
Abstract
Background/Hypothesis:
Creativity is a cognitive process that affects the performance of many daily life activities. This process, in turn, is influenced not only by various environmental factors but also by numerous individual aspects. Chronic pain is one of the factors that has proven to negatively affect creativity. Our hypothesis is that people with migraine in the interictal phase also have lower levels of creativity than the control group.
Methods:
We collected data from participants with migraine (n = 31) in the interictal phase and from a non-migraine control group (n = 30). We used the Alternative Uses Task (AUT) test and the Creative Intelligence Test (CREA) to evaluate creativity.
Results:
Our results revealed lower creativity in participants with migraine. This was confirmed by both the AUT (fluency: controls 7.4 (4.35) vs. participants with migraine 4.4 (2.9); p < 0.001; originality: controls 2.353 (0.457) vs. participants with migraine 2.07 (0.278); p < 0.001; flexibility: controls 3.4 (1.55) vs. participants with migraine 2.0 (1.0); p < 0.001) and CREA (controls 14.0 (9.875) vs. participants with migraine 9.5 (5.0); p = 0.004) tests.
Interpretation:
The present pilot study provides evidence that migraine, even in the interictal period, reduces creative ideation and this may impact the quality of life of these individuals.
Introduction
Migraine is a chronic condition with a prevalence that fluctuates in Western countries between 15–20% in women and 5–8% in men, 1 and more than 80% of people with migraine have some type of migraine-related disability. 2 According to the 2019 Global Burden of Disease Study, migraine is the second leading cause of years lived with disability in the specific disorder classification. Several studies have demonstrated the impairment of various cognitive processes in people with migraine during pain crises. 3 Although the impact of migraine on attention, memory, or executive function in the interictal periods was initially more controversial, the latest published studies and meta-analyses show that these processes are indeed affected in people with migraine even in the interictal period. 4
There is an ever-increasing interest in the study of human beings’ ability for creativity. More knowledge about creativity, including how, when and where it is generated, as well as what factors affect it, has significant implications for a multitude of areas such as marketing, education, and the arts as well as various scientific disciplines. Creativity permeates our daily lives because we draw on our knowledge base to find novel solutions to problems that arise in our daily lives. 5
Few definitions of creativity have been proposed. For example, Chrysikou defined creativity as “the product of oppositional but synergistic neurocognitive processes capturing the generation of novel ideas that deviate from regularly produced responses (a process commonly described as ‘divergent thinking’) and the evaluation of the appropriateness of these ideas in context (sometimes referred to as ‘convergent thinking’)”. 6 Meanwhile, Plucker proposed the following definition: “creativity is the interaction among aptitude, process, and environment by which an individual or group produces a perceptible product that is both novel and useful as defined within a social context”. 5 Whatever the definition, it seems clear that creativity fosters social integration and is important for problem solving. Thus, it is important to quantify the effect of chronic medical conditions like migraine on creativity.
Studies regarding the effect of headache on creativity are limited. In Gubler et al., the evaluation of chronic pain patients, mostly with conditions that generate musculoskeletal pain as well as a small group of headache patients, suggests that this population generates fewer creative ideas than the control group. 7
This pilot study aims to test whether there are differences in creativity between participants with migraine in their interictal period and a control group of healthy subjects.
Methodology
This study has the characteristics of a case–control study.
Procedure
The data collection sessions were carried out in person and took place at the Hospital del Henares. The data compilation phase took place during April and May 2023. The study date was set after informing participants of the study characteristics and obtaining written informed consent. On the day of the session, all the required demographic and clinical data were collected and the creativity tests were carried out. We collected the data, the Visual Analog Scale (VAS) for pain, the Headache/Migraine Day Calendar (HDC), Hospital Anxiety and Depression Scale (HADS), the NEO Five-Factor Inventory (NEO-FFI) personality test, and the AUT and CREA creativity tests. A typical session lasted approximately 45 minutes.
Participants
Two groups of participants were selected for this study: a group of participants with migraine (n = 31; 27 female; age = 45.48 ± 11.03), and a control group of healthy subjects (n = 30; 22 female; age = 43.33 ± 12.44). We followed the ICHD-III criteria for migraine with or without aura, chronic migraine, or medication-overuse headache. There were no other coexisting headaches in any participant. Due to the exploratory nature of this pilot study aura was not considered for analysis due to our small sample size. Participants with migraine included in this study had a face-to-face or telephone appointment at the headache division of the Neurology Department at the Hospital del Henares in Madrid. The control group was composed of individuals from the general population, participants’ companions or employees of the Hospital del Henares in Coslada-Madrid who met the inclusion criteria. Inclusion Criteria: (1) Age between 18 and 80 years; (2) Both sexes; (3) Participants with migraine must meet criteria for episodic or chronic migraine with or without medication-overuse headache 8 ; (4) Acceptance of informed consent. Exclusion Criteria: (1) age <18 or >80 years; (2) presence of other pathologies that generate chronic pain; (3) migraine episode at the time of testing or pain levels above four (measured using visual analogue scale); (4) serious sleep disturbances; (5) recreational drug consumption (volunteers who occasionally consume moderate amounts of alcohol and tobacco were admitted. Moderate drinking definition: up to 14 grams per day for women and up to 28 grams per day for men. Moderate tobacco definition: up to 10 cigarettes, or equivalents, per day); (6) Participants with migraine under prescribed treatment of topiramate or benzodiazepines; (7) non-acceptance of informed consent. Inclusion criteria no 3 and exclusion criteria no 6 were specific for the group of participants with migraine. Whereas in the control group, no medication was permitted for any indication besides contraceptive treatment.
The study protocol is in accordance with the Declaration of Helsinki and was approved by the IRB of the “Universidad a Distancia de Madrid” (PSIA20230329-3). Participants signed a written informed consent.
Data collected and tests
The demographic data collected were age, sex, occupation, and educational level. On the other hand, the clinical data obtained were clinical diagnosis and type of headache, current treatment including non-pain related treatments, number of days with migraine (HDC), and other pathologies. The participants with migraine with migraine were evaluated in their interictal period. At test time, participants with migraine could not have any prodromic symptoms and had to be pain free for the previous 24 hours. As an exception, chronic participants with migraine with almost daily headaches could not have any prodromic symptoms, could not have required rescue treatment in the last 24 hours, and could not present pain levels over 3 on the VAS scale. Participants with migraine were asked to inform of a migraine attack occurring in the 24-hour period following evaluation.
The tests used were:
Visual Analog Scale (VAS). To assess pain, we used VAS 9 for the last week and at the time of testing. The VAS measures pain intensity and consists of a 10 cm line, with two endpoints representing 0 (“no pain”) and 10 (“pain as bad as it could possibly be”) where participants with migraine graph the average pain level.
Hospital Anxiety and Depression Scale (HADS). This is a short clinical instrument (14 items) designed to evaluate anxiety and depressive mood levels that has been validated in Spanish. 10 Here, participants must rate statements on a Likert scale indicating which option best defines their situation over the last week. This scale was corrected as indicated by the authors. 11,12
NEO Five-Factor Inventory. Personality was assessed using the self-reported NEO-FFI questionnaire (reduced to five factors), which consists of 60 items and evaluates the big five personality traits: neuroticism, extraversion, openness, agreeableness, and conscientiousness. Herein, participants used numbers indicated at the beginning of the test to rate their level of agreement with the statements, referring to their habitual situation. This test was corrected following indications in the manual. 13
Alternatives Uses Task (AUT). The evaluation of “divergent thinking” is still considered a benchmark in assessing differences between individuals. 14 The subject was shown an object and was instructed to indicate all the possible uses he/she could think of. Subjects were given 2 minutes to write as many uses as they could for each of five objects shown successively (e.g., chair, brick, paper clip, umbrella, and spoon), keeping in mind that we were conducting a creativity study, 15 and would therefore exclude any response indicating the common use of the object or multiple responses that refer to the same overall use of a given object. Corrections followed the indications of previous studies. 14,16 Scores were obtained for the following measures:
Fluency: ability to produce ideas. The examiner calculated the scores by counting the number of different uses given to each object, excluding its most common use.
Originality: Defined as the subject’s ability to produce new and unique ideas. All the participants’ answers were compiled in a single list, eliminating repeats. Three judges independently rated the responses contained in this list for originality on a five-point Likert scale ranging from 1 (not at all original) to 5 (very original) based on the instructions for judging creativity from previous studies. 16 After scoring response originality, an average score was calculated for each object as well as an average score for all five objects. Subsequently, the judges’ agreement was measured quantitatively at 0.651, which is considered a good level. 17
Flexibility: Ability to produce different idea categories. Herein, the complete list of responses for each object was entered into ChatGPT-4, asking it to produce a list of 10 categories. Subsequently, the judges reviewed the different categories and adjusted for possible errors. After coming to a consensus on what categories to use, the judges evaluated the number of categories that each participant’s answers could be classified under for each object.
Creative Intelligence Test (CREA). Creativity can also be measured through the subject’s ability to generate questions. As opposed to the AUT, the CREA test measures the ability to generate problems to a solution by posing questions about a given image. Participants were shown two images, successively, and were given 4 minutes per picture to formulate as many questions as they could about each of the images. The CREA test was corrected following the instruction manual. 18
Statistical analysis
Demographic data, pain score (VAS), depressive and anxiety levels (HADS), the NEO-FFI personality test, the Headache/Migraine Day Calendar (HDC), AUT and CREA are summarized in Table 1. Parametric data are shown by mean and standard deviation (SD) and the parametric univariate test (t test) was used to compare data between the different groups (control vs. migraine and episodic vs. chronic) and non-parametric data are showed by median and interquartile range (IQR) and the non-parametric univariate test (Mann–Whitney U test) were used to compare groups. We used the Chi-squared test to compare the proportion of women to men between the different groups. The Shapiro–Wilk test evaluated the variables normality. Finally, we performed a factor analysis to group the creativity variables (CREA test and the three measures of the AUT test) into a single factor. We used a principal components analysis (PCA) to reduce the number of creativity variables. We used the Kaiser–Meyer–Olkin (KMO) test, to test the suitability of the sample for PCA. We analyzed the differences in this factor between groups (controls, participants with episodic migraine, and participants with chronic migraine) using non-parametric Kruskal Wallis H test. In case of significant effects, the Dunn post hoc test was performed using a Bonferroni–Holm correction. To confirm that potential differences in creativity are attributable to migraine, a covariance analysis (ANCOVA) will be conducted, adjusting the analysis for covariates that demonstrate differences between both groups. All analyses were conducted using the statistical software JASP 0.16.1, and significance was set at p < 0.05.
Demographic characteristics and study variables (clinical, creativity and personality) of control subjects and participants with migraine and statistical results of the comparison between the groups.a

N: number of subjects; SD: standard deviation; IQR: interquartile range; VAS: Visual Analog Scale for pain; HADS-D/A: Hospital Anxiety and Depressive Scale–Depressive/Anxiety; NEO-FFI_A/N/C/E/R: NEO Five-Factor_Agreeableness/Neuroticism/Conscientiousness/Extraversion/Openness_to_Experience (personality test); HDC: Headache/Migraine Day Calendar; AUT-Fluid/Orig/Flex: Alternative Uses Task Fluency/Originality/Flexibility (creativity test); CREA: creativity test.
a The variables shown mean + SD, median (IQR) or N. Univariate statistical test used: chi-square test, t test or Mann–Whitney U test. Significant p values are in bold.
To calculate the sample size, we used the effect sizes of two previous studies which examined both the relationship between chronic pain and creativity 7 and the differences in cognitive tasks between healthy individuals and patients with chronic pain. 19 Both studies found moderate to large effect sizes (η 2 p = 0.091 and f = 0.4 respectively). We used G*Power 20 to calculate the sample with a medium-large effect size (ds = 0.75), and a significance of 0.05. Obtaining a statistical power of 0.80 required a total sample of 58 participants for the two groups.
Results
As shown in Table 1, there were no significant differences in age (p = 0.511) or sex (p = 0.176) distribution between groups. participants with migraine reported significantly more pain, depressive mood, and anxiety than healthy controls. Regarding pain, participants with migraine had higher average pain intensity scores in the last week according to the Visual Analogue Scale (W = 121.5, p ≤ 0.001) and more days with pain in the last month evaluated by the Headache/Migraine Day Calendar (W = 29, p < 0.001). Furthermore, participants with migraine obtained significantly higher scores in anxiety (W = 273.5, p = 0.006) and depressive levels (W = 224.5, p < 0.001) according to the HADS. No significant differences were found in the NEO-FFI personality test (O: p = 0.994; N: p = 0.241; A: p = 0.347; E: p = 0.988; C: p = 0.977).
Regarding creativity, the migraine group showed lower scores than healthy controls in the CREA test (W = 665.5, p = 0.004) and in all AUT measures: fluency (W = 723.5, p < 0.001), originality (W = 730.5, p < 0.001) and flexibility (W = 823.5, p < 0.001).
Participants with migraine are broken down into chronic and episodic migraine subgroups in Table 2. In this case, no significant differences were observed in age (p = 0.335), sex (p = 0.849), pain intensity (p = 0.061), anxiety (p = 0.540), or depressive levels scores (p = 1), or in the NEO-FFI personality traits, except agreeableness (O: p = 0.844; N: p = 0.346; E: p = 0.554; C: p = 0.930). Participants with chronic migraine showed lower agreeableness scores than participants with episodic migraine (W = 151.5, p = 0.023), as well as a greater number of days with pain in the last month according to the Headache/Migraine Day Calendar (W = 2,500, p < 0.001). Regarding creativity, participants with chronic migraine obtained significantly lower scores in all dimensions of the AUT, fluency (W = 152.5, p = 0.021), originality (W = 147.5, p = 0.037), and flexibility (W = 155.5, p = 0.014), but there were no significant differences in the results of the CREA test (p = 0.206).
Demographic characteristics and study variables (clinical, creativity and personality) of participants with chronic and episodic migraine and statistical results of the comparison between the groups.a
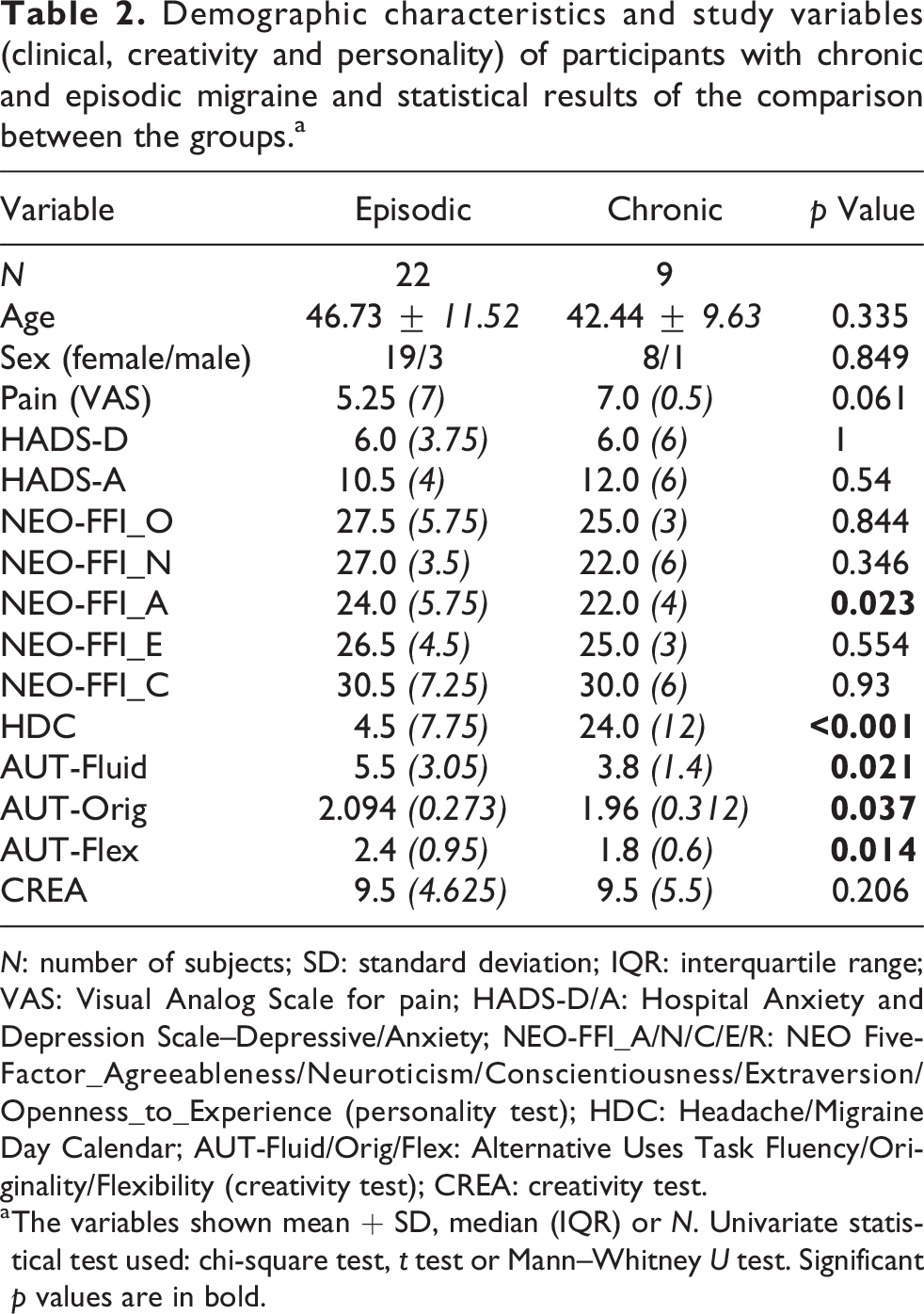
N: number of subjects; SD: standard deviation; IQR: interquartile range; VAS: Visual Analog Scale for pain; HADS-D/A: Hospital Anxiety and Depression Scale–Depressive/Anxiety; NEO-FFI_A/N/C/E/R: NEO Five-Factor_Agreeableness/Neuroticism/Conscientiousness/Extraversion/Openness_to_Experience (personality test); HDC: Headache/Migraine Day Calendar; AUT-Fluid/Orig/Flex: Alternative Uses Task Fluency/Originality/Flexibility (creativity test); CREA: creativity test.
a The variables shown mean + SD, median (IQR) or N. Univariate statistical test used: chi-square test, t test or Mann–Whitney U test. Significant p values are in bold.
We used a PCA to reduce the number of creativity variables. The results of the KMO measure of sampling adequacy, yielding a value of 0.784, alongside Bartlett’s Test of Sphericity, revealing a significant chi-square of 151.469 (p < 0.001), collectively provide strong justification for conducting a PCA. Dimensionality reduction of creativity revealed the existence of a single creativity factor with all the variables that evaluate this construct (CREA, AUT-Fluid, AUT-Orig, and AUT-Flex), which explains 74.6% of the variance. The Kruskal Wallis test showed the existence of significant differences between the three groups (H = 23.928, p < 0.001): controls (0.591 ± 1.005), participants with episodic migraine (0.391 ± 0.542), and participants with chronic migraine (−1.014 ± 0.421). The Dunn post hoc analysis revealed that there are differences between the control group and both participant with migraine groups: episodic (p = 0.002) and chronic (p < 0.001) but there are no significant differences between the two participant with migraine groups (p = 0.065) (Figure 1).

Differences in the total creativity factor between groups. The raincloud plot shows the score of each subject (points) in the “total creativity” factor, as well as the mean and distributions of the data for each group. The plot suggests that subjects in the chronic (purple) and episodic (orange) migraine groups score significantly lower on creativity than healthy controls (green). It is observed that the distribution of the data differs between the groups, so it is more appropriate to perform a non-parametric analysis. The significant p value of the Kruskall–Wallis test supports the differences in creativity between the groups (***p ≤ 0.001). The chronic (purple) migraine group showed a tendency to have lower creativity than episodic (orange) group (#p = 0.065).
Anxiety and depressive levels (measured by the HADS) were included as covariates in ANCOVA analysis. The group variable (controls/participant with migraine) emerged as significantly different for CREA (p = 0.009) and all measures of the AUT (p < 0.001), while the covariates of anxiety and depressive levels did not significantly affect these results (p > 0.05). This outcome suggests that the observed effect on creativity is primarily attributable to migraine condition rather than anxiety or depressive mood.
Discussion
This pilot study demonstrated that participant with migraine, in their interictal period, generated fewer creative ideas than healthy controls. Our findings are consistent with previous studies that demonstrated the detrimental effects of migraine on the performance of cognitive abilities (not formally individually tested here). Many different cognitive functions facilitate creativity. 21,22 Moreover, cognitive flexibility allows people to avoid habitual thought patterns 23 and inhibitory control may allow people to distance themselves from obvious, non-creative ideas. 24
Previous studies reported that the greater the patients’ reported pain, the less creative were their generated ideas. 7 Interestingly, we confirm less creativity in absence of actual pain (the interictal period).
As expected, levels of depressive and anxiety levels were higher in the participant with migraine than in controls. We cannot completely discard the role of psychological and psychiatric comorbidities on creativity; however, we did not observe any correlation between the levels of creativity (measured by CREA or AUT) and anxiety or depressive mood (measured by HADS).
To rule out the presence of prodromal symptoms, participants with migraine were asked if they had any of the following symptoms: fatigue, neck stiffness, mood change, concentration difficulties, nausea, photophobia, phonophobia, yawning, depressive symptoms, irritability, food craving. 25
This must be considered a preliminary pilot study. We did not evaluate confounding factors such as fatigue, decreased concentration, cognitive functions, sleep patterns, etc. However, we did ask participants if they were experiencing usual levels of fatigue and concentration impairment on the test day.
Some of the participants with chronic migraine included in this study reported daily pain. Although this study measures migraine’s impact on creativity in the interictal phase, we decided not to exclude these participants from the study as long as they were not in any migraine attack phase, reported pain levels below 4 on the VAS scale and complied with all of the other inclusion criteria.
Moreover higher levels of comorbid pathologies associated with migraine, 26,27 as well as other potential confounding variables, may affect creative ideation in the participant with migraine group. In addition, medications could have influenced our results. We excluded any participant under treatment with topiramate 28 and benzodiazepines 29 because of their known cognitive side effects (exclusion criteria). On the other hand, we included the participants with migraine under preventive treatment with botulinum toxin 30 or anti-CGRP monoclonal antibodies 31 because these treatments have no demonstrated effects on cognition. As other drug concerns, we included only one participant with migraine under low-dose amitriptyline (10 mg per day) as this was a pilot study. All these confounding factors will be systematically investigated in a larger population.
The CREA and the AUT are commonly employed tools to assess creativity; however, both present significant limitations that must be considered. In both tests, the evaluation of specific responses may be influenced by factors such as task familiarity and evaluator expectations, limiting its validity. Additionally, these tests do not assess the implementation of creative ideas in practice or evaluate their feasibility and effectiveness in real-life situations. However, good predictive validity of the AUT and other creativity test on the Design Product Ideation task has been demonstrated. 32
Regarding the limitations of CREA, it focuses on verbal creativity and may not fully encompass the diversity of creative skills. Additionally, it may be culturally biased. However, CREA shows strong alternate form reliability and moderate test-retest reliability, along with convergent validity with other creativity measures and discriminant validity with personality traits and academic performance. 33
On the other hand, in the case of the AUT, scoring tends to be biased toward the quantity of responses rather than their quality, and subjective evaluation may introduce inconsistencies and lack of objectivity in the results. However, the consensual assessment technique in AUT, where multiple judges rate responses independently, has proven effective across diverse contexts and samples, suggesting sufficient validity of subjective scores. Silvia et al. 14 also reported high agreement among evaluators, with participants explaining 50–60% and evaluators explaining 4–12% of the variance.
Regarding AUT’s measure of flexibility as a dimension of divergent thinking, this test holds significant theoretical importance, although it is only measured in a minority of published works on creativity. The significance of flexibility lies in its ability to differentiate the creative quality of participants’ responses beyond originality. 34 Concerns have been raised regarding the validity of flexibility measures in the AUT. Critics argue that flexible responses might not necessarily reflect real creativity, as they could include diverse yet irrelevant or unhelpful ideas. Additionally, the interpretation of flexibility can be subjective and influenced by evaluator bias. However, proponents of the AUT maintain that while flexibility alone does not guarantee creativity, it remains an important and measurable component of it. They highlight the AUT’s demonstrated predictive validity in various contexts, such as identifying creative individuals in artistic and scientific fields. 32 Furthermore, flexibility has been shown to correlate with other creativity aspects like originality and fluency, indicating its validity as a measure of creative capacity. 35 Additionally, the strong prediction of flexibility by fluency and originality suggests convergent validity among these measures, accounting for 61% of the variance. Conversely, the lack of association between creative flexibility and working memory/processing speed after adjusting for fluency/originality underscores its discriminant validity relative to these cognitive processes. 36
Beyond potential confounding factors, adding creativity to the list of cognitive processes affected by migraine supports the notion that this condition has a major impact on person with migraine’ quality of life. Less creativity decreases the chances of success when facing new situations, solving problems, or making novel proposals. 37 –42 Assessing creativity through tests offers valuable insights into the impact of migraine headaches on people with migraine’ creative capacity and cognitive processes supporting creativity. These tests examine both the quality and quantity of artistic or creative output. Additionally, these tools can be used to evaluate the effectiveness of therapeutic interventions aimed at improving the quality of life of people with migraine by measuring changes in creativity before and after treatment. Likewise, these tools can be used for devising coping strategies to enhance the quality of life of the people with migraine, such as implementing creative activities or exercises that can serve as outlets for expression and stress reduction.
Since migraine mainly affects women from the second to the fifth decade of life, a stage when work productivity is at its peak, 26 this condition has a major impact on optimal work performance. If we add this to the cognitive alterations in migraine described in previous publications, 4,43 –48 it further justifies these people with migraine’ feelings. We must also keep in mind creativity’s impact on coping with pain 42 and the protective and healing effect of creative activities that favor psychological well-being. 49
As this study has been designed as an exploratory pilot study, it has limited generalizability. First, recruitment was performed in a specialized migraine clinic, so treatment and diagnosis may be different from “real world” people with migraine. Moreover, the migraine group included the following variants: participants with low-frequency migraine, high-frequency migraine, chronic migraine, and migraine with and without aura. These clinical situations may have a different impact on creativity and only subsequent studies with larger samples can allow a realistic sub-analysis to test the influence of different types of migraine headaches on creativity.
To summarize, the present study provides evidence that migraine, even in the interictal period, reduces creative ideation and this may impact the quality of life of these individuals.
Clinical implications
Our findings provide further insights into cognitive alterations in people with migraine, specifically a decrease in creativity during interictal periods.
Impaired creativity in people with migraine can have serious consequences in their daily lives. For instance, it may worsen the impact of migraine on quality of life, disrupt stress management, affect the treatment and management of pain and challenging situations, and hinder treatment adherence by affecting individuals’ willingness to change their habits and try new strategies to manage their migraine.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are available upon reasonable request to the corresponding authors.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.