
Abstract
Objectives
To serially test the International Classification of Headache Disorders (ICHD) 3rd edition beta version criteria for 6.7.3.1 probable reversible cerebral vasoconstriction syndrome (probable RCVS) in patients with thunderclap headache.
Methods
We prospectively screened consecutive patients with thunderclap headache who visited the Samsung Medical Center between October 2015 and March 2017. Patients were included in the analysis if they a) visited our hospital within 1 month after onset, b) completed a diagnostic work-up, and c) had no secondary causes other than RCVS. The ICHD-3 beta 6.7.3.1 criteria were evaluated serially during the first visit (visit 1), 2 weeks after the first visit (visit 2), and 1–3 months after onset (visit 3).
Results
A total of 99 patients completed this study. Based on the first clinical and radiological evaluation, 63 (63.6%) were diagnosed with angiogram-proven RCVS, whilst 36 (36.4%) showed normal neuroimaging. The ICHD-3 beta 6.7.3.1 criteria were fulfilled in 76.2% of patients with angiogram-proven RCVS. In patients with normal angiograms, the ICHD diagnosis of probable RCVS changed over time: 25.0%, 47.2%, and 38.9% at visits 1, 2, and 3, respectively. The sensitivity and specificity of the criteria at visit 1 were 72.4% and 95.5%, respectively, for the prediction of a final diagnosis of overall (angiogram-proven + probable) RCVS.
Conclusions
The ICHD-3 beta criteria for probable RCVS are applicable for patients with thunderclap headaches at the acute stage, with the exception of criterion C3. Criteria C1 and C2 are less reliable when applied at the first visit. Repeated evaluation is necessary to enhance diagnostic sensitivity.
Keywords
Introduction
Thunderclap headache is a red-flag sign that suggests a life-threatening condition (1). When a patient presents with thunderclap headache, a number of secondary causes need to be excluded by appropriate investigations. However, aneurysmal subarachnoid hemorrhage can be documented only in 10–25% of patients with thunderclap headache, while other causes account for even smaller percentages of cases (2,3). The remaining cases had been classified as “benign thunderclap headaches” before reversible cerebral vasoconstriction syndrome (RCVS) was widely recognized (1,4,5).
Currently, it is believed that RCVS accounts for most benign thunderclap headaches (4). However, angiogram results can be normal or ambiguous depending on the timing, modality, and resolution of the angiographic scan (6,7). For those with normal angiogram results, RCVS can be diagnosed based on the clinical manifestation (“probable RCVS”). The International Classification of Headache Disorders 3rd edition beta version (ICHD-3 beta) offers diagnostic criteria for probable RCVS in section 6.7.3.1 (8). However, those criteria have not yet been validated. Its validation is important, because these criteria are the only way to make a specific diagnosis when patients show normal neuroimaging.
In this study, we tested the ICHD-3 beta criteria for probable RCVS in patients with thunderclap headache. We aimed to a) validate the ICHD-3 beta criteria for probable RCVS in patients with angiography-proven RCVS, b) test the applicability of the criteria during acute phases in patients with thunderclap headache, and c) serially test the stability of the diagnosis at different time points.
Methods
Patients
We screened new patients with thunderclap headache who visited the outpatient headache clinic or emergency room of the Samsung Medical Center, Seoul, Korea from October 2015 to March 2017. We included patients who a) presented to us within 1 month after onset, b) completed a diagnostic work-up, and c) did not have a secondary cause other than RCVS. Our protocol for the evaluation of thunderclap headache was described previously (9). The institutional review board at Samsung Medical Center approved this study. All participants provided written informed consent.
Evaluation
During the initial visit (visit 1), patients were screened and interviewed by investigators. Patients then completed a structured questionnaire designed for this study. This questionnaire included questions regarding time to peak intensity, severity and duration of the thunderclap headache, recurrence, and any event triggered by the typical precipitants. Brain magnetic resonance imaging (MRI) and magnetic resonance angiogram (MRA) were performed after visit 1.
Patients were evaluated again within 2 weeks after visit 1 (visit 2). During visit 2, patients were interviewed by investigators and completed the same questionnaire as during visit 1. Any recurrence of thunderclap headache was recorded, while a mild residual headache was not regarded as a recurrence.
The final evaluation (visit 3) was performed 1–3 months after the first visit. At this time, the evaluation included both the interview and the same questionnaire. When interviewing patients at this time point, we focused on the occurrence of any significant headache more than 1 month after onset. Follow-up neuroimaging was performed 3–6 months after onset for patients with angiogram results suggestive of RCVS, i.e. multifocal stenosis of >50% in ≥2 intracranial arteries (9).
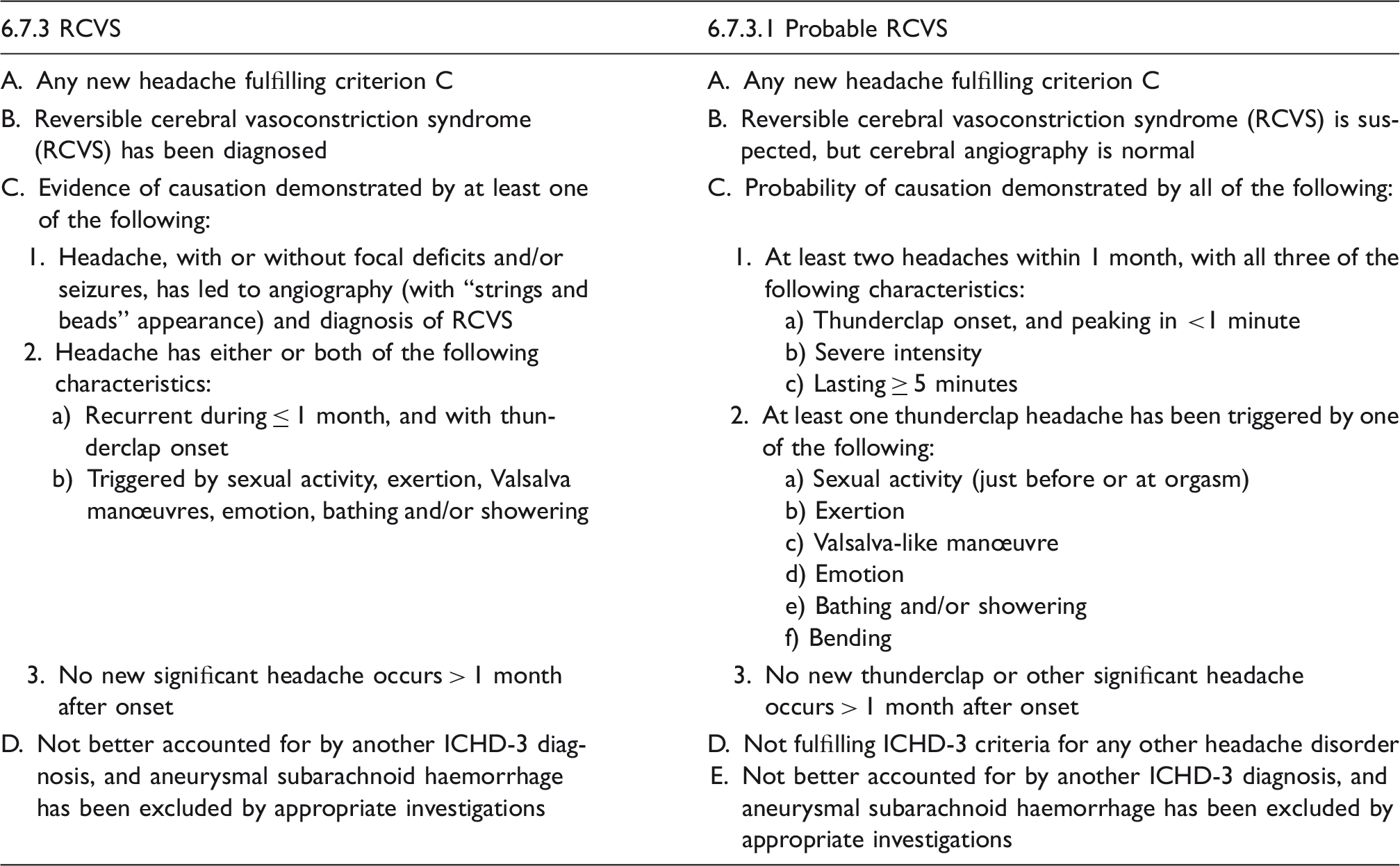
Comparison of the ICHD-3 beta criteria for 6.7.3 RCVS and 6.7.3.1 probable RCVS.
Statistical analysis
Statistical analyses were performed using PASW Statistics for Windows, Version 18.0 (SPSS Inc., Chicago, IL, USA). Data were presented as number (%) or median (interquartile range). The chi-square and Fisher’s exact tests were used to compare each criterion between patients with angiogram-proven RCVS and those with a normal angiogram. For patients who fulfilled the ICHD-3 beta criteria for probable RCVS at each visit, their final diagnoses were evaluated. The diagnostic power of the 6.7.3.1 criteria and neuroimaging for the diagnosis of all RCVS (angiogram-proven + probable) were determined by analyzing the receiver operating characteristic (ROC) curve. Two-tailed p values < 0.05 were considered significant.
Results
Patients
During the study period, we screened 127 patients with thunderclap headache. Among them, 106 patients met the inclusion criteria. Ninety nine patients completed the serial evaluation and were included in the analysis. The final diagnoses of the included patients were RCVS (n = 63), probable RCVS (n = 14), and primary thunderclap headache (n = 22). The flow diagram is presented in Figure 1.
Flow diagram.
Serial evaluation of the criteria for 6.7.3.1 probable RCVS
Serial assessment of the ICHD-3 beta criteria 6.7.3.1 probable RCVS and neuroimaging findings.

Only 13 (36.1%) patients with initial normal MRA underwent follow-up MRA. Data are presented as number (percentage) or median (interquartile range).
Serial validation of ICHD-3 beta criteria for 6.7.3.1 probable RCVS
At the first evaluation, 76.2% of patients with angiogram-proven RCVS met all criteria for probable RCVS (Figure 2(a)). The proportion did not greatly vary at subsequent visits, showing 79.4% and 76.2% at visits 2 and 3, respectively.
Serial testing of the ICHD-3 beta criteria 6.7.3.1 probable RCVS in patients with (a) angiogram-proven RCVS (n = 63) and (b) normal neuroimaging (n = 36). Black bar indicates proportions of patients who met the 6.7.3.1 criteria at a given time point.
Among 36 patients with normal neuroimaging, only nine (25.0%) were diagnosed with probable RCVS at the first visit (Figure 2(b)). Diagnostic rates of probable RCVS increased at visit 2 (n = 17, 47.2%), then decreased at visit 3 (n = 14, 38.9%). The diagnosis of 4.4 primary thunderclap headache was made in 22 (61.1%) patients who did not met the criteria for 6.7.3.1 probable RCVS at visit 3. Primary exercise headache, primary cough headache, and primary headache associated with sexual activity were not present in our study subjects.
Diagnostic implications of ICHD-3 beta criteria for 6.7.3.1 probable RCVS
Figure 3 shows the distribution of final diagnosis according to the ICHD-3 beta criteria for probable RCVS at different time points. When patients met these criteria at the first visit, the final diagnosis was RCVS in 98.2% of cases (Figure 3(a); 84.2% with angiogram-proven RCVS and 14.0% with probable RCVS). However, patients who did not meet the criteria still had a 50% possibility of having overall RCVS. At visit 2, 17 patients met the criteria (Figure 3(b)). Among these, three (4.5%) had persistent or recurrent headache at over 1 month after onset: Recurrent thunderclap headache on day 42 after onset (n = 1) and persistent headache of greater than moderate intensity for 45 and 120 days, respectively (n = 2). Their final diagnosis was changed to primary thunderclap headache at visit 3. At visit 3, 14 (22.6%) of 62 patients who met the 6.7.3.1 criteria were finally diagnosed with probable RCVS.
Final diagnosis according to the ICHD-3 beta criteria 6.7.3.1 probable RCVS at (a) visit 1, (b) visit 2, and (c) visit 3.
Comparison with neuroimaging findings
In patients with angiogram-proven RCVS, initial MR findings were highly suggestive of RCVS in only 46 (73.0%) patients (Table 2). In the remaining 17 patients, initial angiogram findings were considered equivocal or normal. Follow-up imaging revealed dynamic changes that helped diagnose RCVS. In angiogram-negative patients, three (8.3%) showed multifocal intracranial stenosis in their initial neuroimaging, but their follow-up imaging at 3 months showed no change. All three patients were elderly Korean women (age: 70, 72, and 73 years). We performed follow-up MRAs for two patients at 6 months and 1 year, respectively, but found no improvement. They were finally determined to have intracranial atherosclerosis. Among those three patients, one patient had symptoms compatible with probable RCVS. The other two patients were diagnosed with primary thunderclap headache.
Diagnostic power of initial neuroimaging and the ICHD-3 beta criteria for 6.7.3.1 probable RCVS for the prediction of the final diagnosis of overall (angiogram-proven + probable) RCVS.

Abbreviations: AUC: area under the curve; CI: confidence interval.
Discussion
In this prospective, single-center, serial validation study, we found that a) approximately 80% of patients with angiogram-proven RCVS met the ICHD-3 beta criteria for probable RCVS, b) the ICHD-3 beta 6.7.3.1 criteria were applicable for patients with thunderclap headache in the early phase of the disease, except for criterion C3, c) the diagnosis of probable RCVS using the criteria changed over time, and d) when the criteria were fulfilled, patients were highly likely to have RCVS, but there was also a substantial probability of RCVS when patients did not meet the criteria.
Applicability of the criteria
In this study, we applied the ICHD-3 beta 6.7.3.1 criteria to patients with thunderclap headache. The criteria helped investigators effectively interview patients, and patients clearly understood the questions based on the criteria. However, criterion C3, which denotes the 1-month observation period, could not be applied at the early phase of the disease. Also, criteria C1 and C2 were less reliable when patients visited the hospital immediately after the first thunderclap headache.
Validation of the ICHD-3 beta criteria for 6.7.3.1 probable RCVS in patients with angiogram-proven RCVS
This study is the first to validate the ICHD-3 beta criteria for probable RCVS. Because the ICHD-3 beta criteria 6.7.3.1 are currently the only diagnostic method for the diagnosis of probable RCVS, the diagnostic accuracy of the criteria could not be validated in comparison with a “gold standard” diagnostic method. Instead, we tested the criteria in patients with angiogram-proven RCVS. Over 75% of patients with angiogram-proven RCVS met the 6.7.3.1 criteria at all the three visits. In other hand, as shown in our previous study (10), the ICHD-3 beta criteria for 6.7.3 headache attributed to RCVS was met in 100% of patients with angiogram-proven RCVS. When patients did not have any recurrent or triggered thunderclap headaches, they still met the ICHD-3 beta 6.7.3 because neuroimaging (criterion C1) or clinical course (criterion C3) can be substituted for the diagnosis.
The criteria showed a relatively low sensitivity, but a high specificity for RCVS at the first evaluation, and repeated assessment increased the sensitivity. Considering that the sensitivity of the initial angiogram was also not optimal (61.8% in this study), serial evaluation of the criteria might be helpful for early suspicion of RCVS. When the criteria were met at the first evaluation, it was highly specific for the RCVS in our study setting.
Instability of the diagnosis
The diagnosis changed over time in patients with normal neuroimaging. In particular, whether patients met the C1 and C2 criteria changed over time; higher recurrence and triggered thunderclap headaches were noted later. Therefore, the visit 2 evaluation led to an increased diagnosis of probable RCVS. The criterion C3 determined the final diagnosis at visit 3. These findings emphasize the need of repeated application of the ICHD-3 beta criteria.
At the first visit, less than 50% of patients with a final diagnosis of probable RCVS met the section 6.7.3.1 criteria. At visit 2, all patients met all criteria except criterion C3. Although three patients were reclassified as having primary thunderclap headache at visit 3, two showed a monophasic course within 2 months after onset. Taken together, repeated evaluation can help increase the diagnostic rate of probable RCVS. Our study suggests that criterion C3 can be deferred during the acute early evaluation to enhance a rapid identification of the disease.
Strengths and limitations
The prospective setting and serial assessment of clinical and radiological findings are the primary strengths of this study. However, this study is not without limitations. First, the 6.7.3.1 criteria were not tested in patients with secondary causes other than RCVS. Therefore, our study results should not be generalized when other secondary causes were not excluded with appropriate neuroimaging. Second, not all patients with normal angiograms underwent repeated angiograms, as the National Health Insurance System in Korea does not reimburse the cost of neuroimaging in patients without a neurological deficit. This can lead to underdiagnosis of RCVS (6,11). However, there is no prerequisites in the number of neuroimaging to determine or exclude the diagnosis of RCVS or probable RCVS in the current ICHD-3 beta (8). Cost-effectiveness of repeated neuroimaging is also unknown. These concerns should be further discussed to draw a consensus recommendation. Third, we used 3D time-of-flight (TOF) MRA for the diagnosis of RCVS. Different modalities can yield different results in the diagnosis of RCVS (12). However, TOF MRA has many benefits. First, intracranial arterial dissection can be differentiated by analyzing TOF MRA source images (13). Second, TOF MRA is a non-invasive and safe method (6), while DSA carries a substantial risk of deterioration in patients with RCVS (11). Although both MRA and CTA have limitations for the detection of distal vasoconstrictions (12), limitations of TOF MRA, flow-related artifact and in-plane saturation artifact can be overcome by follow-up imaging, which helped to differentiate true reversible vasoconstrictions versus artifact in distal intracranial arteries (14).
Clinical implications
The ICHD-3 beta criteria for 6.7.3.1 probable RCVS were applicable for patients with thunderclap headache at the early phase of the disease, except for criterion C3. Over 75% of patients with angiogram-proven RCVS met the ICHD-3 beta criteria for probable RCVS. The diagnosis of probable RCVS based on the 6.7.3.1 criteria changed over time. In particular, repeated evaluation led to increased recognition of recurrence and triggered headaches (criteria C1 and C2). When the section 6.7.3.1 criteria were fulfilled, patients were highly likely to have RCVS, while there was also a substantial probability of RCVS when patients did not meet the criteria.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by Yuhan company in data management.