
Abstract
Aim:
To help clinicians in the diagnostic approach of giant cell arteritis (GCA) by providing a better knowledge on headache patterns in GCA.
Methods:
Cross-sectional data of a cohort of 30 known GCA patients regarding symptoms, clinical signs, laboratory and pathology data were collected retrospectively.
Results:
Headache was experienced by the majority of our cohort (26/30; 87%) and the most common pattern reported was a continuous, unilateral pain centered in or around the temporal area (13/26; 50% of all headaches). Pain confined to the occiput or frontal areas of the head was rarely reported as well as migrainous or cluster-like headaches.
Conclusion:
This data suggests that the headache pattern in GCA is heterogeneous, but that the most common pattern is a continuous, unilateral, temporal headache. Several other patterns were infrequently reported and these should question the clinical diagnosis of GCA. A large prospective study will be necessary to further elaborate these findings.
Introduction
Diagnosis in giant cell arteritis (GCA) may be challenging due to sampling errors in temporal artery biopsies, which are still considered the gold standard. Therefore, the diagnostic workup may be comprehensive and invasive, and a high level of clinical suspicion is warranted in new onset headache over 50 years and more so in the absence of visual symptoms, jaw claudication or elevated ESR. 1 –3
Although headache is the most frequent mode of presentation, little is known about the headache profile in GCA. The classic headache described in GCA is a localized temporal pain, but the pain can also appear in other regions of the skull or be generalized. 4,5 In an attempt to further describe the clinical spectrum of presentation, with emphasis on headache, we studied all cases of GCA diagnosed in a neurological practice over a 3-year period, aiming at providing answers to diagnostic pitfalls.
Methods
Patients
In this retrospective cross-sectional study we included all cases diagnosed with GCA in the Canisius Wilhelmina Hospital (CWZ) in Nijmegen between 2015 and 2017, using the hospital’s claims database. Diagnoses were required to conform to the revised ACR criteria. 6 Suspected cases that failed to meet these criteria because of painless vision loss were required to have an elevated ESR, a positive temporal artery biopsy or both. Additionally, non-conformant cases with normal or unobtainable ESR and biopsy results were nonetheless included in the sample if they exhibited a swift and lasting response to high-dose prednisolone treatment.
First, we studied the files of all subjects with the claims code “temporal arteritis/polymyalgia rheumatica” and identified 27 possible cases of GCA. Six of these had been miscoded and were excluded from our analysis. Next, we extended our search to all subjects 50 years or over and coded as “other headache.” Finally, we screened a subset of files of individuals 50 or over coded as “TIA/amaurosis fugax.” Of 503 individuals coded as “other headache” nine were diagnosed with GCA and included for analysis. The “TIA/amaurosis fugax” sample comprised of 807 records, but because the screening of the first 400 records did not identify any cases further screening was abandoned.
Standard protocol approvals and registrations
For the aim of the study, cases were not subjected to any intervention, nor was their cooperation required at any stage. Though not formally required, the hospital’s ethical committee granted permission to effectuate our aims.
Clinical data
This study presents the analysis of retrospective data from patient files, collected by two clinicians (SV and WM) working in the hospital’s neurology department. We acquired data regarding patient characteristics, symptoms and signs at presentation, laboratory and pathology data. For headache, we collected data regarding location, laterality, temporal profile, quality and associated features. The distribution of the headache was assessed for each subject, first dividing all headaches between uni- or bilateral headaches and then mapping them to prespecified anatomical regions: frontal (i.e. the sensory projection of the first division of the trigeminal nerve), occipital (i.e. the sensory projection area of the occipital nerve), or temporal (i.e. the remaining area of the neurocranium). Distribution patterns were classified as “restricted” (i.e. perceived in one anatomical area), “contiguous” (i.e. perceived in two neighboring regions) or “hemicranial” (i.e. one half of the neurocranium). The temporal profile was classified as either paroxysmal (i.e. a sudden increase or recurrence of pain with stereotypical duration, separated by pain free intervals) or unremitting/continuous (daily pain of variable intensity, but without relapsing pattern).
Statistical analysis
Statistical analyses were performed using Microsoft Office Excel 2016 and SPSS Statistics 24. Patient characteristics and clinical data were described using descriptive statistics, which were presented as frequency (%) or mean and standard deviation unless stated otherwise. There were no missing data.
Data availability
The data from this study cannot be made publicly available because no patient approval has been obtained for sharing coded data.
Results
Population
A total of 30 cases were included in the study sample. It included 18 female patients and the mean age was 75 years (±8.1SD). Twenty-one patients measured up to the revised ACR criteria. Nine did not: four had a swift clinical response to prednisolone therapy, another three had acute visual disturbances (one with an elevated ESR <50 mm/h and two with biopsy pathology compatible with GCA), one had a borderline ESR-value (45 mm/h) and one had clear evidence for GCA on PET-CT.
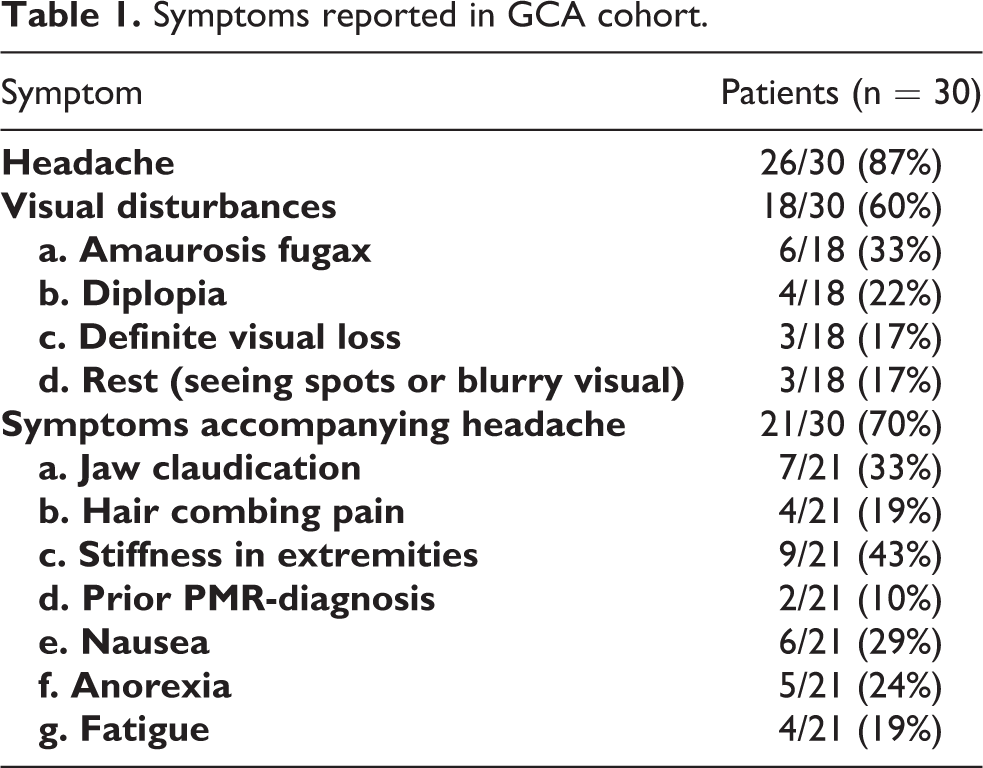
Symptoms
All reported symptoms are presented in Table 1.
Symptoms reported in GCA cohort.
Headache
Headache was reported most of all symptoms mentioned in our sample (Figure 1).

Distribution of all headaches reported.
Distribution
a. Unilateral headaches
• In the “restricted” group, the temporal area was most often exclusively affected (8/26; 31%), while pain restricted to the occiput or frontal area was exceptional.
• In the “contiguous” group, all patients had pain in the temporal area as part of a larger distribution (2/26; 8%).
b. Bilateral headaches
• The “bilaterally restricted” headaches, meaning localized to both frontal, temporal or occipital areas, were mainly temporal (4/26; 15%).
• In the “bilateral contiguous” group all had bilateral occipitotemporal pain, whereas bilateral frontotemporal pain was not reported.
In summary, the temporal area was involved in 88% of all patients experiencing headache in GCA, either unilateral or bilateral and either in isolation or as part of a larger distribution. The frontal area was only involved in 38% and the occipital area in 42% (Figure 2).

Headache patterns: all combinations of laterality, regionality and temporal profile reported. All uni- and bilaterally restricted headaches were counted as one region. For all uni- and bilateral headaches with a larger distribution, all regions involved were counted separately: for contiguous headaches 2 regions and for hemicranial headaches 3, leading to a total of 44 regions.
Temporal profile
An unremitting course of the pain was reported by the majority of subjects reporting headaches (23/26; 88%). Of those who described a paroxysmal course, most experienced repetitive short-lasting stabbing pain.
We combined the data on laterality, regionality and temporal profile to determine which headache patterns occurred frequently and which were uncommon. Because some patients described headaches in more than one anatomical area, each region affected was counted: two (contiguous) or three (hemicranial) areas. Bilateral areas only counted once, resulting in 44 headache patterns in 26 individuals. Unilateral continuous pain in (but not necessarily restricted to) the temporal area is by far the most frequently reported (13/26; 50%). Only one patient described a continuous unilateral pain that did not involve the temporal area. The next most common combinations were unilateral continuous frontal pain and continuous bilateral temporal pain (both 7/26; 27%). In contrast, neither uni- or bilateral paroxysmal frontal headache, nor bilateral paroxysmal occipital headache were encountered. All other combinations were infrequently reported.
Other symptoms
In some patients, the headache was accompanied by specific symptoms, of which nausea was recited mostly, followed by anorexia and fatigue. Only one patient reported vomiting and photophobia.
Most patients (18/30; 60%) experienced a variety of visual disturbances. Amaurosis fugax was reported six times and progressed to definite blindness once. Only half of these cases reported headaches. All patients with jaw claudication and pain during hair combing reported headaches.
Discussion
In this cross-sectional study of patients with clinically confirmed GCA we found that most headaches were continuous and unilateral (respectively 88% and 62% of subjects). However, the most distinguishing feature of the headaches was a localization in or around the temporal area (88%). When combining this localization with continuous and unilateral profiles, we were able to correctly identify 50% of all GCA subjects reporting headaches. In contrast, paroxysmal frontal headache was not reported in our study, but all other pain profiles were described. With the exception of the one patient reporting vomiting and photophobia, no accompanying symptoms indicative of migraine were found. Moreover, ipsilateral cranial autonomic symptoms (indicative of cluster-like headaches) were not reported, although it must be stressed that due to the retrospective data retrieval this may be due to documentation bias.
As a neurologic clinic specialized in headache, we were able to include a relatively homogenous study-sample, diagnosed using a comparable workup. Because the proportion of GCA cases with headache in our study were in line with previous reports (86%), we believe that it is likely that our study resembled previously reported populations. 4 There are, however, several limitations of this study that deserve consideration when interpreting the results. First, because of its retrospective design, we encountered a large variability in the way data was reported by different clinicians. Secondly, because this study was a mono-center study, the sample size remained rather small and we cannot fully exclude selection bias. Furthermore, our cohort did not fully meet the 2016 revised ACR criteria, although we provided several arguments to support our methods. Future research should address these limitations in our design. In addition it is important to realize that an atypical headache may still be the presenting manifestation of GCA. 7
With this study we aimed to provide a better knowledge of the headache patterns in GCA cases, that may lead to a less complicated diagnostic approach. In conclusion, there is no such thing as a specific headache pattern in GCA, but half of our study-sample describes a unilateral, unremitting, temporal headache. Pain confined to the occiput or frontal areas of the head was rarely reported. Similarly, paroxysmal headache with migrainous or cluster-like features was exceptional.
This suggests that these headache types should question the clinical diagnosis of giant cell arteritis. A large prospective and controlled study is needed to refine and further elaborate these findings.
Clinical implications
We report on the headache characteristics of a small group of patients with clinically confirmed giant cell arteritis.
Fifty percent of all GCA patients reporting headaches described a unilateral, continuous, temporal headache.
Paroxysmal pain as well as pain restricted to the occiput or frontal areas of the head were rare in our study.
Footnotes
Acknowledgements
The authors thank Dr Aad Verrips for critically reading the manuscript and making suggestions for improvement.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Wim M Mulleners has received personal fees from Ely Lilly for medical advice.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.