
Abstract
Introduction
To describe clinical, neuroimaging, and laboratory features of a large cohort of Italian patients with reversible cerebral vasoconstriction syndrome.
Methods
In the setting of the multicenter Italian Project on Stroke at Young Age (IPSYS), we retrospectively enrolled patients with a diagnosis of definite reversible cerebral vasoconstriction syndrome according to the International Classification of Headache Disorders (ICHD)-3 beta criteria (6.7.3 Headache attributed to reversible cerebral vasoconstriction syndrome, imaging-proven). Clinical manifestations, neuroimaging, treatment, and clinical outcomes were evaluated in all patients. Characteristics of reversible cerebral vasoconstriction syndrome without typical causes (“idiopathic reversible cerebral vasoconstriction syndrome”) were compared with those of reversible cerebral vasoconstriction syndrome related to putative causative factors (“secondary reversible cerebral vasoconstriction syndrome”).
Results
A total of 102 patients (mean age, 47.2 ± 13.9 years; females, 85 [83.3%]) qualified for the analysis. Thunderclap headache at presentation was reported in 69 (67.6%) patients, and it typically recurred in 42 (60.9%). Compared to reversible cerebral vasoconstriction syndrome cases related to putative etiologic conditions (n = 21 [20.6%]), patients with idiopathic reversible cerebral vasoconstriction syndrome (n = 81 [79.4%]) were significantly older (49.2 ± 13.9 vs. 39.5 ± 11.4 years), had more frequently typical thunderclap headache (77.8% vs. 28.6%) and less frequently neurological complications (epileptic seizures, 11.1% vs. 38.1%; cerebral infarction, 6.1% vs. 33.3%), as well as concomitant reversible brain edema (25.9% vs. 47.6%).
Conclusions
Clinical manifestations and putative etiologies of reversible cerebral vasoconstriction syndrome in our series are slightly different from those observed in previous cohorts. This variability might be partly related to the coexistence of precipitating conditions with a putative etiologic role on disease occurrence.
Introduction
Reversible vasoconstriction syndrome (RCVS) is a clinical and radiological entity characterized by recurrent severe thunderclap headaches (TCHs) with or without other neurological deficits and diffuse segmental vasoconstrictions of the cerebral arteries which resolve spontaneously within 3 months (1,2). Although the disease is increasingly recognized as a medical condition in the literature, mostly because of the routine availability of non-invasive imaging including computed tomography angiography (CTA), magnetic resonance angiography (MRA), and transcranial Doppler (TCD) (1,3,4), the reports from large case series remain limited and are predominantly from sparse main groups in France, the US, Taiwan, and Korea (5–11). Furthermore, since the clinical and radiological features of the disease derived from the series reported to date are far from being homogeneous, there is a clear need for more detailed data from large patient cohorts. Therefore, in the present study, we sought to determine the clinical characteristics, risk factors, triggering conditions, as well as detailed neuroimaging and laboratory features of RCVS from a large series of Italian patients recruited in the setting of the Italian Project on Stroke at Young Age (IPSYS).
Methods
Study design and study population
The IPSYS is a countrywide network of neurological centers with special interest in cerebral vascular disease at young age across Italy, aimed at recruiting Caucasian patients with first-ever acute vascular events in the setting of a hospital-based, multi-center, observational study (12). For the purpose of the present study, we retrospectively identified consecutive patients with RCVS regardless of whether they had a stroke or not, at institutions included in the IPSYS network, which serve as referral centers for acute neurological diseases. The recruitment period was January 2011 through January 2018. We diagnosed RCVS patients among those who visited the outpatient headache clinic or the emergency unit, were admitted to the stroke unit or the neurology ward or underwent in-patient consultation in each center. The performance of noninvasive brain vascular imaging investigations (TCD, CTA, or MRA) or conventional cerebral angiography was left to the discretion of the investigator in charge of the patient, when the latter presented with TCH or any acute, severe, persistent or recurrent headache of recent onset not fulfilling the criteria for primary headaches, regardless of concomitant focal neurologic deficit and/or other neurologic manifestation, or cryptogenic stroke. In those cases where imaging findings prompted suspicion of RCVS, a follow-up visit and MRA or CTA to determine the reversibility of intracranial vasoconstriction were scheduled at 3 months after onset. In the present analysis, we included only patients who met the criteria for definite RCVS according to the third edition of the International Classification of Headache Disorders, beta version (ICHD-3 beta)(13). Cases of probable RCVS, that is, patients who had had recurrent, triggered TCHs typical of RCVS but with normal cerebral angiography, did not qualify for the analysis. The study complies with the Declaration of Helsinki. All aspects of the study were approved by the Ethics Committee of the coordinating Center (University of Brescia) and of each study site. Written informed consent was obtained from all patients (or next of kin).
Risk factor definition
Hypertension was defined as systolic blood pressure ≥140 mm Hg and diastolic pressure ≥90 mm Hg in two separate measurements after the acute phase or use of antihypertensive drugs before recruitment. Diabetes mellitus was defined as a history of diabetes mellitus, use of hypoglycemic agent or insulin, or fasting glucose ≥7.0 mmol/L. Smoking history was defined as “current smoking”, including former smokers who had quit smoking for 6 months before the index event, versus “ever smoking” or “never smoking”. Hypercholesterolemia was defined as cholesterol serum levels ≥5.7 mmol/L or use of cholesterol-lowering drugs. Current use of oral contraceptives included current users as well as former users who had quit taking these medications for 1 month before the index event. We also collected information on alcohol consumption, personal history of coronary artery disease (history of physician-diagnosed angina or myocardial infarction) or other heart disease, as well as any vascular disease before the index event. Personal history of migraine was assessed in all patients by study physicians during a face-to-face interview in both the acute phase and follow-up evaluations, according to the diagnostic criteria of the International Headache Society (12,14).
Trigger factors
Based on the individual history of specific precipitating factors with a clear temporal association with the disease occurrence, in agreement with previous reports (7), RCVS was qualified as secondary or idiopathic. Secondary RCVS were cases in whom any conditions that have been reported in the literature as accepted causes of RCVS (i.e. postpartum status or use of serotonergic or adrenergic medications) were identified, while idiopathic RCVS were those in whom the above-mentioned conditions could not be detected.
Clinical features
We collected the following data: recent pregnancy and delivery, use of vasoactive and serotonergic medications or any other medication taken within 15 days before disease occurrence, and detailed characteristics of present headaches and any neurological symptoms. In particular, headache intensity was evaluated by using a verbal scale ranging from 0 (no pain) to 10 (the maximum pain that you can ever imagine). Headaches reaching a maximum intensity above 7/10 in less than 1 min qualified as TCH. Information on duration of symptoms prior to establishment of diagnosis, date of established diagnosis, presence of neurological complications (i.e. seizures, ischemic stroke, intracranial hemorrhage, or posterior reversible encephalopathy syndrome (PRES)) or clinical worsening after diagnosis, and treatments were also collected. Any recurrence of TCH or development of new neurological deficits after treatment and timing of these events were recorded at three-month follow-up.
Radiological and laboratory data
Brain imaging findings and non-invasive and conventional angiography imaging results on diagnosis and on eventual clinical worsening, as well as time to angiography, were also collected. Biological data included results from cerebrospinal fluid (CSF) analysis.
Statistical analyses
Descriptive statistics are presented as mean ± standard deviation or number (percentage). We compared patients’ characteristics by subgroups defined by presumed etiology (idiopathic vs. secondary RCVS) as well as by personal history of TCH at disease onset (RCVS with TCH vs. RCVS without TCH) using the χ2 test and Fisher’s exact test for categorical variables and the Student’s t-test for continuous variables. p ≤ 0.01 on two-sided test was considered significant. Data were analyzed using the SPSS (version 21.0) software package (www.spss.com).
Results
Baseline demographic characteristics of the study group.

Low alcohol intake was defined as up to seven drinks per week, moderate intake as 7–14 drinks per week for women or 7–21 drinks per week for men, and high intake as more than 14 drinks per week for women or more than 21 drinks per week for men.
TCH: thunderclap headache.
Precipitating factors
Precipitating conditions associated with RCVS.

Headaches
Headache was the presenting symptom in all patients. However, TCH was documented at disease onset only in 69 (67.6%), and it typically recurred only in 42 (60.9%) of these cases. Pain location was mainly bilateral (n = 63; 91.3%), and nausea/vomiting were the most frequently reported associated symptoms (n = 56; 81.2%). Severe headache of gradual onset was reported by 15 (14.7%) patients, while eight (7.8%) patients had throbbing headache. The remaining patients reported other varieties of pain, including persistent headaches of variable severity and acute headache episodes peaking in more than 1 minute. Most patients with episodic pain also had lingering headache of mild severity between their acute headaches.
Brain imaging
The most frequent abnormality detected at brain imaging was cortical subarachnoid hemorrhage (cSAH; n = 16 [15.7%]), followed by acute cerebral infarction (n = 12 [11.7%]) and intracerebral hemorrhage (ICH; n = 3 [2.9%]). Fourteen of these patients showed persistent neurological deficits.
Vascular imaging
The diagnosis of vasospasm was made by cerebral magnetic resonance angiography (MRA) in the majority of cases (n = 47 [46.1%]), followed by conventional digital subtraction angiography (n = 42 [41.2%]), computed tomographic angiography (CTA, n = 12 [11.8%]), and transcranial Doppler sonography (n = 1 [1.0%]). Overall, the first vascular imaging procedure was performed at a mean of 5.9 ± 7.4 days after symptom onset. In 36 (35.3%) cases, however, cerebral vasospasm was not detectable on the first investigation and it was visualized on a second angiogram (MRA in 28 cases, CTA in eight) performed at a mean of 15.4 ± 14.8 days following symptom occurrence.
Cerebrospinal fluid analysis
Lumbar puncture was performed in 45 (44.1%) patients. Nine had slightly elevated CSF WBC (mean, 7.8/mm3; range, 5–16) and six (5.9%) slightly elevated CSF protein levels (mean 93 mg/l, range 67–111).
Treatment
Eighty (78.4%) patients were treated with nimodipine, by intravenous infusion (1–2 mg/hours) followed by oral administration (n = 10) or by direct oral administration (n = 70; 30–60 mg every 4 hours) for 4 to 8 weeks; 10 (9.8%) patients received glucocorticoids, while in the remaining 12 (11.8%) cases no specific therapy was used because of the spontaneous improvement of symptoms.
Idiopathic versus secondary RCVS
Clinical features of the study group according to RCVS etiology.

PRES: posterior reversible encephalopathy syndrome; TCH: thunderclap headache.
RCVS with TCH versus RCVS without TCH
Apart from a higher prevalence of hypercholesterolemia in the subgroup of RCVS patients without typical TCH, we did not detect any difference in both predisposing conditions and clinical features between the two groups defined by headache characteristics (Tables 1 and 3).
Discussion
The main findings from the analysis of this large series of Italian patients with definite RCVS were a) confirmation that the disease targets middle-aged women in most of the cases; b) the evidence, consistent with the literature, that precipitating conditions or potential triggers with putative impact on cerebral arterial tone are a frequent finding in these patients; c) the relatively high rate of RCVS related to putative etiologic conditions, which occurred in approximately one out of five cases. These patients were, furthermore, younger than those with idiopathic RCVS, more frequently had a personal history of migraine, and more likely had atypical clinical manifestations, with TCH as presenting symptom in less than one-third of cases and a relatively high rate of neurological complications leading to incomplete recovery; d) the difficulty in making the correct diagnosis in a non-negligible proportion of cases, about one-third of the patients having a normal cerebral vasculature at initial angiogram.
In the context of the current literature
Summary of selected studies including large series of RCVS patients.
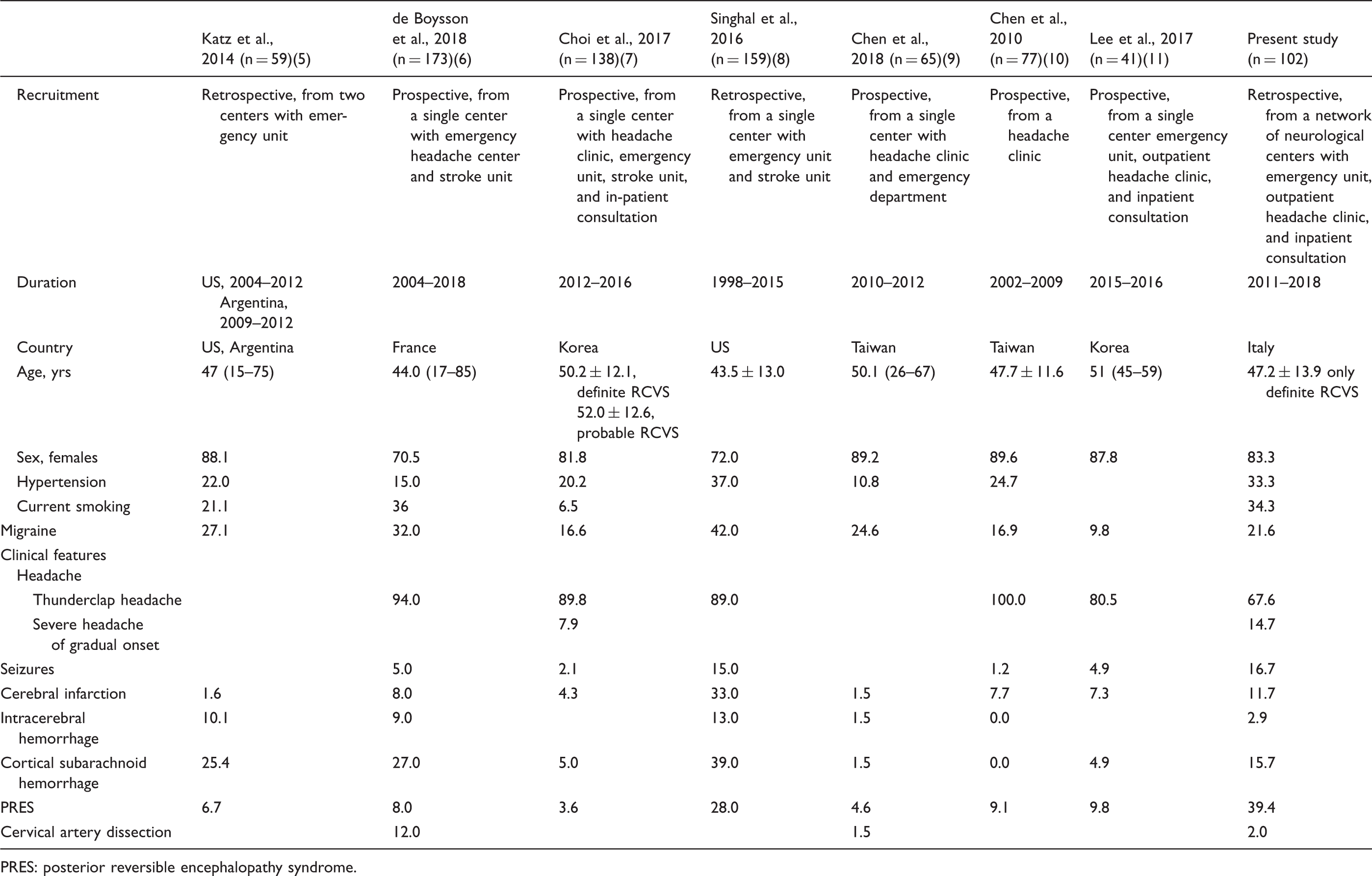
PRES: posterior reversible encephalopathy syndrome.
Finally, in agreement with findings from prior cohorts, the first angiogram was normal in more than one third of our cases when performed within the first week of symptom onset, and it became diagnostic at a mean of two weeks (15). These observations underline the importance of repeated vascular imaging investigations in the diagnostic workup of RCVS, even in those cases with persistent non-TCH.
Strengths and limitations
One of the strengths of the present study relies on the thoroughness of case ascertainment, which allowed unbiased diagnosis and comprehensive evaluation. In this regard, our decision to include only patients who met the criteria for definite RCVS was taken in order to reduce the risk of misdiagnosis as much as possible. Nevertheless, several limitations should also be considered. Although this is one of the largest series reported thus far, the number of patients included might have been too small and the analysis underpowered to identify subtle correlations with specific risk factors and comorbid conditions. Therefore, estimates, especially for subgroups that contain only a few patients, might be unstable and should, therefore, be interpreted with caution. In addition, the criteria we adopted for the definition of specific subgroups, such as those of idiopathic RCVS and secondary RCVS, is another issue. Our results were, actually, derived on the basis of a non-validated etiologic classification of the disease, which potentially limits their generalizability. However, in the absence of standardized classification criteria, any other way of subcategorizing the disease based on the presumed etiology would have been equally arbitrary. Obviously, because the study was designed as a multicenter registry for epidemiologic purposes, any exhaustive investigation of pathogenic determinants was beyond the scope of the present analysis. Finally, inaccurate capture of the incident cases cannot be excluded. This, in addition to the fact that the present cohort is not population-based, implicates that our study group could be similar to a convenience sample. However, this is an unavoidable feature of all hospital-based registries even when all consecutive cases diagnosed at the participating centers are included.
Conclusions
In conclusion, the present study showed that the clinical manifestations of RCVS are slightly different from and more heterogeneous than those observed in some previous cohorts and suggests, in particular, that such variability might be partly related to coexistent precipitating conditions with a putative etiologic role in disease occurrence. Whether this depends on different biologic processes underlying the disease is beyond the scope of our analysis and warrants further investigations. Our results also confirmed the difficulty in making a diagnosis in selected cases, especially when the angiogram performed within a week of symptom onset is normal, which implies that a high level of clinical suspicion is needed in these circumstances and that the opportunity for repeated vascular investigations about two weeks later should be considered, even in case of persistent non-TCH. Finally, neurological complications leading to persistent deficits are all but uncommon. Formal randomized trials on the management of RCVS and its impact on patient outcome or prognosis are, therefore, urgently needed.
Footnotes
Clinical implications
Reversible cerebral vasoconstriction syndrome (RCVS) targets middle-aged women in most of the cases, is frequently preceded by precipitating conditions with putative impact on cerebral arterial tone, and about one-third of the patients have a normal cerebral vasculature at initial angiogram.
Patients with RCVS related to putative etiologic conditions are more likely to have atypical manifestations with a relatively high rate of neurological complications. This suggests that the biologic process underlying the disease might partly vary according to the causative mechanisms.
The first angiogram, irrespective of type, is negative in more than one third of cases if it is performed within a week of symptom onset. The opportunity for performing a second angiogram at two weeks should be considered in the event of persistent, though atypical, headache.
Author contributions
Filomena Caria: Manuscript drafting/revising, study design, data analysis and interpretation, data acquisition. Alessandro Pezzini: Statistical analysis, manuscript drafting/revising, study design, data analysis and interpretation, data acquisition, statistical analysis, study supervision. All authors: Manuscript drafting/revising, data acquisition.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The sponsor had no role in the design and conduct of the study; the collection, management, analysis, and interpretation of the data; the preparation, review or approval of the manuscript; or the decision to submit the manuscript for publication. Alessandro Pezzini had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Italian Project on Stroke in Young Adults (IPSYS) is supported by a grant from the Associazione per la Lotta alla Trombosi e alle Malattie Cardiovascolari (ALT).