
Abstract
Literature documenting the location of pain at onset of migraine attacks and during established headaches in children and adolescents is sparse. Through a prospective study (2003–2005) of 200 children with migraine (ICHD-2: 1.1 and 1.2.1), we set out to document (i) the site of onset of pain and (ii) the location of pain during established attacks (on >50% of occasions) through semistructured interviews of patients and parents. Of the 200 children, the male:female ratio was 118 : 82 (1 : 0.69), the age range was 7–15 years (mean 11.8 years) and the duration of migraine 6 months to 4 years (mean 1.6 years). Ninety-three percent of subjects were ethnic Bengalis from the eastern Indian state of West Bengal, capital city Calcutta. Migraine types were: 1.1, 197 (98.5%); 1.2.1, three (1.5%). Location of pain at onset: 20.5% of subjects had unilateral onset; of these, 26.8% had eye pain, 65.9% frontal and 12.3% temporal pain. Thirty-three percent had bilateral location of pain, mostly bifrontal or ocular. None had vertex onset pain. However, in 35% of subjects, pain was holocranial at onset. Only 11.5% experienced pain in the occipito-cervical region at onset. Location of established headaches: in 53.7% of subjects with unilateral onset, headaches subsequently became holocranial. Hemicranial headaches occurred in only 19.5%. Of bilateral onset pains, 57.8% also became holocranial subsequently. In all, 73.5% of children ultimately experienced holocranial headaches. This study documents pain location at onset and during established headaches in children with migraine largely from a specific ethnic group.
Introduction
Paediatric migraine differs from adult migraine in more than one respect. This has resulted in debate regarding diagnostic criteria. The ‘footnote’ in the International Classification of Headache Disorders, 2nd Edition (ICHD-2) criteria (1) for migraine without aura (1.1) has clarified the situation substantially and has subsequently been validated (2). In the ICHD-2, the lower limit of headache duration has been reduced to 1 h, although the nosology of shorter duration of ‘migrainous’ headaches often encountered in clinical practice (fairly common in Indian children) remains to be addressed. The ICHD-2 ‘footnote’ (1) also mentions the location of paediatric migraine: ‘migraine headache is commonly bilateral in young children; an adult pattern of unilateral pain usually emerges in late adolescence or early adult life’ and ‘migraine headache is usually fronto-temporal’. ICHD-2 also comments on the rarity of occipital headache in children and calls for diagnostic caution to exclude structural lesions (1). Brief comments related to location of migraine headache in children have been made by Wober-Bingol et al. (3) and Winner et al. (4), and more recently by Winner and Rothner (5) and Hershey et al. (2). However, none has commented in detail regarding the location of onset pain, its subsequent evolution and the final location of pain during established attacks. A detailed pain location study has recently been undertaken by Kelman in adult migraineurs (6). It is also important to study phenotypic differences in different populations with varying geographical locations and ethnicity. The present study was undertaken (along with a similar study in adults) to document migraine pain location at onset and during established headaches in Indian children and adolescents largely of Bengali origin residing in the eastern Indian state of West Bengal, capital city Calcutta.
Materials and methods
The present study was carried out between September 2003 and December 2005 at the neurology out-patient department (tertiary care centre) of a large general hospital (550 beds) in the city of Calcutta in eastern India, with a predominantly Bengali population. A total of 262 subjects (age 7–15 years; 91.6% Bengali) diagnosed with episodic migraine attacks and having at least two attacks of acute migraine per month during the preceding 6 months of recruitment and not on any form of prophylactic medication during the same period were assessed through a semistructured questionnaire.
Interviews were always made in the presence of one or both parents and their responses to the questionnaire were also considered. Children thought to have chronic headache (uncommon in our experience) and variant forms of migrainous disorders (e.g. cyclical vomiting) were excluded. In our Institute, children up to the age of 7 years with neurological problems are generally cared for by paediatricians and referred to neurologists only when needed. Although paediatric seizure disorders are often referred, children with headache disorders <7 years old are seldom referred to the neurological services and on most occasions they turn out to have secondary headache disorders. Diagnosis of migraine and migraine subtypes were made according to the ICHD-2 criteria made available on the internet in 2003 and later published in February 2004 (1). Migraine headaches were diagnosed for headaches lasting ≥1 h as suggested in the above-mentoned ‘footnote’. Assessment was made through several stages (as had been done in the study of adult patients with migraine).
At the first visit, each patient was evaluated by one of the three participating consultants (authors) to confirm the diagnosis of migraine, identification of subtype and arrangement of relevant investigations to exclude secondary headaches as and when needed (imaging done in 88 patients and positive in only one patient).
During the second visit, 1 week (on average) later, each patient was evaluated through a semistructured questionnaire by a trainee physician specially assessing the site of location of onset pain and its subsequent location during established attacks in the majority (>50%) of headache spells in the preceding 6 months. Patients were asked to put their hands at the sites of onset pain, show with their hands the subsequent spread of the pain (if possible) and, finally, the locations of the pain during the established phase of the headaches. Descriptions of the terminologies relating to anatomical sites are given below at the end of this section.
During the third visit, usually a month later, each patient (in presence of parent/parents) was asked the same questions relating to location of pain by one of the authors (consultants) and results were compared with those of the interview by the trainees. In subjects in whom some discrepancies had been noted between the two responses, the patients (along with their parents) were offered the first responses and given the opportunity to make a definite choice between the two. Patients (and their parents) giving grossly discrepant or vague responses (not really of localizing value) were excluded from the study. Patients who failed to present for this stage of interview (even after a reminder) were also excluded.
Lastly, all response sheets were carefully evaluated by the corresponding author and only the first consecutive 200 subjects (93% Bengali) giving consistent (or near consistent) responses to questions relating to pain localization, both at onset and during established phase of headaches, were included for analysis.
Descriptions of terms used for anatomical sites of location are:
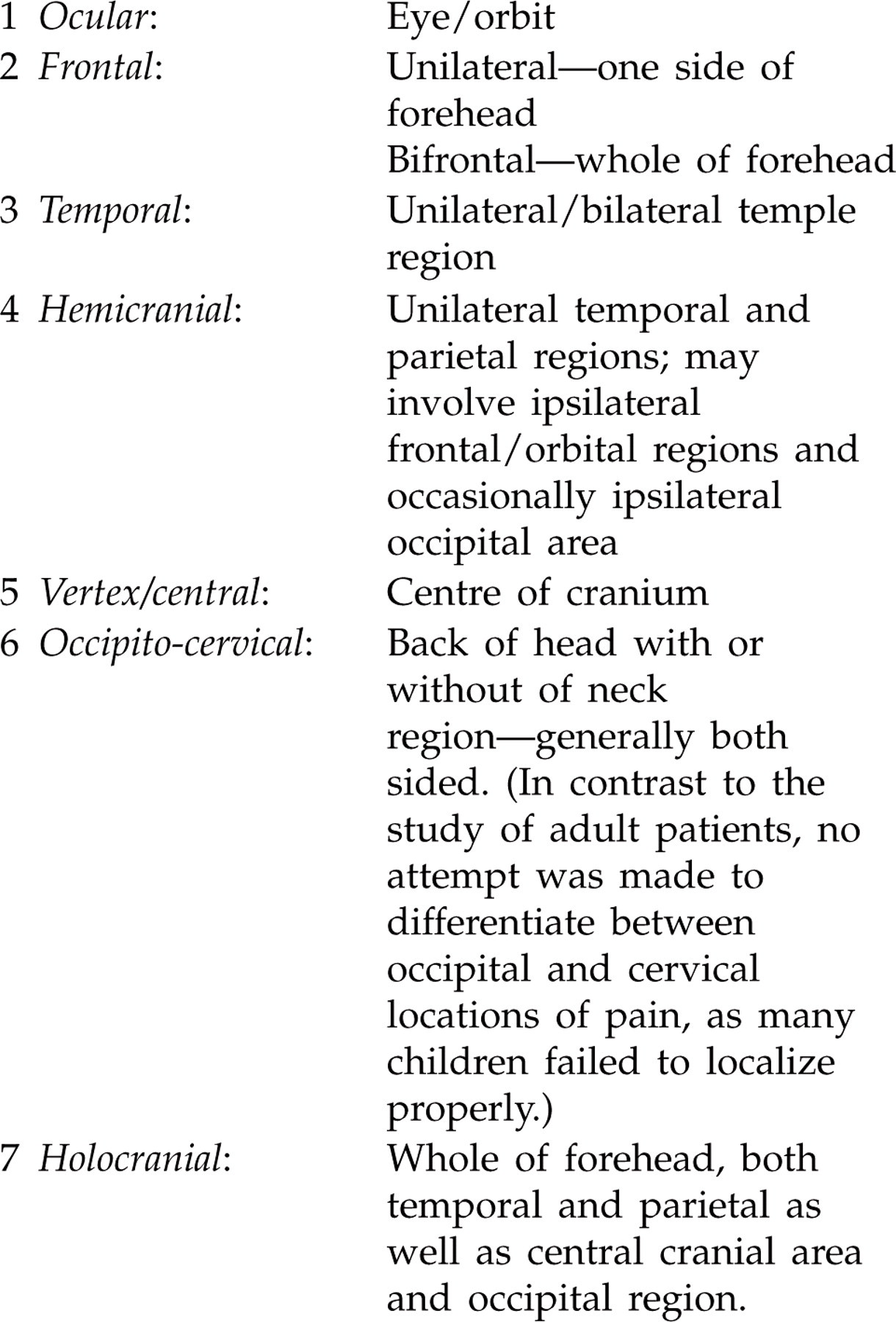
It can be seen that, while noting the location of pain, especially onset pain, the area mostly affected was taken into account. For example, pain involving one side of the forehead but extending a little into the temple region has been designated as frontal onset, and vice versa. This distinction is somewhat artificial, but necessary to make the final analysis more simple.
As the patient population involved older children and adolescents, responses to questionnaire were generally clear and consistent.
Results
Observations made in the present study are summarized in Tables 1–3.
Paediatric migraine: demography and clinical types (International Classification of Headache Disorders, 2nd Edition)

Location of pain at migraine onset (on >50% of occasions) (N = 200)

Location of pain during established headache phase vis-à-vis location at onset (N = 200)

Summary observations
Migraine in children and adolescents in Bengalis appears to be a slightly male-dominant disease.
Migraine with aura (MA) is rare in Indian patients and migraine in children andadolescents is no exception, especially amongst Bengalis.
In contrast to what is generally noted (and reported in western literature (6)) to occur in adults, only 20.5% of children had unilateral onset of pain during acute migraine attacks. Of these (n = 41), most (60.9%) had unilateral frontal location; ocular pain occurred in 26.8% and temple pain in only 12.2%. In no subject had onset pain been side locked.
Pain was bilateral in 33% of subjects (n = 66). Bifrontal pain at onset was found to be most common (56.1%) and was less commonly found in both eyes (27.3%) and bitemporally (16.6%). None had onset pain localizing in the vertex region.
Holocranial location of pain at onset was common, occurring in 35% (n = 70) of subjects.
Onset pain localizing at the occipito-cervical region was found in 11.5% (n = 23) of subjects, and was mostly bilateral. No attempt was made to differentiate between predominantly cervical and occipital localization (as had been done in the study of adult migraineurs), for reasons mentioned above.
In 31.7% of subjects with unilateral ocular, frontal and temporal location of pain at onset, pain remained at the same site during established headaches.
Only 19.5% (n = 8) of subjects with unilateral ocular, frontal and temporal location of pain at onset subsequently developed ipsilateral hemicranial headaches.
In contrast 48.8% of subjects with unilateral location of pain at onset, subsequently developed bilateral or holocranial headaches.
In 42.4% of subjects with bilateral (both eyes, bifrontal, bitemporal) location of pain at onset, pain remained at the same sites during established headache spells, but in the majority (57.8%), during established attacks pain had been holocranial.
All subjects with holocranial location of pain at onset (n = 70) continued to experience pain at the same location, but of varying intensity.
Of the small number of subjects with occipito-cervical location of pain at onset (n = 23), most (n = 17, 73.9%) subsequently had holocranial pain and in 26.1% (n = 6) pain remained localized at the same site. None developed hemicranial headaches.
In all, during the established migraine headache phase, only 10.5% (n = 21) of all subjects (n = 200) had experienced strictly unilateral pain. The vast majority experienced bilateral or holocranial headaches (n = 173, 86.5%) during established migraine. A minority of subjects (n = 6, 3%) experienced only occipito-cervical pain during established migraine attacks.
Discussion
On the whole, literature documenting location of migraine pain in children and adolescents is sparse. Also, the limited number of reports available (2–5) had actually looked at sites of pain location during established migraine attacks only, and the location sites of pain at onset and their subsequent evolution has not been addressed adequately. The present study was designed to look specifically at these aspects in children and adolescents with migraine, largely drawn from a particular group, Bengalis residing in the eastern Indian state of West Bengal.
Migraine headaches in children were diagnosed when headaches lasted >1 h according to recommendations made in ICHD-2 (1). Only migraine 1.1 and 1.2.1 of the general category were included; children with ‘migrainous’ headaches lasting <1 h (common in our population) had been excluded.
Based on the results of the present study, the following issues need discussion:
Migraine in children amongst Bengalis in eastern India appears to be a slightly male-dominant disease, compared with a slightly female predominance noted in all western series. We also observed this male dominance in an earlier study of chronic daily headaches (CDH) in children in the same population (7). CDH in adults in India is a female-dominant disease (8). Considering the socio-economic status of the patients seen at our department, it seems unlikely that headache problems in young females remain under-reported.
MA is rare in both children and adults compared with all western studies on migraine phenomenology, and this had been commented upon earlier by us (9).
Bilaterality of migraine pain location in children has been stressed in all previous western studies, including those of Weiner et al. (4), Wober-Bingol et al. (3) and the recently published validation study of Hershey et al. (2). Wober-Bingol et al. (3) found this in 55.4% of subjects and Hershey et al. noted bilaterality of established migraine headaches in as many as 82.7% of subjects. These studies did not mention pain location being holocranial and probably made no distinction between ‘holocranial’ and ‘bilateral’ location of pain. We noted ‘holocranial’ (as distinct from ‘bilateral’, meaning both ocular/orbital, bifrontal and bitemporal) distribution of pain both at onset (35%) and during the established phase of headache. Although there is probably little clinical (or pathophysiological) significance in the distinction between adjacent anatomical sites, we felt the need for this distinction for documentation purposes. We acknowledge that it has been difficult at times to make this distinction between ‘holocranial’ and ‘bilateral’ distribution of pain location in many young subjects during established headache spells. In view of this, in the final analysis of pain location during established headaches, ‘bilateral’ and ‘holocranial’ pain locations have been grouped together and noted to occur in 86.5% of subjects. This is very similar to the observation reported by Hershey et al. (2) and underscores one essential difference between pain location between adults and children with migraine.
Unilaterality of migraine pain location is well known in adults. Available western studies have noted unilaterality of paediatric migraine attacks in almost 30% of subjects (2–5). In the present study, strictly unilateral headache during established migraine attack was noted in only 10.5% of subjects. This distinction between our population and western subjects seems significant.
An important feature of the present study has been its location of the sites of onset of migraine pain and the recording of the sites of established head pain in relation to variability of sites of onset. This has not been attempted in the past. As the present study included mostly older children and adolescents (<15 years), subjects on the whole were fairly consistent in their responses to the questionnaires. Although it was difficult at times to differentiate between ‘bilateral’ and ‘holocranial’ headaches during established migraine pain, it was easier to make this distinction during onset of migraine attacks (possibly because of lesser intensity of the pain at onset). In contrast to unilateral location of pain during established migraine (10.5%), in 20.5% of subjects, pain was unilateral initially. Nearly half of these (48.8%) subsequently developed bilateral/holocranial headaches.
We have used the term ‘hemicranial’ to document headaches involving more than two anatomical locations on one side of head. This distinction may appear artificial, but provides a clearer anatomical idea of the headache location. The term ‘hemicranial’ has not been used in any of the recent western reports on paediatric migraine. The term ‘hemicrania’ indeed has some historical significance.
It is important to note that, even at onset, pain involved the whole of the head (holocranial) in 35% of children, but in none was headache onset at the centre of the head (vertex region). Wober Bingol et al. (3) have mentioned ‘median’ distribution of migraine headaches in 7% of children. The exact anatomical meaning of the term ‘median’ had not been explained, but perhaps it means pain over the centre (what we have called vertex/central location).
The ICHD-2 ‘footnote’ (1) refers to rarity of occipital location of migraine headaches in children and provides a cautionary note regarding exclusion of a secondary headache disorder. This is important. We noted occipito-cervical pain location during established migraine in only 3% of subjects, but 11.5% of subjects noted onset of pain in the same region, most (>70%) of which subsequently became holocranial, but none became hemicranial. On the whole, it appears that in children onset of migraine headache in the cervico-occipital region is common in Indian subjects, at least amongst Bengalis. Cervico-occipital location of migraine pain has not been adequately highlighted in western literature, except for the recent study of adults by Kelman (6).
Lastly, ethnicity needs to be given adequate importance when discussing the clinical phenomenology of any disorder where genetic factors seem to be implicated. This has not previously been attempted. Although Hershey et al. (2) have mentioned the ethnicity of subjects included in their study (quite diverse), no attempt was made to note differences, if any, between different groups. Our study had been based on subjects largely dominated by a single group (93% Bengalis). We have made no attempt to study any phenomenological differences between Bengali children and those of other ethnicity, because of the lack of statistical power such a comparative study would have (93% subjects vs. 7% subjects).
To summarize, the present study is important for its documentation of migraine pain location at onset and during established phase of headaches in children and adolescents largely drawn from a specific group (Bengalis in eastern India). There is a need for similar clinical studies in subjects belonging to other ethnic groups and geographical regions.