
Abstract
Background:
Chronic migraine can be challenging to treat and despite recent advances in treatment, there are cases that do not respond to current available pharmacological therapies.
Case:
We report a case of a 64-year-old male with a long history of chronic migraine who developed severe tremor-dominant Parkinson’s disease.
Conclusion:
After implantation of subthalamic deep brain stimulation (DBS), he reported not only benefit for his parkinsonian symptoms, but also a complete remission of his migraine attacks.
Introduction
Parkinson’s disease is associated with motor and non-motor features. For a long time, deep brain stimulation (DBS) has been successfully used for the control of bradykinesia, rigidity, and tremors in patients with Parkinson’s disease. 1 The benefit of DBS on non-motor symptoms such as pain and autonomic functions, remains to be elucidated, although there is growing evidence of its clinical usefulness. 2 In different populations, DBS has also been shown to be effective in conditions such as refractory epilepsy, chronic pain, severe forms of cluster headache and autonomic cephalalgias but has not been reported for the treatment of migraine. 1 Given migraine is associated with dopamine hypersensitivity and DBS has a wide neurostimulation effect including the dopaminergic network; DBS might offer a therapeutic option in refractory cases of migraine. 3
We present a case of chronic migraine that was alleviated post subthalamic DBS. To our knowledge, this is the first case that reported the beneficial effect of DBS for Parkinson disease on chronic migraine.
Case presentation
We present a 64-year-old gentleman with severe tremor-dominant Parkinson’s Disease, who was successfully treated with bilateral subthalamic deep brain stimulation (DBS) surgery (Figure 1). Prior to implantation, he had also suffered from chronic migraine for more than 30 years.

Subthalamic deep brain stimulation: Postoperative CT brain merged with preoperative MRI brain (FLAIR) with active contacts in the subthalamic nuclei. A: Coronal view and B: Axial view.
The patient had reported weekly headache attacks which occurs twice a week on average. They were unilateral with a sensation of retro-orbital pressure accompanied by nausea, dizziness with photophobia and phonophobia, which could last for several days and required multiple hospital admissions per year. Most of his attacks were preceded by scintillating scotoma and positive visual phenomena (flashes of lights and expanding zig-zag patterns). He used to miss 5–8 days of work due to migraine per year. His symptoms did not abate after trialing multiple medications, including paracetamol, non-steroidal anti-inflammatory drugs, triptans, betablockers, and tricyclic antidepressants. The patient does not have symptoms suggestive of sleep apnea such as morning headaches, snoring and lethargy. He did not use opioids for headache and did not suffer from medications overuse headache. Simple analgesia (paracetamol and NSAIDs) and triptans were not used more than 10 times per months. He was using nortriptyline as preventer for 5 years prior to the insertion of DBS. He reports complete resolution of headache after 1 week. His preventative medication was successfully weaned off and ceased 4 weeks post DBS.
His family history was positive for migraine with visual aura in his oldest daughter and grandson, who were both diagnosed in adulthood. Interestingly, after his DBS system was activated, there was not only an improvement of his parkinsonian symptoms, but the patient also noticed a complete remission of his migraines.
Deep brain stimulation targeting the subthalamic nuclei (STN) bilaterally was performed in 2015, at the age of 58 (Medtronic Activa PC, Minneapolis, Minn., USA). In 2017 the implantable pulse generators were replaced with rechargeable pulse generators (Brio, St Jude Medical, Plano, Texas, USA). During 6 years of follow-up in our movement disorder clinic and several adjustments of his DBS settings (Table 1 shows his latest settings), his headache attacks have never re-occurred, nor did he require pain medications, ED presentation, or further hospital admissions.
Deep brain stimulation (DBS) settings.

Discussion
To our knowledge this is the first case report of a patient with a dual diagnosis of a severe migraine and Parkinson’s disease, who did not only show improvement of motor symptoms, but also complete resolution of his migraine attacks after subthalamic DBS. This effect was noted after the DBS surgery and the patient remained migraine-free until his last follow up appointment, 7 years later. It is important to note that migraine improvement was previously reported after anterior thalamic DBS for a severe form of idiopathic generalized seizure. 4 In that case, Lendavi et al. reported clinical improvement in both headache frequency and intensity at the 6 years follow up review. 4 On the contrary, another group reported no significant change in migraine headaches 1 year post subthalamic DBS for Parkinson’s disease. 5 Studies on subthalamic DBS for cluster headache show improvement in symptoms after an average of 2 years suggesting that time might be a key factor. 3 For example, Huotarinen et al reported a resolution of cluster headache during 5 years follow up for a middle-aged male who underwent subthalamic DBS for advanced Parkinson’s disease. 6 Similarly, his parkinsonian symptoms have also improved. 6
DBS has been used for refractory cases of chronic cluster headaches with promising results. Given migraine has analogous features, it was hypothesized that it could be effective in chronic migraine. 1 The indirect positive effect on migraine after targeting the subthalamic nuclei with DBS can be explained by several possibilities. Functional MRI and positron emission tomography (PET) shows activation and hyper-perfusion of the hypothalamus in chronic migraine. This can lead to wide network activation including trigeminal nuclei. 1,7,8 The hypothalamus also plays a key role in activation of the pain matrix which includes many structures such as the thalamus, cingulate cortex and insula. Neuromodulation with DBS might alleviate headache by improving these pathways (Figure 2). 1
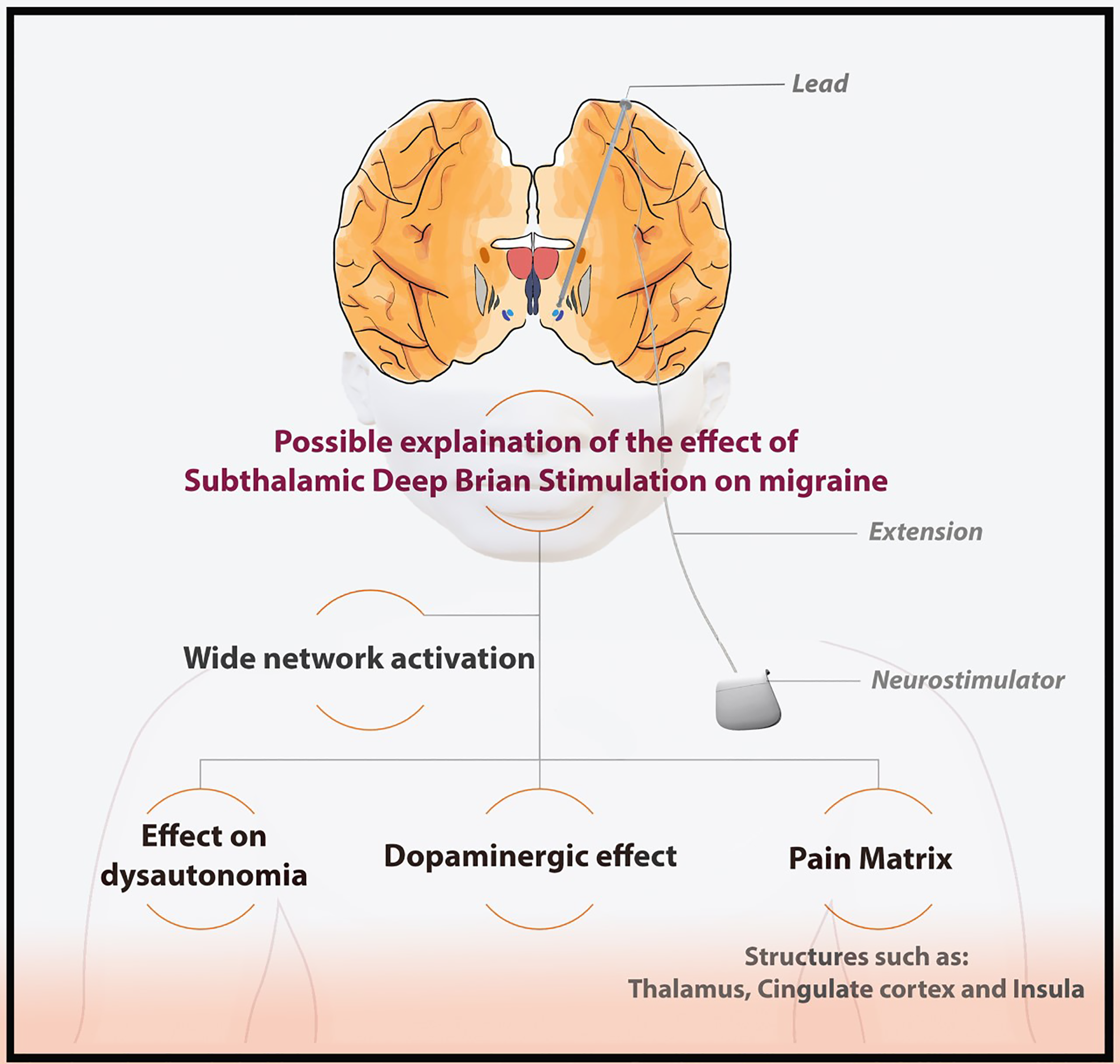
Possible explanation of the positive effect of subthalamic deep brain stimulation.
In addition to calcitonin gene related peptide (CGRP) and serotonin 5-HT, dopamine has been suggested to play a key role in the pathogenies of migraine through activation of the trigeminocervical complex. 9 Cubo et al. found that patients with Parkinson’s disease and migraine show better clinical response in motor symptoms compared to those without migraine. 10 Migraine has been associated with dopamine hypersensitivity. For example, dopamine agonists are associated with some of the symptoms seen in migraine such as nausea, vomiting and yawning. On the other hand, dopamine blockers have been used in the treatment of migraine. 10 Migraine also has autonomic features and DBS is thought to exert some positive effects on dysautonomia such as orthostatic hypotension that is often seen in Parkinson’s disease. 11
The major recent advances in migraine management include the use of calcitonin gene related peptide (CGRP) inhibitors but neurostimulation remains a reasonable option as an adjunctive tool for refractory cases. 11 Several methods of neurostimulation are available such as transcutaneous supraorbital stimulation, reparative magnetic stimulation and vagal nerve stimulation. These treatments are designed based on the theory of neuromodulation through the cerebral cortical excitability and cortical spreading depression which is associated with migraine. 12 Our case highlights that DBS might have a potential neuromodulation benefit in the treatment of migraine in selected cases where the pharmacological intervention is not sufficient. Given the potential serious side effects of intracranial stimulation such as infection and neurological deficits, careful patient selection is essential.
Conclusion
In summary, we describe a case with complete resolution of chronic migraine attacks after undergoing STN DBS surgery. DBS for migraines has never been described. A possible explanation for this is that DBS leads to wide network activation including hypothalamus, trigeminal nuclei and pain matrix. Future studies are needed to assess the potential effect of DBS on migraine.
Footnotes
Acknowledgments
We thank the patient for granting permission to publish this case.
Clinical implications
Migraine is associated with dopamine hypersensitivity and subthalamic DBS could be beneficial in the future for refractory cases of migraine due to its potential neuromodulation effect. Given the potential serious side effects of DBS and the current lack of evidence for DBS for the treatment of migraine, this remains a hypothesis only and clinicians are encouraged to report indirect positive and negative effect on chronic migraine when DBS is done with other neurological conditions such as epilepsy and Parkinson’s disease.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that there are no conflicts of interest relevant to this work. TJL received support from the Jan Meerwaldt Foundation for an Overseas Fellowship. All other authors report no disclosures.
Ethical approval
Approval of an institutional board or ethics committee was not required for this work. Written consent was obtained from the patient to use his MRI/CT imaging and clinical case details in the manuscript. We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this work is consistent with those guidelines.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.