at the onset ranged form 13–73 years with the mean age at the onset being 35.0 years. The duration of headache ranged from three months to 27 years, and the mean morbidity period before consulting us was 39.5 months. Many of the male patients had the first episode in their 10s to 30s (Fig. 1).
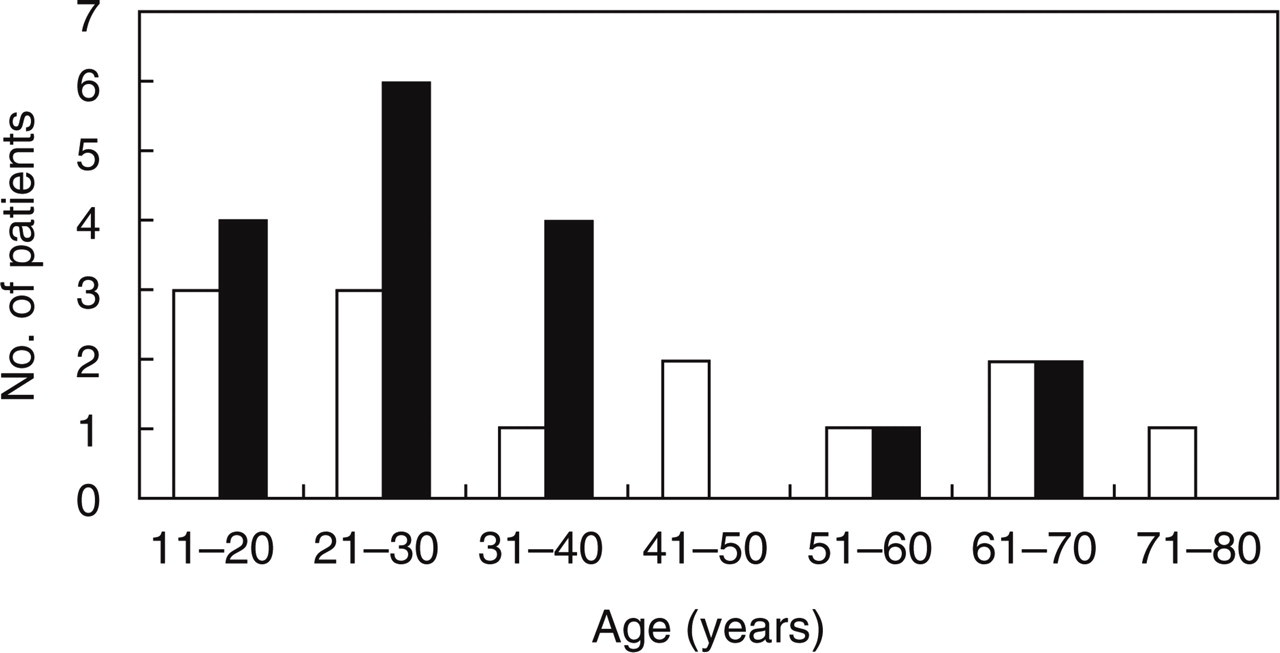
Age at onset; h female, ▪ male.
Clinical features and effectiveness of drug-based treatment
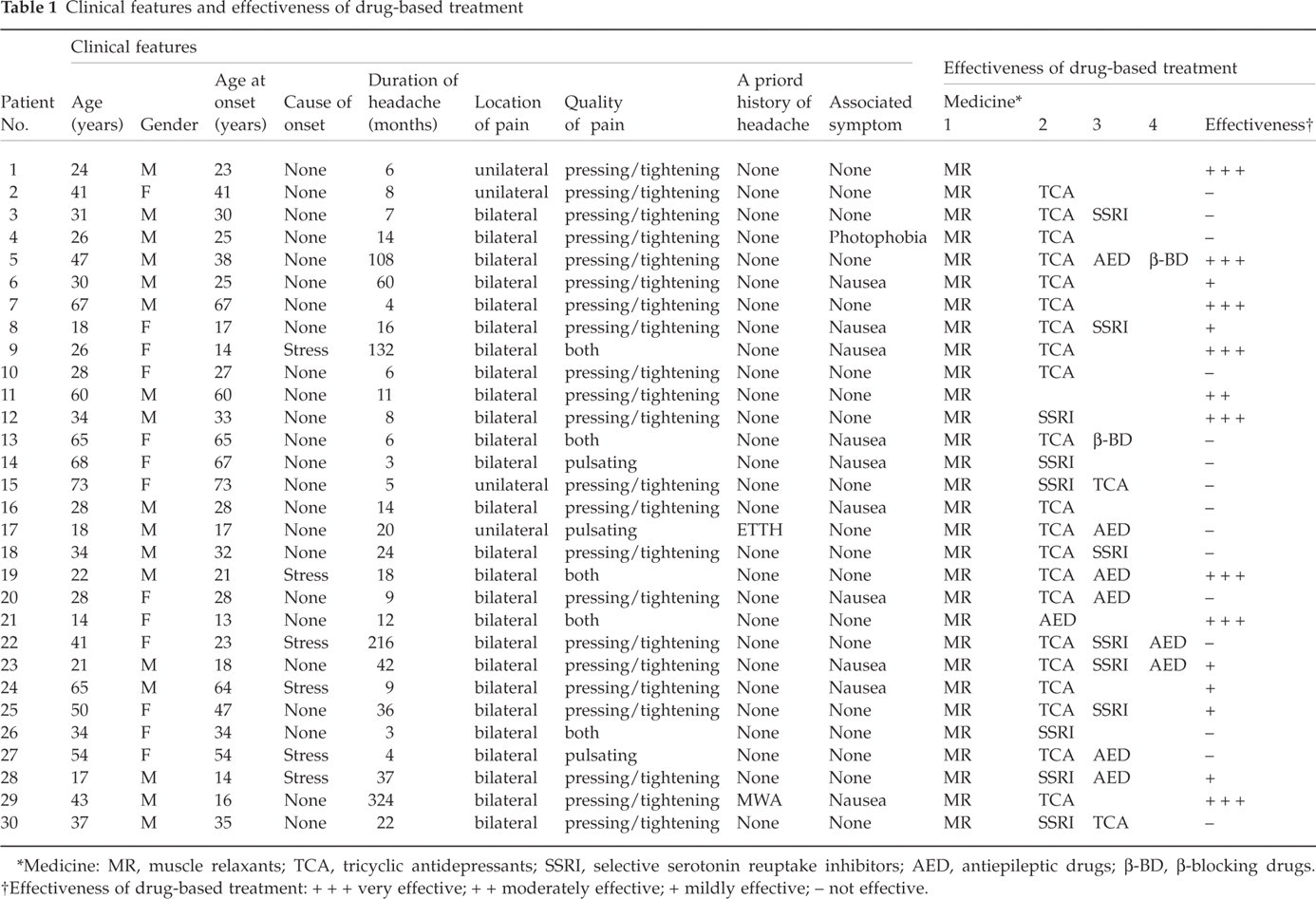
∗Medicine: MR, muscle relaxants; TCA, tricyclic antidepressants; SSRI, selective serotonin reuptake inhibitors; AED, antiepileptic drugs; β-BD, β-blocking drugs.
†Effectiveness of drug-based treatment: + + + very effective; + + moderately effective; + mildly effective; – not effective.
Regarding the cause of the headache, 24 (80%) patients elucidated no precipitating factors and six (20%) patients identified stress as a precipitating factor. Two patients had experienced several headaches before the onset of NDPH (episodic tension-type headache or migraine with aura), but 28 patients, the majority of the study population, had not had any history of headache before the first episode. In most cases the headache persisted all day long every day and most patients did not have any headache free time. All the patients complained of unbearable headache. The headache developed bilaterally in 26 patients and unilaterally in four patients, and its nature was pressing/tightening for 22 (73%) patients, pulsating for three (10%) patients, and both pressing/tightening and pulsating qualities for five (17%) patients. Associated symptoms were nausea (mild, only loss of appetite and not related with medication) in 10 (33%) patients and photophobia in one (3%) patient.
As for the treatment, muscle relaxants are generally administered first in Japan to treat the patients on the basis of the nature of the headache. In this study, if muscle relaxants were not effective (including noneffective cases treated by general practitioners or neurologists in other institutions), tricyclic antidepressants, selective serotonin reuptake inhibitors, and antiepileptic drugs were subsequently administered (Table 1). Results of the drug-based treatments in the 30 cases were ‘very effective’ for 8 (27%) cases, ‘moderately effective’ for 1 (3%) case, ‘mildly effective’ for 6 (20%) cases and ‘not effective’ for 15 (50%) cases (Fig. 2). In the 8 patients who had ‘very effective’ responses only 2 cases (No. 1 & 21) were cured of their headaches, and in the other six patients their quality of life improved as most likely they still remained with daily headache. Indomethacin was tried in one patient with unilateral, pulsating NDPH (No. 17), but it was not effective to the patient.

Effectiveness of drug-based treatment; ▪‘very effective’ for 8 (27%) cases, ‘moderately effective’ for 1 (3%) case, ░‘mildly effective’ for 6 (20%) cases, □‘not effective’ for 15 (50%) cases.
According to the survey on the phone for the patients who did not improve to the level of ‘mildly effective’ or better and did not come back to our hospital as of October 2003, there were no cases found to have spontaneously improved to the level of ‘mildly effective’ or better.
Discussion
Cases of NDPH are few in numbers with very rare previous reports. In the IHS classification of 2004 (1), NDPH was classified into the category of 4.8 as an entity distinct from CTTH. Li & Rosen (2) reviewed 56 cases of NDPH using diagnostic criteria of Silberstein et al. (3) and reported that headache onset occurred in relation to an infection or flu-like illness in 30%, exracranial surgery in 12%, a stressful life event in 12%, and 46% of the cases developed headache with no precipitating factors. We excluded persistent headache occurred in relation to an infection or flu-like illness because of possible chronic postnon-bacterial infection headache, which developed after viral infection. In our cases only six patients stated, ‘Stress seemed to induce the headache’, while cases without any precipitating factors accounted for 80%. It is completely unknown why the headache suddenly develops without any precipitating factors.
They also reported that NDPH was frequently seen in women, and persistent in nature with migraine-like symptoms (2). All the cases in this report had the disease history of six months or more. In our study, however, NDPH was rather seen more frequently in men (male to female ratio of 1760 patients with chronic headache in our hospital is approximately 3 : 7), and its location was bilateral with pressing/tightening quality in many of the patients. Only one patient suffered associated symptom of photophobia. The nature of the headache was similar to that of CTTH in many cases.
It is noted in the IHS classification of 2004 (1) that NDPH may take either of two subforms: a self-limiting subform which typically resolves without therapy within several months and a refractory subform which is resistant to aggressive treatment programmes. Vanest, the first reporter of NDPH, referred to the prognosis and commented that the headache spontaneously regressed within two years without any treatments in 86% of male patients and in 73% of female patients (4). In contrast, most of our cases had intense headache and were highly recalcitrant to the treatments with poor prognosis, though we cannot deny the possibility of spontaneous regression of the headache if we continue to follow the patients for a longer period of time.
The nature of the headache of NDPH is similar to that of CTTH, and if the headache is not alleviated by nondrug treatment, it is treated with medication. Results of the drug-based treatments were ‘very effective’ for 8 (27%) cases, ‘moderately effective’ for 1 (3%) case, ‘mildly effective’ for 6 (20%) cases, and ‘not effective’ for 15 (50%) cases, indicating that most cases were not very responsive. Evans & Rosen (5) are among those who do not think that NDPH is a disease with as favourable prognosis as Vanest reported, and they previously described that many of their cases had poor prognosis and were recalcitrant to treatments even if drugs for chronic daily headache including antidepressants and antiseizure agents were used. Our study showed comparable results with their study. The patients of NDPH have scarcely had headache before, and headache is daily and unremitting from very soon after onset. Therefore it is suggested that most of them cannot accept their headaches and most patients are not well responsive to medication. Rozen has recently reported on four cases for whom sufficient alleviation of the headache was obtained with gabapentin or topiramete (6), but gabapentin and topiramete are not currently available in Japan.
He also described that the patients with NDPH were very likely to recuperate if they were adequately treated well within one year of the onset (7). Our study, however, did not demonstrate such relationship between how promptly the treatments were taken after the onset and how effective the treatments were.
Goadsby & Boes (8) stressed the importance of correctly ruling out secondary headaches, including headache with intracranial hypotension and headache caused by idiopathic intracranial hypertension. Although we did not measure cerebrospinal fluid pressure by lumbar puncture in our 30 cases, we did not perform enhanced MRI because no patients were suspected to have low cerebrospinal fluid pressure syndrome. We also did not perform MRV looking for cerebral vein thrombosis. Our study did not include any obese women of 20–44 years of age who have frequently reported to suffer idiopathic intracranial hypertension in previous papers (9). But we have to consider that the refractoriness of NDPH in some of our patients could have been the result of missing a secondary cause although this was unlikely for most patients.
NDPH seems to be rare and incidence rate of NDPH is also entirely unknown. However, a great majority of the patients with NDPH are recalcitrant to therapy, thus prompting us to develop some novel treatments in the future.