
Abstract
Background
Orofacial migraine has been increasingly recognized and described in literature. The presence of orofacial migraine could be due to the radiation of migraine headache to the facial area, the development of new isolated facial migraines, or the relocation of prior migraine headaches to the facial region following nerve trauma.
Case
This report presents a patient who developed a novel orofacial migraine after an injury to the trigeminal nerve caused by the surgical removal of an impacted tooth. Initially diagnosed as post-traumatic trigeminal neuropathy, the pain later evolved to exhibit migraine-like characteristics. The patient had no prior history of migraine or other primary headaches. While the possibility of “novel-onset” post-traumatic orofacial migraine has been proposed, no cases have been documented in the literature.
Conclusion
Recognizing post-traumatic migraine in the orofacial region suggests a potential association between trigeminal nerve injury and the onset of new orofacial migraine and underscores the importance of accurate diagnosis and treatment among orofacial pain conditions.
This is a visual representation of the abstract.
Keywords
Background
Migraine is the second most common primary headache disorder after tension-type headache, affecting about 15% of the global population annually.1,2 According to the definition by the International Classification of Headache Disorders, 3rd edition (ICHD-3), migraine is a recurrent headache lasting 4–72 h, typically unilateral, pulsating, and of moderate to severe intensity. 3 It often worsens with physical activity and is accompanied by nausea, photophobia, or phonophobia. The ICHD-3 classifies migraine into three main types: without aura, with aura, and chronic. Migraine can significantly impact quality of life, with substantial personal and societal burdens.4–6
Migraine pain location can vary between individuals and across attacks in the same person. A population-based study of 517 people with migraine found that in 46 cases (8.9%), the head pain extended to the lower half of the face. 7 In a cohort of 1176 migraine patients, Lambru et al. identified 58 cases of isolated facial migraine, indicating a prevalence of approximately 5% among migraine sufferers. 8 Recently, the International Classification of Orofacial Pain (ICOP) has categorized this novel migraine presentation in orofacial regions as “orofacial migraine,” a subset of pain that resembles primary headache. 9 The ICOP classification applies to patients who develop new migraine in the facial region (maxillary division or V2, and mandibular division or V3, of the trigeminal nerve) rather than the typical head region (ophthalmic division of the trigeminal nerve or V1 area). The mechanism of orofacial migraine is not fully understood, but it likely involves the trigeminovascular system and central mechanisms. The somatotopic organization of the trigeminal nucleus caudalis suggests that stimulation of one branch of the trigeminal nerve can alter pain perception in other branches. 10
Although orofacial migraines are uncommon due to their atypical location, it is often misdiagnosed as another orofacial pain (OFP) condition.11,12 Aside from orofacial migraine, OFP includes a wide range of conditions affecting the face, mouth, and jaws, arising from dental, musculoskeletal, neuropathic, or idiopathic origins. The ICOP provides a structured framework dividing OFP into six categories: dentoalveolar disorders, musculoskeletal pain, neuropathic pain, cranial nerve (CN)-related pain, primary headaches presenting in the orofacial region, and idiopathic OFP. This classification helps clinicians systematically assess and differentiate pain types, enhances diagnostic accuracy, and guides appropriate treatment.
The evidence of two cases reporting their original migraine location remapped itself to the location of the face where the injury site was. 13 The fact that both patients reported the original migraine headache had totally resolved and been replaced by the orofacial variant suggests that this is indeed a post-traumatically relocated orofacial migraine. Additionally, 30% of orofacial migraine cases reported trauma-related onset 14 and 45% of patients in a study of 11 facial migraine cases had prior endodontic treatment at the affected site. 15 Some patients had a history of typical migraine headaches before the facial pain developed, supporting the idea that trauma may trigger migraine relocation rather than new-onset orofacial migraine. Therefore, to the best of the author's knowledge, there are no documented cases clearly reporting new-onset facial migraine without a prior history of typical migraine headaches following trauma which might be referred to as novel-onset post-traumatic orofacial migraine.
Our report presents the first documented case of novel-onset orofacial migraine following trigeminal nerve injury, also referred to as post-traumatic orofacial migraine. This case report aims to present a patient's clinical features who developed novel migraines following an injury to the trigeminal nerve and to demonstrate the potential mechanisms underlying trigeminal nerve injury-induced migraines.
Case presentation
The patient provided written informed consent for the publication of this report. The timeline of this case report is shown in Figure 1(a). A 38-year-old, Thai woman presented at the OFP clinic with intense, chronic dull, and burning pain with a numerical rating scale (NRS) of 8/10 at the upper left gingiva and teeth, in the area between maxillary left lateral incisor and maxillary left second premolar for a year (Figure 1(b)). The pain began about 7 months after her impacted upper left canine was removed due to an infection. Although the surgical wound had healed perfectly, she had persistent pain at the surgical site radiating to the left upper lip, lateral nasal wall, nasal ala, cheek, and lower eyelid (Figure 1(c)), with reported allodynia to light touch. The CN examination of other CNs revealed normal sensory and motor functions. There was no pain upon palpation of the temporomandibular joints (TMJs) or the masticatory muscles. At that time, the pain was not accompanied by any other symptoms.

(a) Timeline of events for this case report. (b–d) Mapping of the pain on the left side of the face in relation to the timeline. (b, c) Initial pain observed during the first visit, localized in the V2 region (grey). (d) Recurrent pain, which later extended to the temple area (green). (e, f) The pain from the latest visit was consistently menstrual-related, originating from the temple and radiating to the area between the wing of the nose and the upper lip on the left side. PPTTN: painful post-traumatic trigeminal neuropathy; V2: maxillary branch of the trigeminal nerve.
Prior to the referral to OFP clinic, the patient underwent endodontic treatment of the left maxillary lateral incisor and first and second premolars due to persistent postoperative pain (Figure 2(a, b)). The endodontic treatment did not alleviate the pain, despite confirmed treatment success on periapical radiographs and cone beam computed tomography (CBCT), no missed canals or signs of infection were found (Figure 2(c–h)). Consequently, the patient was referred to us to rule out nonodontogenic pain before final restorations on these root canal–treated teeth. Therefore, the OFP team initially diagnosed her dull and burning pain as painful post-traumatic trigeminal neuropathy (PPTTN) of the right V2 region due to impacted tooth surgery. The patient was prescribed daily doses of nortriptyline 10 mg and gabapentin 300 mg.

Periapical (a, b) and cone beam computed tomography (CBCT) (c–h) images of the endodontically treated teeth in the upper left maxilla: lateral incisor (a), first and second premolars (b and c) showing acceptable root canal fillings without periapical lesions (a, b). The CBCT images confirmed the absence of missed accessory canals and demonstrated complete filling of the root canals in all three teeth (c–e; axial view, f–h; sagittal view).
The patient was followed by the OFP team every 6 months. Over the course of 12 months, her burning pain gradually decreased from an NRS score of 8/10 to 2/10. During this period, she independently discontinued her medications, as the residual pain became manageable. At a follow-up visit in March 2024 (Figure 1), she reported 1–2 monthly episodes of recurrent pain with a different character—now described as throbbing, with pain intensity of 6/10 and without any constant background pain. The pain was in the same area, slightly extending upward along the buccal side of the gum from the first left premolar to the first molar, radiating to the upper cheek, orbit, and temple on the left side (Figure 1(d)). The pain typically lasted for 2 days (48 h) and was more severe during menstrual periods. She experienced nausea as an accompanying symptom with this pain and never had an aura or cranial autonomic symptoms. Bright light, heat, sleep deprivation, and stress often triggered and exacerbated pain. The patient denied a family history of headaches or any history of primary headaches. Intraorally, all dental restorations of involved teeth were within normal limits with normal alveolar bone support and surrounding soft tissue. Psychosocially, she reported significant work-related stress due to her roles as the head of nursing and as a researcher, which she identified as a trigger for her current pain. She observed that the pain did not occur (NPS = 0) when she was on holiday. The OFP team suspected that the recurrent pain following PPTTN was an OFP resembling migraine in the left V2 region. These episodes meet ICOP diagnostic criteria for the episodic orofacial migraine: recurrent OFP without head pain, 1–2 episodes per month lasting for 48 h, with a pulsating quality, moderate intensity, and associated with nausea and photophobia and constant pain from PPTTN had resolved. Menses, heat, sleep deprivation, and stress were not part of the diagnostic criteria but should be considered as aggravating factors. Therefore, the patient was referred to a neurologist for a definitive diagnosis of migraine. Additionally, we provided supportive treatments for her stress, including relaxation techniques and stress-reducing exercises.
After seeing a neurologist, she received a confirmed diagnosis of migraine without aura and was prescribed gabapentin 300 mg once daily at bedtime, nortriptyline 10 mg once daily at bedtime, propranolol 10 mg twice daily after meals, and ibuprofen 400 mg three times daily after meals. However, she reported that the combination of nortriptyline and gabapentin had recently been sufficiently effective, and the pain had significantly subsided. Six months later, she returned to the OFP clinic for a follow-up. The pain remained in the same area (Figure 1(e, f)) and always intensified each month around her menstrual period, lasting about 1 week. During this time, she managed it with ibuprofen, nortriptyline, and gabapentin but did not need any medication for the remaining 3 weeks. She also became highly capable of managing stress independently and effectively.
Discussion
This case report aims to present a case of new-onset orofacial migraine induced by an injury to the trigeminal nerve by a dental procedure. However, no direct trauma to a major trigeminal nerve branch was identified during the removal of the impacted tooth, and no sensory loss in the corresponding dermatome was observed. Impacted teeth, including canines, are often removed to prevent potential complications such as cyst formation, root resorption of adjacent teeth, or infection. The removal of an impacted canine can range from a simple to a complex surgical procedure, depending on the depth, position, and angulation of the tooth. Deeper impactions may require flap elevation, bone removal, and sectioning of the tooth to facilitate extraction. It is important to recognize that postoperative factors such as surgical manipulation and infection may contribute to, or even mimic, persistent facial pain. Therefore, these possibilities should be thoroughly evaluated and carefully ruled out.
Post-traumatic trigeminal neuropathy occurs following direct or indirect injury or trauma to the trigeminal nerve, which provides sensation to the face, including the teeth, jaw, and surrounding areas. 16 This type of neuropathy can develop after dental procedures, facial trauma, or surgery involving the nerve. 16 The diagnosis of PPTTN was made for this patient because of the spontaneous neuropathic-like pain in the surgical area, related to surgical event, and the recurrent infection was excluded as a cause. The radiating pain in the V2 area was attributed to the injury of superior alveolar nerve, a branch of the infraorbital nerve. Damage to the branches of the infraorbital nerve, which supplies sensation to the skin of the upper lip, cheek, lateral aspect of the nose, and ipsilateral maxillary teeth, could be the cause of the patient's radiating pain. 17
Before the patient was referred to the OFP team, her three teeth underwent root canal treatment as the pain was initially misdiagnosed as dental pain, but this treatment failed to alleviate the pain. Several cases have been reported where the misdiagnosis of nonodontogenic facial pain as odontogenic pain led to inappropriate treatment, such as unnecessary root canal treatment 18 or tooth extractions. 19 The lack of a thorough history taking and examination and failure to recognize nonodontogenic pain may have contributed to unnecessary and potentially irreversible treatments for the patient and may further aggravate the trigeminal nerve.
This case did not meet the criteria for chronic migraine or pure menstrual migraine, nor did it fulfill the ICHD-3 criteria for primary migraine with headache. The patient experienced fewer than 15 migraine days per month, with pain localized to the facial and temporal regions. While the attacks were associated with menstruation, she also reported mild migraine symptoms on nonmenstrual days. Therefore, we propose that the patient's symptoms are best understood as a secondary form of episodic orofacial migraine associated with menstruation that developed following the resolution of PPTTN. Her pain presentation is consistent with findings from a previous study, in which 66% of patients with isolated facial migraine were diagnosed with episodic migraine. 8 In that study, the pain was most commonly located in the maxillary region (85%) and was strictly unilateral in 79% of cases. 8 Other potential sources of OFP were systematically ruled out. Dentoalveolar pain was excluded due to the absence of caries, periodontal diseases, or tenderness on percussion. Plain radiographs and CBCT imaging showed no periapical abscesses, excessive root canal fillings, or extruded materials, ruling out periapical infections or root canal treatment complications. These findings supported a nondental origin of the pain. Postsurgical inflammation was also excluded, as there were no signs of localized swelling, redness, warmth, or systemic symptoms such as fever during follow-up. There were no signs of temporomandibular disorders, such as restricted jaw movement or tenderness over the masticatory muscles or TMJs.
In addition to PPTTN and orofacial migraine, other differential diagnoses should be considered when evaluating OFP. Persistent idiopathic facial pain, previously termed atypical facial pain, presents as constant, poorly localized facial pain without clinical findings. This diagnosis is less likely in our case due to the episodic and throbbing nature of the symptoms, as well as the clear association with an identifiable cause. Orofacial complex regional pain syndrome, which can occur after injury; however, the absence of signs such as edema, or skin changes makes it unlikely. Persistent idiopathic dentoalveolar pain or atypical odontalgia may present as persistent pain in a tooth or gum without clinical cause, but it typically lacks migraine-like features. Trigeminal autonomic cephalalgias and trigeminal neuralgia (TN) were also considered but excluded due to the absence of autonomic symptoms or the brief, electric shock-like pain typical of TN. Overall, the clinical presentation most closely aligns with episodic orofacial migraine, as defined by ICOP.
When migraines develop novel-onset after injury, particularly in this patient who had no prior history of such headaches, it raises significant clinical and scientific interest. Head trauma has been reported as a potential initiating or aggravating factor for typical migraines.20,21 However, there have been no reports association of trigeminal nerve injury in the orofacial area to the onset of novel orofacial migraines as presented in our report. As mentioned earlier, previous case reports and studies have also described orofacial migraines associated with trauma,13–15 but in their cases, patients experienced migraine headaches prior to the injury, after which the migraines either disappeared or relocated to the orofacial region and should be called as post-traumatically relocated orofacial migraine. 22 In contrast, the patient in this case report presented with no history migraine and the onset of novel orofacial migraine developed following a trigeminal nerve injury in the orofacial region. The proposed differentiation of novel-onset post-traumatic orofacial migraine and post-traumatically relocated orofacial migraine is shown in Figure 3.
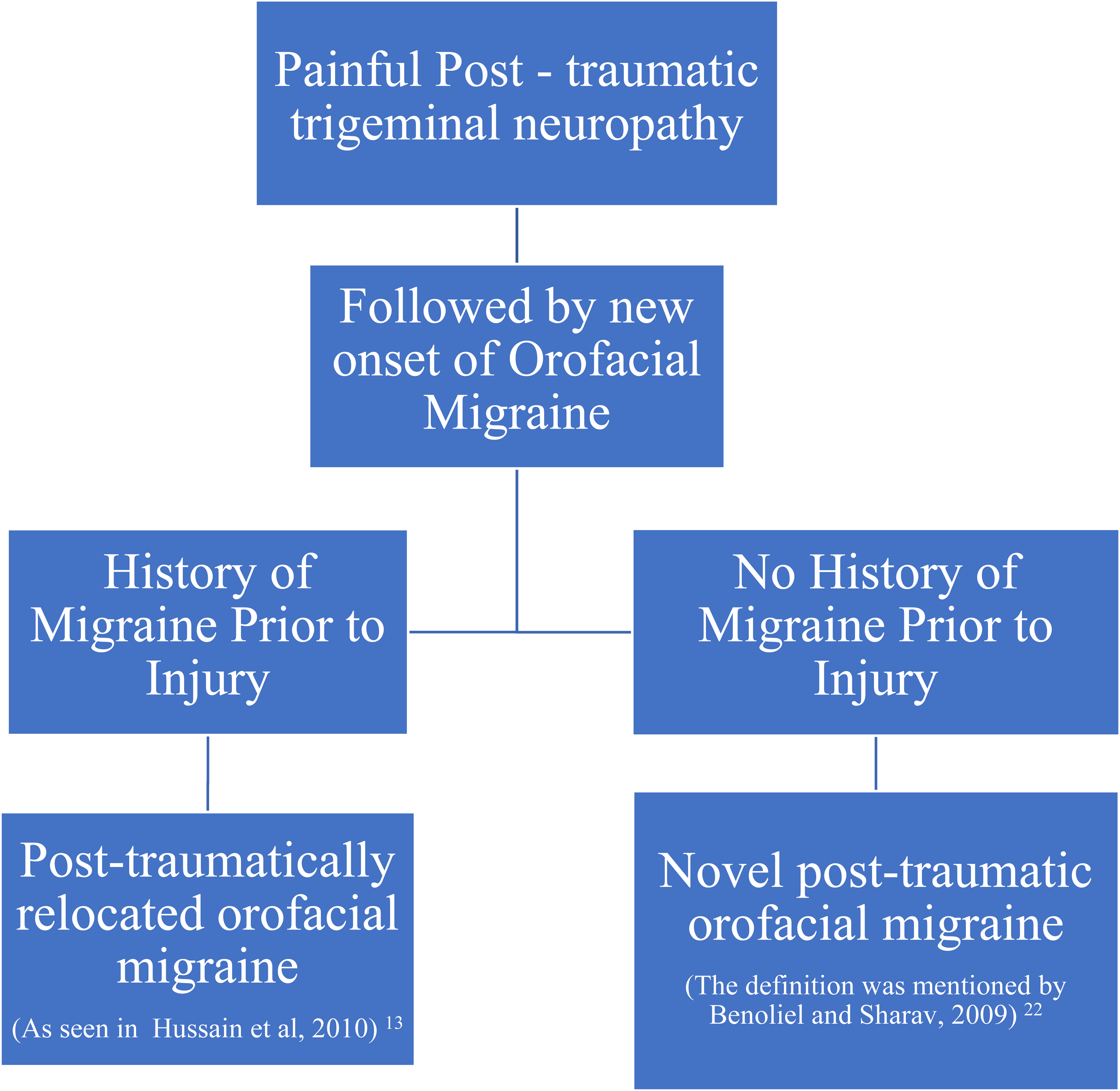
Diagnostic flowchart for differentiating post-traumatic orofacial migraine.
The phenomenon of novel-onset post-traumatic orofacial migraine suggests a potential link between the trigeminal nerve trauma and the onset of migraine symptoms. The involvement of the trigeminal nerve in migraine pathogenesis is well-documented, with evidence suggesting that activation of the trigeminovascular system plays a pivotal role in migraine initiation. 23 The author outlines potential mechanisms through which PPTTN may trigger or exacerbate migraine, with trigeminal nerve hyperexcitability proposed as a primary factor. When this nerve experiences trauma, it can initiate a neuroinflammatory response that leads to hyperexcitability, causing it to become increasingly sensitive to stimuli. 10 Increased peripheral input from the second and third trigeminal divisions after facial or oral injury may alter central pain processing, potentially reorganizing migraine pathways and underpinning the mechanism of central sensitization. 13 Central sensitization was proved to play a role in post-injury pain hypersensitivity. 24 Clinically, it presents as lowered pain thresholds and amplified responses, 24 often referred beyond the original injury site—consistent with the observed shift of migraine pain to the orofacial region. Neuropathic irritation can further stimulate migraine circuits. Supporting evidence includes nasopharyngeal stimulation triggering migraines 25 and both mechanical and chemical stimuli activating the trigeminal system in migraine sufferers. 26
In terms of medication management, the use of gabapentin, nortriptyline, and ibuprofen for only one week per month was not part of a formal medical plan. Instead, the patient adjusted her medication use on her own through trial and error, based on symptom relief and tolerability. Although unconventional, she reported this intermittent schedule to be the most effective with minimal side effects. This regimen was later discussed with the OFP and neurology teams, who acknowledged her positive response but did not formally recommend this approach. The combined use of nortriptyline and propranolol as preventive medications was started under the guidance of her neurology team to help manage migraine as a single preventive agent might not provide sufficient relief. However, whether monotherapy or combination therapy is used depends on the physician's clinical judgment at the time, based on what is believed to offer the greatest benefit for the patient. Nortriptyline is considered effective in PPTTN due to its dual role as an analgesic and neuromodulator and is also commonly used as a migraine preventative. 16
However, some clinical features in this patient warrant careful consideration. Firstly, the patient's age at the onset of new migraine episodes was slightly higher than the median age associated with migraine onset which was 25 years among women. 10 This atypical timing, following a documented trigeminal nerve injury, supports a secondary or post-traumatic etiology rather than a primary migraine. Secondly, the occurrence of orofacial migraine in the same anatomical division as the PPTTN raises important questions about the underlying mechanisms that remain unexplained. If the trigeminal nerve is hyperexcited due to injury, it is plausible that migraine pain could manifest not just in the areas associated with nerve injury but also in any other regions innervated by the trigeminal nerve.
Conclusions
This case report emphasizes the potential occurrence of new orofacial migraines related to trigeminal nerve injury. The complexity of symptoms and the rarity of such presentations underscore the importance of a thorough diagnostic process and a holistic treatment approach. An integrated care is essential to identify all contributing pain sources and deliver targeted interventions that enhance the patient's overall quality of life.
Clinical implications
Trigeminal nerve injury may trigger new-onset orofacial migraine.
Insufficient evaluation of nonodontogenic pain risks unnecessary treatments.
Footnotes
Acknowledgments
The authors express our sincere gratitude to the patient for their invaluable contribution.
Author contributions
All authors participated in data collection. PY drafted the primary manuscript, and all authors contributed to manuscript revision and submission.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written consent was obtained from patient.