
Abstract
The author set out to review the thought processes of Bayard Horton as he was clinicopathologically describing the first cases of temporal arteritis. The Mayo Clinic records of the original temporal arteritis patients were examined. Horton obtained the first biopsies of the temporal arteries in temporal arteritis and was the first to describe the histopathology. Horton initially thought his first two patients had actinomycosis of the temporal arteries, but later abandoned this diagnosis. He reported these two patients in 1932 as ‘an undescribed form of arteritis of the temporal vessels’. He was the first to describe jaw claudication. He saw a patient with blindness and symptoms suggestive of temporal arteritis before this complication was described in the literature, but initially felt the patient had some other disease. The sedimentation rate was elevated in his first patient. He cared for the first temporal arteritis patient ever treated with cortisone.
Introduction
Jonathan Hutchinson gave the first clinical description of temporal arteritis in 1890 (1–3). Max Schmidt reported a patient who probably had temporal arteritis in a 1930 article on intracranial aneurysms (3, 4). Neither Hutchinson nor Schmidt obtained temporal artery biopsies. Bayard Horton (Fig. 1) and his Mayo Clinic colleagues obtained the first biopsy specimens of the affected temporal arteries (2, 3, 5). Giant cell arteritis is referred to as Horton's disease. Previous authors have outlined Horton's important contributions to our understanding of temporal arteritis (2, 3, 6). This article will examine his contributions in more detail by reviewing the original clinical records of the first several patients that Horton diagnosed with temporal arteritis.

Bayard Horton.
Methods
The Bayard Horton Archives at the Mayo Clinic were reviewed. Horton's list of patients with temporal arteritis, which he kept for research purposes, was found. The Mayo Foundation Institutional Review Board approved a retrospective chart review of these patients. Horton's published papers on temporal arteritis and his personal correspondence in the St Mary's Hospital and Mayo Foundation Archives were reviewed.
Results
Temporal arteritis diagnosis
Horton's first patient
Horton saw his first patient with temporal arteritis in early 1931. This 50-year-old woman had symptoms we now recognize as typical of the disease (headache, scalp tenderness, weight loss, fever, night sweats). She was also hypertensive. Both temporal arteries were enlarged. The patient was anaemic and had an elevated sedimentation rate (Fig. 2). After seeing the patient for the first time on 7 April 1931, Horton wrote the following in the chart:

Erythrocyte sedimentation rate in Horton's first patient with temporal arteritis.
‘Has new indurated areas along arteries in temporal regions. Largest in left temple – quite tender. Does not suggest ordinary thrombosis – [x]ray skull for metastases. Believe this patient has a malignancy somewhere. Question of a hypernephroma not ruled out, but no definite indications for cysto, although I would like to have one done. Slight stiffness in the neck muscles noted for 2 or 3 days.’
On 9 April, Horton wrote that the ‘xray shows evidence of pituitary tumour – urine negative for Bence-Jones’. Later that same day, Horton and his fellow vascular medicine specialist George Brown wrote a chart note together:
‘Hardened nodules along temporal arteries – but vessels not thrombosed – tender nodules of arteries suggest peri-arteritis nodosa. This could explain fever. Would consider biopsy of scalp vessel. Note evidence of pituitary tumour.’
In a 1957 letter to the Mayo Clinic Board of Governors, Horton wrote the following about his visit on 11 April 1931 (7):
‘As I entered her room on the morning of April 11th, the light from the window, falling across the left side of her face and head, clearly outlined the enlarged red and somewhat nodular left temporal artery. I had the artist make a sketch of the left side of the head (Fig. 3). Later that day, I persuaded one of the surgical first assistants to resect the temporal artery’ (p. 2).

Artist's sketch of the enlarged temporal artery in Horton's first patient with temporal arteritis. From Horton BT. Temporal arteritis: a focal localization of a systemic disease. In: Council on Scientific Assembly, American Medical Association, editors. AMA scientific exhibits 1955. New York: Grune and Stratton 1955 : 385. Reproduced with permission from the American Medical Association.
Temporal artery biopsy showed a granulomatous arteritis. Actinomyces was found in culture from the artery, and thus the patient was treated with potassium iodide. Horton felt this original patient had actinomycosis of the temporal arteries, as evidenced by the letter he sent to the referring physician upon the patient's discharge from hospital in May 1931 (Fig. 4). In this letter, Horton also wrote:

Hospital discharge letter from Horton to the referring physician of his first patient with temporal arteritis.
‘We were of the opinion, at first, that these nodules along the temporal vessels might be metastasis from some unknown malignancy, and for that reason X-rayed the head. We were surprised to find enlargement of the pituitary gland, but in view of the fact that the patient had no objective neurologic findings we did not feel that any surgical treatment was indicated at this time.’
Horton saw the patient in the clinic on 3 November 1931 and wrote:
‘Patient states that during past two weeks she has had a recurrence of the red, painful nodules in both temporal regions, and that these nodules have been along the course of the vessels. From a clinical standpoint, these are the same lesions which [the] patient had here in April of this year.’
In September of 1932, Mayo pathologist Thomas Magath determined that the actinomyces was a contaminant (8). Horton saw this patient last on 3 December 1932:
‘2 weeks ago began to develop painful areas along left temporal artery. The tender segments of the artery still pulsate, indicating, I believe, that she has a periarteritis in the area. What apparently happens is that this produces internal changes, and later, thrombosis.’
The patient was admitted to the hospital in February 1933 for congestive heart failure and marked renal insufficiency. Her temporal arteritis had not recurred since December 1932. She gradually failed after she returned home and died 1 month later. An autopsy was not performed.
Horton's second patient
A 68-year-old male was seen in May 1931 with a similar clinical presentation (4 weeks of headache, scalp tenderness, weight loss, intermittent fever, night sweats). The patient was anaemic. The sedimentation rate was not determined. On 27 May 1931, Mayo physician George Brown wrote:
‘1 month ago pain and tenderness both frontal areas. Localized along superficial vessels. Exam show calcified arteries? frontal area – red and tender III. May be an acute thrombosis or localized phlebitis. Dr Horton see.’
On 29 May 1931 Brown wrote:
‘Impresses me as a periarterial infection – similar to case of actinomycosis of artery in woman pt. Should be in hospital – biopsy of vessel. Dental sepsis.’
On 29 May 1931 Horton saw the patient for the first time and wrote:
‘Should have biopsy right temporal vessel – remove at least 2–3 cm of the vessel for cultures and microscopic study.’
Actinomyces was found in culture from his resected artery. On 12 June 1931, George Brown wrote:
‘Pt. seems much better. Local vessel lesions have subsided. Has had eight teeth extracted and balance should be removed at home. Continue potassium iodide. If Hgb low – iron citrate.’
In September 1932, the actinomyces was determined to be a contaminant. The patient wrote to Horton in 1935 that he had ‘fully recovered and [had] not had any recurrence in the least’.
Horton's disease
Horton and colleagues reported these two patients on 7 December 1932 as ‘an undescribed form of arteritis of the temporal vessels’ (5). The authors commented (5):
‘Actinomyces were found in pure culture from both resected arteries, but after careful study these organisms were found to be exactly like common Actinomyces found in the soil, and at present we do not regard these organisms as of aetiologic significance’ (pp. 700–701).
The authors also stated (5):
‘The two cases which form the basis of this report represent a new clinical syndrome, the aetiology of which is still obscure. At the present time no name can be given to this condition, but other cases will probably be found and the condition dignified by nomenclature’ (p. 701).
Temporal arteritis was officially recognized as a disease entity in a 1946 JAMA editorial (9).
Horton's clinical research was performed at St Mary's Hospital in Rochester, Minnesota. In a letter to Sister Domitilla (former superintendent of St Mary's Hospital), Horton summarized how he discovered this new disease after seeing these two patients (10):
‘In the Spring of 1931, I recall walking into room 310, St. Mary's in the old building, and seeing a patient by the name of … Her chief complaint in April, 1931, was with reference to headache, general malaise, and lassitude, and symptoms suggesting a mild sepsis. I was intrigued by the fact that her temporal arteries were prominent, nodular and tender to the touch. They were thrombosed. I had never observed this clinical picture before. Approximately two hours later, I met Dr Leonard Rowntree … He casually remarked … “What's new? Can I be of any help?” I remarked, perhaps just as casually, “I have just discovered a new disease”. Maybe the average physician would have “shot back”, “Oh, yes, and what else?” But not Dr Rowntree, for he promptly replied, “I would like to see it”. He looked at [the patient] and hurriedly palpated the enlarged, nodular temporal arteries … and replied, “You are right, this is a new disease”. About 5 weeks later, while … talking with the late Dr George Brown, a bald headed man came walking down the corridor toward us. I was discussing the case of [the first patient] with Doctor Brown as the [male] patient approached us. Doctor Brown looked up and said, “If she represents a new disease, here is a second patient with the same illness”. That proved to be true' (pp. 1–2).
Temporal arteritis and vision loss
In 1938 Jennings was the first to describe vision loss in temporal arteritis (11). On 23 July 1937, Horton saw a 70-year-old man with 6 weeks of headache, weight loss and night sweats. One month after these symptoms started he lost vision in one eye and then 1 week later the other eye. His temporal arteries were tender and thrombosed without erythema or warmth. Ophthalmological examination 2 weeks after the last eye became blind was unrevealing, aside from documenting the blindness. The Mayo ophthalmologist William Benedict felt that the patient's blindness was ‘due to disturbance of the circulation along the optic pathways as a result of arteritis’. Because of the vision loss and the temporal artery biopsy results, Horton initially felt that the patient did not have temporal arteritis. Horton wrote the following in a letter to the referring physician:
‘On examination of the artery microscopically, it was evident there was a mild arteritis present but it is different than that previously observed by us and I do not believe it corresponds in any way to the syndrome which we described. In none of our previously described cases has blindness been noted. The aetiology of his condition from my standpoint is still obscure.’
Horton later realized that the patient did indeed have temporal arteritis (Fig. 5). Horton did not report cases of vision loss associated with temporal arteritis until 1943 (12).

Notation by Horton in the chart of a patient with vision loss secondary to temporal arteritis.
Temporal arteritis and jaw claudication
In 1944 Horton was the first to report jaw claudication in association with temporal arteritis (13). He wrote (13):
‘It is interesting to note that during the past decade I have seen many patients with temporal arteritis who have complained of pain in the jaw, but it did not occur to me until two years ago that the pain itself was of the intermittent claudication type. The pain is due to ischemia of the muscles of mastication. The facial arteries are easy to palpate, but in routine practice even those who specialize in the field of peripheral vascular disease fail to make observations of these vessels. Hence the pain of intermittent claudication of the jaw had been previously overlooked.
‘A woman, aged 64 years, who had all the classic findings of temporal arteritis, also had bilateral thrombosis of the facial arteries. Chewing resulted in intermittent claudication of the jaw. This pain occurred only with chewing and promptly disappeared with rest. A segment of the thrombosed facial artery was resected for special study. The microscopic appearance of the vessel was identical to that which we have previously described as characteristic of the syndrome, temporal arteritis. I know of no specific treatment for this syndrome. This patient eventually developed an adequate collateral circulation in the face so that she no longer had pain with chewing’ (pp. 5–6).
Horton saw this first patient with jaw claudication and temporal arteritis in 1942. Figure 6 is a letter written by Horton on 14 February 1942 to the Mayo Foundation in an attempt to obtain charity care for the patient, as she could no longer afford treatment. The Mayo Foundation granted Horton's request and the patient was treated free at St Mary's Hospital for a further 2 weeks.
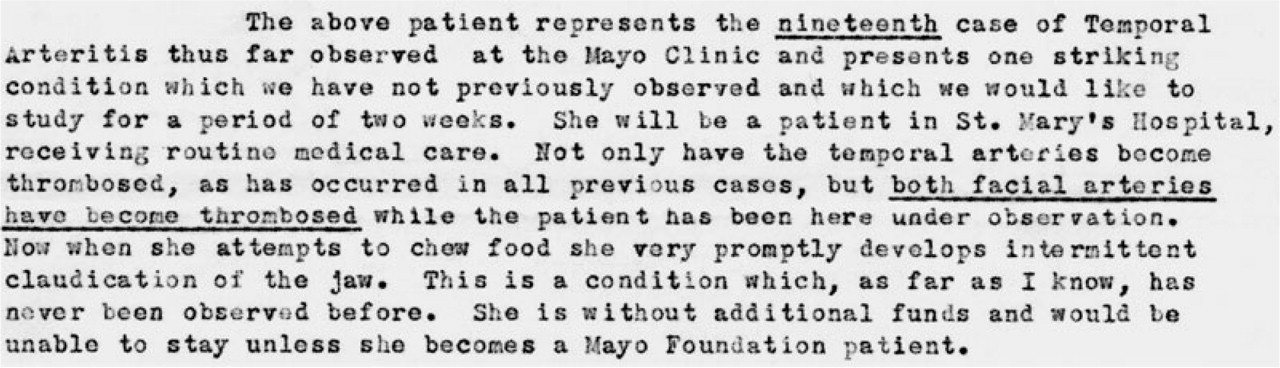
Letter sent by Horton to the Mayo Clinic Board of Governors in an attempt to obtain charity care for the patient, the first to be reported with jaw claudication.
Temporal arteritis and the sedimentation rate
In 1938 Jennings was the first to report an elevated sedimentation rate in temporal arteritis (11). Horton's first patient had an elevated sedimentation rate, but he did not report it in his 1932 paper (5) (Fig. 2). In a letter in the Mayo Foundation Archives, Horton confirms that in his first patient, ‘the sedimentation rate was 67 mm in one hour’ (7).
Temporal arteritis treatment
In 1942 Horton gave his first patient with temporal arteritis and jaw claudication Kendall's adrenocortical extract and commented in the clinical record that it had had no effect (Fig. 7). This extract was not the pure cortisone that was later used by his fellow Mayo Clinic vascular medicine specialist Richard Shick (14). Although Horton comments negatively in Fig. 7 about his first attempt at using histamine to treat his original patient with jaw claudication, he later stated that intravenous histamine helped another patient with jaw claudication (15). He initially felt intravenous histamine gave some symptomatic headache relief (16). Horton later clarified in a 1977 interview at the University of Virginia that histamine had no significant influence on the disease (17). In 1948, Chavany and Taptas reported clinical improvement with steroids (testosterone propionate plus desoxycorticosterone acetate, then whole adrenal cortical extracts) (18). In 1949 Horton was involved in the care of the first temporal arteritis patient ever treated with cortisone, and pondered in the clinical record whether this treatment would prevent blindness (Fig. 8). In 1950, Horton's colleague Shick reported clinical improvement with cortisone in two temporal arteritis patients (14). Horton felt cortisone was the treatment of choice in temporal arteritis (16). He wrote in 1955 (16):

Horton's chart comments on his attempts to treat his first patient with temporal arteritis and jaw claudication. He notes that Kendall's cortical extract and intravenous histamine gave no relief.

Horton's chart comments about the first temporal arteritis patient ever treated with cortisone.
‘Cortisone has been used in the treatment of temporal arteritis at the clinic since November 1949. The incidence of blindness has been definitely decreased since cortisone and corticotropin (ACTH) have been employed in its treatment’ (p. 142).
Temporal arteritis pathophysiology research
In 1946 Horton reported that finely ground portions of resected specimens of temporal arteries had been injected adjacent to the temporal arteries in five normal volunteers, aged 70–74, and none developed temporal arteritis (19). This was reported after his paper on vision loss associated with temporal arteritis (12). Horton commented in 1975 that this 1946 study proved that temporal arteritis could not be transferred from one human being to another (20).
Discussion
Horton and colleagues obtained the first biopsy specimens of the temporal arteries in giant cell (temporal) arteritis and were the first to describe the histopathology. Horton initially thought his first two patients had actinomycosis of the temporal arteries, but later abandoned that diagnosis. Horton and colleagues reported these two patients in 1932 as ‘an undescribed form of arteritis of the temporal vessels’ (5). They felt it was a ‘focal localization of some unknown systemic disease’ (5). Kvale (a Mayo physician) wrote that Horton and colleagues were unaware of Hutchinson's prior clinical description of temporal arteritis (21).
Horton correctly stated in his 1934 paper that his first patient was 50 years old at the time of diagnosis, but did it in such a way that it was difficult for the reader to be certain of this fact (8). In the case description, Horton writes ‘an unmarried woman, aged 50, was first admitted to the clinic in May, 1917’ (8). This admission was for a general medical examination, and the patient did not have symptoms of temporal arteritis at that point (8). Horton then goes on to describe several clinic or hospital admissions (primarily for hypertension) over the subsequent years before finally arriving at the hospitalization for temporal arteritis, which occurred 14 years after the patient initially presented to the clinic (8). Once Horton starts describing the hospital admission in 1931 for temporal arteritis, he does not clarify that she was actually 50 years old on that particular year, when he started caring for her (8). Horton appears to have been confused about the patient's age himself while writing this 1934 paper, because in the summary of the 1934 paper he states the patient was 55 years of age at the time of diagnosis (8). In subsequent papers he repeats his error, stating that his first patient was 55 years old at the time of diagnosis (22, 23). Understandably, other authors have repeated Horton's mistake concerning the age at time of diagnosis (2, 6). Another author was off the mark by 14 years (3), because of the confusing way that Horton presented his patient's age in his 1934 paper (8).
Horton was the first to describe jaw claudication in the disorder (13). His unique vocation as a vascular medicine specialist with a strong clinical interest in headache prepared him well to make this seminal observation. Horton wrote several articles on claudication of the extremities (24, 25). He saw a patient with blindness and symptoms suggestive of temporal arteritis before this complication was described in the literature, but initially felt the patient had some other form of arteritis. Although he was not the first to report an elevated sedimentation rate in the disease, it was elevated in his first patient. Sedimentation rate determination was not performed in the subsequent six patients whom Horton diagnosed with temporal arteritis (22). An elevated sedimentation rate was not mentioned in Horton's papers of 1932, 1934, 1937 or 1938 (5, 8, 22, 23), showing he was slow to recognize the importance of this test in helping diagnose temporal arteritis. Horton first wrote about the high sedimentation rate in temporal arteritis in 1949 (15), 11 years after it had been first noted by Jennings (11).
He was involved in the care of the first giant cell arteritis patient ever treated with cortisone and felt it was the treatment of choice (16). Why the Mayo vascular medicine specialist Shick, rather than Horton, was chosen to investigate cortisone in the treatment of temporal arteritis is unclear. This decision may have been made because some of Horton's colleagues felt that his research was not scientifically rigorous (26). Horton's 1946 pathophysiology research, involving the injection of portions of arteritic vessels near normal subjects' temporal arteries, would not receive Institutional Review Board approval today (19). Horton does comment that the injected ground portions of the resected arteries had given negative results on all culture media, and that inoculation of guinea pigs, white rats and rabbits with some of the biopsy material had given negative results (19). Regardless, to a modern reader this study seems dangerous, since blindness secondary to the disease had been reported in 1938 by Jennings (11), and Horton had reported blindness in three patients in 1943 (12). It is possible that this research was carried out before Horton wrote this paper in 1943, as the 1946 temporal arteritis pathophysiology paper does not clarify during which time period this research occurred (19).
Horton is also credited with bringing cluster headache (‘Horton's headache') to the attention of the medical community (27). He was a smart man, a keen clinical observer and a very hard worker. A quote from a letter to the Mayo Clinic Board of Governors in 1957 outlined his research philosophy (7):
‘Wonder is the chief ingredient of the investigator. He, who can no longer wonder – no longer feel amazement – is as good as dead – a snuffed out candle, as Einstein expressed it. The history of medicine is the history of but a few people. It is only the few who leave their foot prints on the sands of time. If a man ever expects to do so, he must wear his “working shoes”’ (p. 3).