
Abstract
Background
Reversible cerebral vasoconstriction syndrome (RCVS) is a transient cerebrovascular disorder characterized by multifocal segmental narrowing of cerebral arteries, often presenting with thunderclap headaches. Known triggers include physical exertion, emotional stress, vasoactive substances, and sexual activity. However, the role of sexual devices in precipitating RCVS has not been documented.
Case
We describe a 50-year-old woman with well-controlled hypertension and noninsulin-dependent diabetes mellitus who experienced recurrent thunderclap headaches triggered by an orgasm following the use of a sexual device. Neurological examination and lumbar puncture were unremarkable. Magnetic resonance imaging and digital subtraction angiography revealed multifocal arterial narrowing, consistent with RCVS. The patient was treated with oral Nimodipine, leading to complete symptom resolution. A one-year follow-up angiography demonstrated full recovery.
Conclusions
This case highlights the potential for intense sexual stimulation via a device to act as a previously unrecognized trigger for RCVS. Given the widespread use of sexual devices, healthcare providers should consider this association when evaluating patients with orgasm-induced thunderclap headaches. Further research is needed to understand the mechanisms underlying this phenomenon and to improve patient counseling and management.
This is a visual representation of the abstract.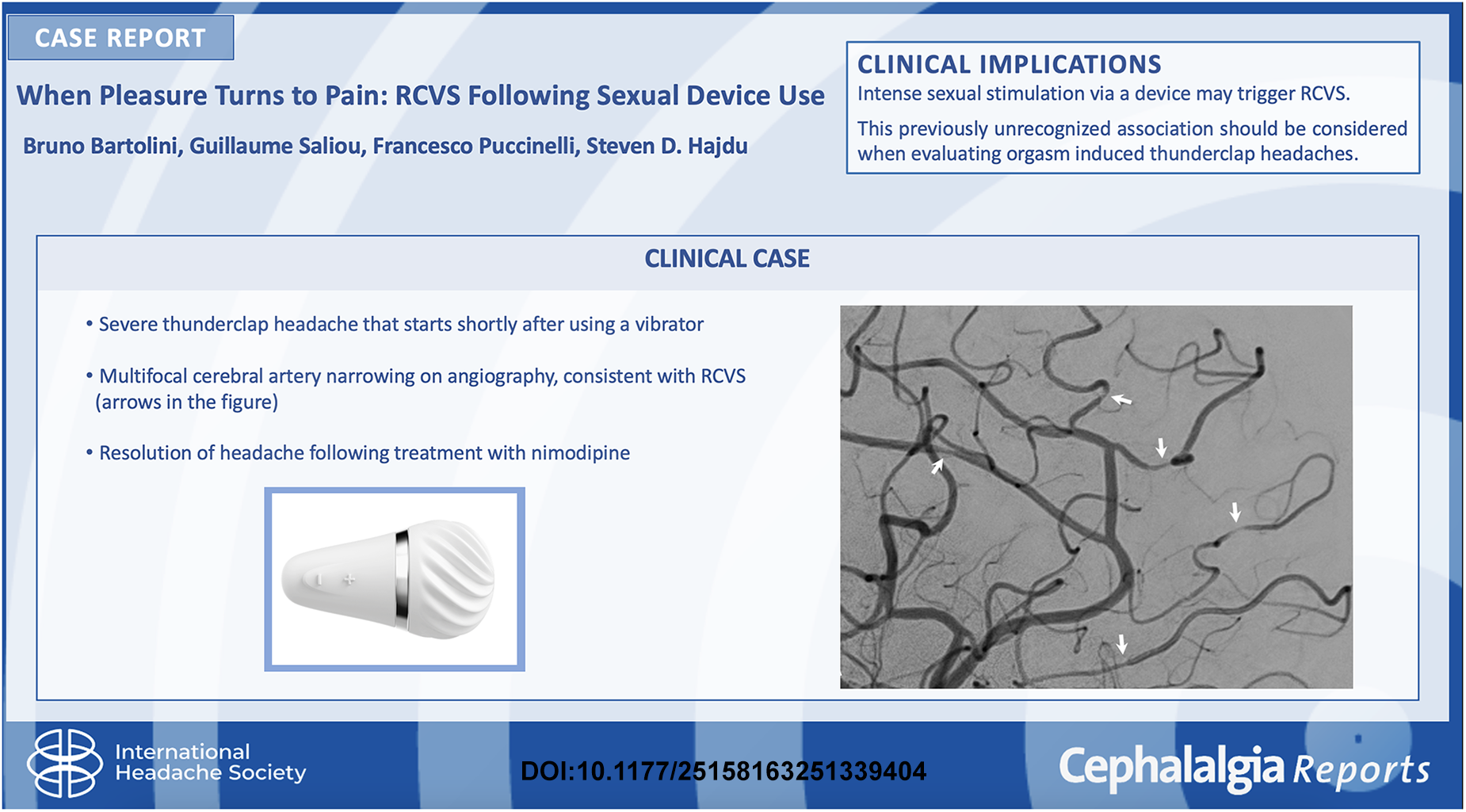
Keywords
Introduction
Reversible cerebral vasoconstriction syndrome (RCVS) is a transient cerebrovascular disorder characterized by multifocal segmental narrowing of cerebral arteries, which resolves within three months. RCVS typically presents with recurrent thunderclap headaches, often triggered by various stressors, including sexual activity, exertion, emotional stress, or vasoactive substances. 1 While orgasmic headaches have been reported, the association between RCVS and sexual activity remains poorly understood. The pathophysiology of RCVS is thought to involve dysregulation of cerebral vascular tone, possibly due to heightened sympathetic activity or reduced parasympathetic modulation.2,3 The role of external factors, such as the use of sexual devices, in triggering RCVS has not been previously documented. Here, we present a novel case of RCVS occurring in a 50-year-old woman following the use of a sexual device during clitoral stimulation, highlighting a potential new trigger for this condition.
Case
A 50-year-old sexually active woman, with a history of well-controlled hypertension and noninsulin-dependent diabetes mellitus, presented to the emergency department with three episodes of thunderclap headache over 48 h. The headaches were triggered by an orgasm experienced during the use of a sexual device (Satisfyer Little Wand, Triple A Import GmbH, Bielefeld, Germany) for clitoral stimulation (Figure 1). She described the orgasm as significantly more intense than usual, followed immediately by an excruciating headache lasting two hours. Similar headaches spontaneously reoccurred at 12 and 48 h after initial symptom onset. The patient denied any prior history of headaches during sexual activity and reported no recent medication changes or use of illicit substances such as cannabis or cocaine.

The sexual device used in this case is a compact, handheld device designed for clitoral stimulation. It features a flexible silicone head, multiple intensity levels (ranging from low to high vibration frequencies), and a rechargeable power source via USB (Triple A Import GmbH, Bielefeld, Germany).
Neurological examination and lumbar puncture were unremarkable. Initial brain magnetic resonance imaging (MRI) demonstrated multifocal constriction and dilatation of cerebral arteries without signs of acute hemorrhage. Arterial wall imaging did not reveal any contrast enhancement. To further assess the extent of vasoconstriction and rule out alternative vascular pathologies, digital subtraction angiography was performed, offering high-resolution imaging to refine the diagnosis and guide management. The findings confirmed the MRI results, revealing focal and marked caliber changes in the distal branches of the anterior and middle cerebral arteries (Figure 2A, B). The patient was treated with oral Nimodipine 30 mg/day for 14 days, leading to complete symptom resolution. The patient was advised to gradually resume sexual activity while monitoring for symptom recurrence. At her follow-up, she reported engaging in sexual activity, both with a partner and through self-stimulation, without experiencing any new headaches.

Cerebral digital subtraction angiography (DSA) at initial presentation (A and B) and at one-year follow-up (C and D). Initial imaging (A and B) reveals multifocal arterial constrictions and segmental dilatations, with marked caliber changes in the branches of the anterior and middle cerebral arteries (white arrows). At one year follow-up (C and D), these vascular abnormalities have completely resolved, demonstrating the reversible nature of the vasoconstriction.
A one-year follow-up brain angiography demonstrated complete resolution of all vascular abnormalities (Figure 2C, D). Based on these findings, a diagnosis of RCVS triggered by an intense orgasm during sexual device use was made.
Discussion
This case represents the first documented instance of RCVS occurring secondary to the use of a sexual device. While sexual activity has been previously suggested as a potential trigger for RCVS, 2 this case underscores the need to recognize sexual devices, such as vibrators as a possible contributing factor.
RCVS has an unclear etiology in many cases, making it a challenging diagnosis. It predominantly affects women between the ages of 20 and 50, a demographic that closely overlaps with vibrator users. 4 Studies estimate that more than 50% of women in this age group have used vibrators yet the role of sexual devices in triggering RCVS has never been systematically explored. 5 Given the sensitive nature of sexual health discussions, it is likely that vibrator use is frequently omitted during routine medical history-taking, potentially leading to under-recognition of this association.
RCVS triggered by sexual activity is not uncommon. A 2010 prospective study reported that RCVS accounted for up to 90% of secondary headaches linked to sexual activity. 6 This association aligns with findings from Frese et al., who reported that 35% of headaches associated with sexual activity were triggered by masturbation, reinforcing the role of orgasm itself as the key precipitant of thunderclap headaches, regardless of the specific sexual activity. 7 The autonomic dysregulation observed in RCVS may be explained by increased sympathetic drive and reduced parasympathetic modulation during sexual stimulation. 3 Given the overlapping demographics of RCVS and sexual device users, future research should explore the potential relationship between these factors in greater detail.
The implications of this case extend beyond its novelty, highlighting the importance of detailed sexual history-taking in patients presenting with thunderclap headaches. Due to embarrassment or stigma, patients may be reluctant to disclose details of their sexual practices, necessitating an open and nonjudgmental clinical approach. 8 Raising awareness among healthcare providers can lead to improved recognition of RCVS cases associated with sexual device activity and mitigate misdiagnoses.
Currently, there is no literature explicitly linking vibrator use to RCVS. This suggests that cases like the one presented here may be underreported. Future studies should explore the possible association between sexual device use and cerebral vasoconstriction, particularly in individuals who experience thunderclap headaches following orgasm. A deeper understanding of the underlying mechanisms, particularly the interplay between autonomic function, vascular tone, and sexual activity, may provide key insights into RCVS pathophysiology.
Additionally, understanding the full spectrum of sexual activity-related triggers may help prevent future occurrences. Patients diagnosed with RCVS should be counseled on potential risk factors, including excessive sympathetic stimulation, and guided toward preventative strategies such as gradual arousal techniques, relaxation strategies, and avoidance of excessive sexual stimulation that could exacerbate the syndrome.
Future research should not only focus on vibrator use as a potential risk factor but should also explore whether different types of sexual activity, frequency, and intensity play a role in cerebral vasospasm development. Prospective studies and case series could provide valuable data on whether certain individuals are predisposed to developing RCVS secondary to sexual activity.
This case expands our understanding of RCVS triggers and highlights the importance of considering sexual device use in the differential diagnosis of orgasmic headaches. Future research is needed to further elucidate the mechanisms linking sexual stimulation, sympathetic overactivation, and cerebral vasoconstriction.
Clinical implications
This case highlights the potential for intense sexual stimulation via a sexual device to act as a previously unrecognized trigger for RCVS. Healthcare providers should consider sexual device use when evaluating patients presenting with thunderclap headaches following orgasm. Due to the sensitive nature of sexual health, clinicians should adopt an open and nonjudgmental approach to patient history-taking. Future research should investigate the potential mechanisms linking sexual device use, autonomic dysfunction, and cerebral vasoconstriction. Increased awareness of this association may help prevent misdiagnosis and unnecessary interventions.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The patient provided written informed consent for the publication of this case report.