
Abstract
Objectives:
To evaluate a multidisciplinary group intervention, the migraine patient school (MPS), for patients with severe, mostly chronic migraine.
Method:
A 13-week group intervention program including seven sessions of patient education, practical body awareness and relaxation exercises, and home assignments was performed in small groups with 5–11 participants. Four groups were consecutively included from spring 2014 to fall 2015. Headache diaries and standardized and study-specific questionnaires were used for evaluation at baseline before MPS (pre-interventional phase), and at follow-up.
Results:
Twenty-four of 30 included patients completed the study, i.e. attended ≥ four sessions. Most participants found it rewarding to participate in the MPS and easy to take part in, understand and complete home assignments. Validated standardized questionnaires delivered before, and after (follow-up) MPS showed that the impact on life (HIT-6) and avoidance behavior (PIPS-A) were significantly improved whereas quality of life (MSQL), anxiety and depression (HAD) and perceived stress (PSS-14) did not show a statistically significant change.
Conclusion:
The Migraine patient school with a multimodal educational and behavioral group intervention program was feasible to perform and seem to benefit patients with severe (high-frequency or chronic) migraine.
Keywords
Introduction
Migraine is characterized by attacks of moderate to severe headache associated with light and sound hypersensitivity, nausea and vomiting. 1 The frequency of migraine attacks varies during the life span both in and between patients. 2,3 Attacks can be induced by many triggers of which hormonal changes in women and stress are the most powerful ones. 4 The unpredictable occurrence of attacks often adds to stress and a feeling of shortcomings. Stress initiates a vicious cycle leading to even more frequent attacks. 4
The prevalence of self-reported migraine and severe headache in Sweden 5 is about 13%. Chronic migraine, 1 is present in 1–2%. 6 The disorder leads to loss of function, emotional and physical stress, and affects both family and working life. 7,8 Besides a loss of quality of life (QoL), migraine leads to high societal costs. Estimates from Sweden and Norway range from EUR 6,200 to EUR 57,800 per year depending on number of migraine days/month, 9 with most (91%) due to indirect costs among patients with chronic migraine. 10
The treatment of migraine focuses not only on effective pharmacological treatment of attacks and attack prevention, 11 but also on the life situation of the patient and on how to reduce stress and other trigger factors. 12 Non-pharmacological self-management interventions are found to reduce pain intensity and headache related disability. 13 There is evidence suggesting that group interventions might be more effective than individual training. 13 Group interventions can have a multidisciplinary approach and include patient education, cognitive behavioral treatment, mapping of individual migraine triggers and stress reduction interventions. Taken together, this will give the individual more control of the disease, enable initiation of lifestyle changes and achievement of a better QoL. 14 –16 We have for some years given a group intervention for patients with severe migraine at our University Hospital clinic. This migraine patient school (MPS) with a structured multimodal approach has not previously been scientifically evaluated for patients with severe migraine.
The aims of this study were to evaluate feasibility from the patient perspective regarding participation and positive effects of the MPS among patients with high-frequency or chronic migraine (primary endpoint). Furthermore, to explore if the outcomes of the MPS as a group intervention could be captured by validated questionnaires and headache diaries (secondary endpoints).
Material and methods
Study population
Migraine patients, seeking care for severe (high-frequency or chronic) disabling migraine, at the outpatient Headache Centre, a tertiary referral unit, at the Department of Neurology, Karolinska University Hospital Huddinge, Sweden, were informed about the MPS by advertisement in the waiting room. Inclusion criteria were: 1) males or females between 18 and 65 year of age, 2) a history of migraine diagnosis with or without aura (IHS)
1,17
and 3) severe (high-frequency or chronic) subtype evaluated by the treating physician based on medical records and a headache severity score in Headache Impact Test (HIT-6)
Study design and implementation
The patients received an information letter prior to the MPS study start informing them on the aim of the study and the detailed MPS program.
An experimental study design was used with a 4-week pre-intervention phase (A), a 13-week intervention phase (B) i.e. the MPS program described below and a 12-week follow-up phase (C), see Figure 1.

Study design. Q = questionnaires distributed. Headache diaries reported before (A) and after (C) intervention.
Description of the MPS program
The MPS was a 13-week group intervention focused on a combination of theoretical headache education and physical/behavioral training using the Basic Body Awareness Therapy (BBAT) technique. 18 –20 This technique focuses on movement quality and how movements are experienced and performed. The underlying assumption is that a person’s lack of awareness of the body regarding physical, mental, and relational factors can lead to pain and impaired movement quality and function. Thus, the aim is to develop body awareness and strengthen basic functions. Key elements are postural stability, free breathing, and mental awareness. The BBAT can be performed individually or as a group intervention, and the movement awareness training is performed in different positions, e.g. standing, walking, sitting, and lying down. In the MPS, all seven sessions included BBAT training aiming to increase participants’ contact with their bodily signals, such as muscular tension and breathing patterns, to increase their ability to better understand and regulate these signals. Relaxation techniques used were progressive relaxation and applied relaxation (AR). 21,22
The MPS included seven meetings (sessions) 1–2 weeks apart, each session had its own theme. 12,16 To make it convenient for the participants, and to minimize interference with work and family life, all group meetings were scheduled to the afternoon with start at 4 pm in weekdays, each session lasting 2.5 hours. The MPS was held by a headache specialist/neurologist and a physiotherapist specialized in pain/headache and cognitive behavior strategies. The themes were: 1) “Stress and calm (stress physiology),” 2) “Exercise (physical activity),” 3) “Diet,” 4) “Thought patterns,” 5) “Emotional life (handling of emotions),” 6) “Approach to yourself and your environment (attitudes),” and 7) “Overall evaluation of the MPS.” 16 Participants who missed certain sessions received all material by email/post to enable practice at home and thereby to continue to the next session. No extra follow-up sessions were given.
The first MPS meeting started with presentation of group members and the MPS program. 16 All other meetings started with a short discussion and evaluation of the previous session. After a short break (coffee/tea, sandwich) the specific theme of the session and home assignments were introduced as a short lecture and discussion. Each session continued with a theoretical part of headache education given by the headache specialist/neurologist. The lectures were covering various aspects of migraine, tension-type headache, medication overuse headache, and headache and sleep in an integrative fashion. Written educational material of the themes had previously been developed and used in an internet-administrated trial in patients with episodic migraine 16 and this material was distributed for home assignments and group discussions the following session. All sessions ended with a 45-minute-long training session led by the physiotherapist with “body awareness exercises,” (BBAT) and relaxation (AR) exercises.
Measurements
A study-specific questionnaire was used for collection of baseline patient characteristics. Migraine diaries on paper (see supplementary material) were used for documentation of number of migraine days and severity (rated as mild, moderate or severe), number of other headache days and impact on daily life (DL) (rated as none, mild, moderate or severe). Each patient was asked to fill out the diaries during a 4-week pre-intervention phase (week 1–4) and during the last 4 weeks (week 9–12) of the follow-up phase, see Figure 1.
The participants were asked to give their evaluation of each session of the MPS program. Perceived experiences of previous group sessions were rated with a numeric rating scale (NRS) ranging from 0 (not at all rewarding) to 10 (very awarding). Perceived ability to take part and understand the previous session and ability to complete home assignments were rated on NRS-ranging from 0 (with great difficulties) to 10 (easily). After the last session, the NRS was used for their evaluation of the overall experience of those aspects i.e. perceived global experience of the MPS and ability to complete the home assignments (feasibility). There was also a possibility to add free comments in the evaluation forms.
In addition, participants were asked to fill out the following questionnaires three times before and three times after the MPS, see Figure 1:
The HIT-6 17,23 was used to evaluate the impact of headache on the life situation of the patient. Scores ≥56 are judged as a severe impact of migraine.
Experienced stress was evaluated with the Perceived Stress Scale (PSS-14). 24
The Migraine-Specific Quality of Life Questionnaire (MSQoL) 25 was used as measures of QoL.
Fusion and avoidance behaviors were evaluated with the Psychological Inflexibility in Pain Scale (PIPS). 26 –29
The Hospital Anxiety and Depression Scale (HAD) was used to find indications of concomitant anxiety and depression disorders. 30,31
Statistical analyses
Descriptive statistics were used to present data. Median scores for NRS for each session and the overall NRS from last session was calculated (primary outcome = feasibility). When compiling data from the migraine diaries, data from the first week before (pre-intervention phase) and after (follow-up phase) the MPS were used for the evaluation due to considerable missing data from other weeks. From the diaries number of days with mild-to-moderate migraine, severe migraine, any sort of headache, and days with mild-to-moderate and severe impact on DL were calculated. The median scores from answered questionnaires (HIT-6, PSS-14, MSQoL, PIPS, HAD) during the pre-intervention phase and the follow-up phase were calculated for each patient and each questionnaire. These median values were further used for descriptive and statistical analyses. Paired Wilcoxon signed ranks test was used to compare results from diaries and questionnaires before and after the intervention. Differences between those who completed the MPS and dropouts were explored with Chi-square tests (sex, education level, work status, duration of migraine) and the Mann-Whitney U-test (age). The significance level was set to p-values ≤0.05.
Results
Feasibility of the MPS
Demographics and description of the participants
Four MPS groups were consecutively included in this study from spring 2014 to fall 2015. A total of 30 patients were recruited. Less attendance than four sessions was considered as dropouts and six patients (20%) were therefore excluded from analyses. Thus, 24 patients (23 women) completed the MPS, see Figure 2. Common reasons for not attending sessions were ongoing migraine, not having enough energy to come, and not the time to come due to their family or work situation. One patient did not consider the intervention useful and stopped attending after the first session. The six patients who dropped out did not significantly differ regarding sex, age, education level, work status and duration of migraine (p-values > 0.05).
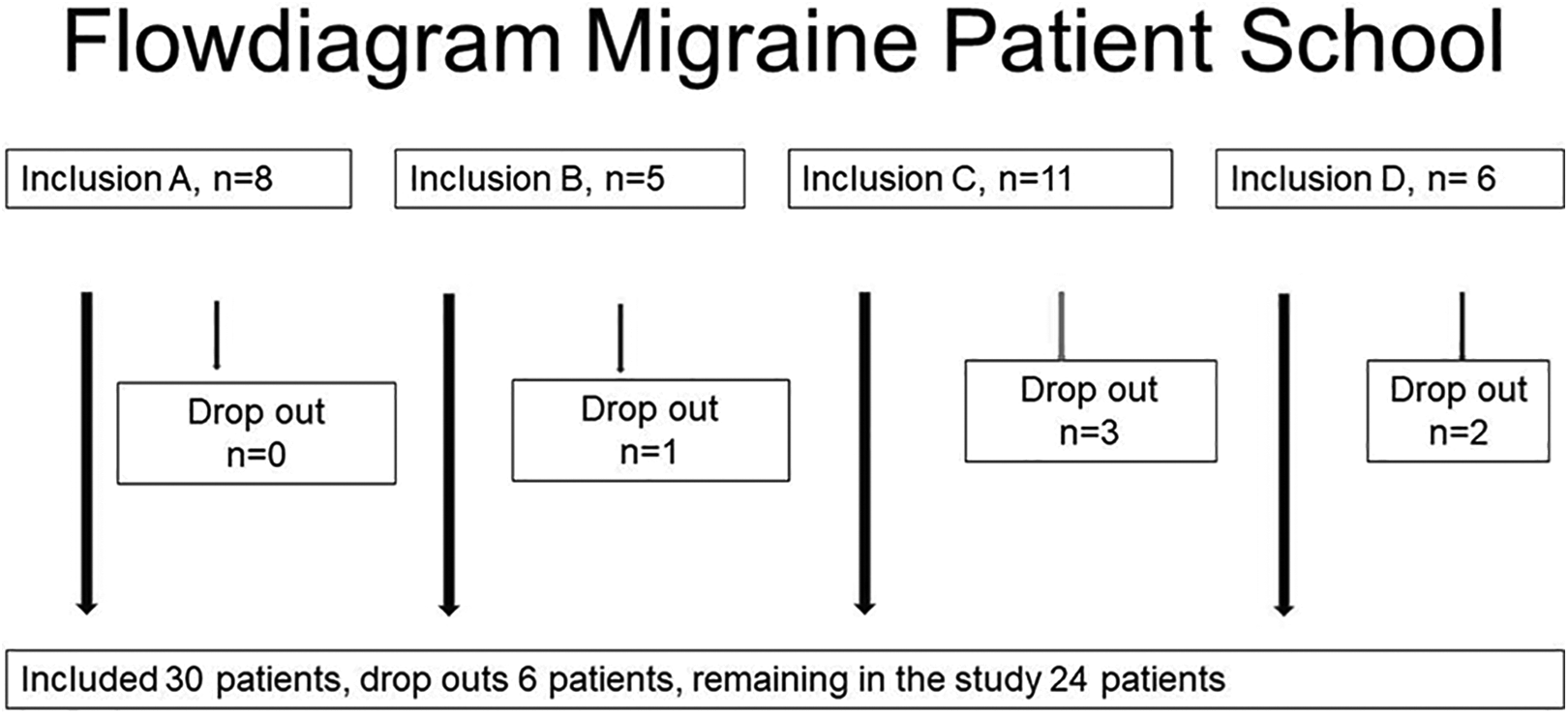
Flow diagram. Number of participants in each of the four groups with number of dropouts.
Baseline patient and migraine characteristics of the 24 who attended the MPS are presented in Table 1. Their median age was 42 years (range 28–59). Most participants were highly educated, and two-thirds were working at least part time. Many patients reported having sleep disturbances. No comorbidities were reported among half of the participants, one-third reported one comorbidity, and one-sixth several comorbidities. Eighteen of 24 (75%) had had migraine over 10 years and 20 (83%) patients fulfilled the criteria for chronic migraine at baseline. Almost all reported severe migraine attacks when it was impossible to continue working or performing other activities. Eleven patients reported use of painkillers daily or almost daily. Triptans alone or in combination with non-steroidal anti-inflammatory drugs (NSAIDs) or other analgesics was common. Only three participants (13%) used attack medication containing codeine. Most participants had tried several pharmacological prophylactics and a variety of different non-pharmacological treatments to handle their migraine situation.
Baseline characteristics of the 24 participants who completed the migraine patient school. Documentation performed during 1 week before and after the MPS intervention.

§Other include diabetes, cardiovascular-, rheumatic-, pulmonary- and gastrointestinal disorders.
#Chronic migraine. *n = 20. NSAID: non-steroidal anti-inflammatory drug
Five participants attended all seven sessions and five attended only four sessions, the remaining participated in five (n = 7) or six sessions (n = 7). Nineteen (79%) of the 24 participants attended most sessions and performed their home assignments. Results from evaluation of each previous session of the MPS are presented in Table 2. Median values of perceived experience and ability to complete home assignments ranged from 7 to 8, and between 8 and 9 for perceived ability to take part and understand the previous session, however there was a wide range of the scores (min-max). The median (min-max) values of perceived experience of the MPS (n = 17) were 7, 1,10 and 8 4,10 both for perceived ability to take part and understand the various components of the MPS and to complete the home assignments (n = 16).
Results from patients’ evaluations regarding their experience and understanding of the session’s theme and their ability to perform the home assignments.

Numeric rating scales (NRS) ranging from 0 (not at all rewarding/with great difficulties) to 10 (very rewarding/easily) were used. Number of evaluations varied since not all participants attended all sessions.
Migraine diaries:
Seventeen (71%) participants filled out a complete week (7days) before and after the group intervention. There were no statistically significant differences in number of days with migraine, days of any other type of headache or days with impact of DL (Table 3).
Descriptive and statistical results from migraine diaries before and after intervention, p-values are from paired Wilcoxon signed ranks tests.

DL: daily life.
Questionnaires:
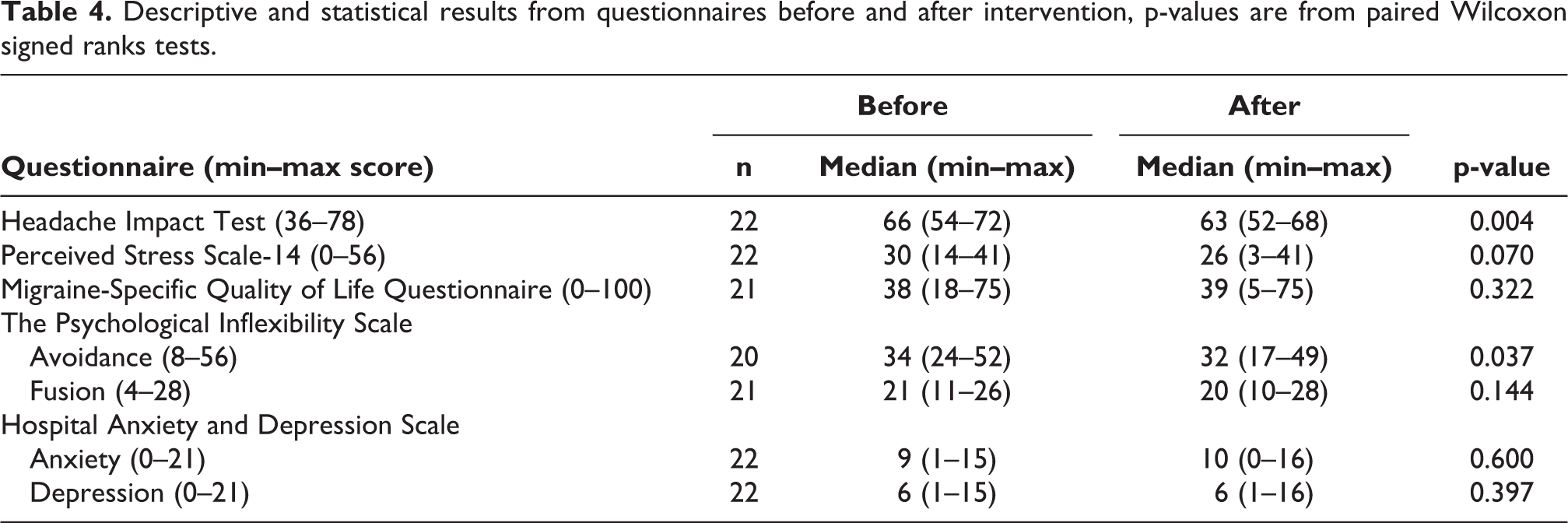
There were missing data from two to four patients depending on questionnaire. The results from the descriptive and statistical analyses from questionnaires are presented in Table 4 and Figure 3. A significant decrease was found for HIT-6 (p = 0.004). Although the decrease in PSS-14 scores was non-significant (p = 0.070), there was a tendency for reduced perceived stress. There was a significant reduction in the PIPS avoidance (PIPS-A) subscale (p = 0.04). The individual changes in the calculated median values from answered questionnaires (HIT-6, PSS-14, PIPS-A) during the pre-intervention phase and the follow-up phase are illustrated in Figure 3. The results from the HAD questionnaires showed that six patients had a possible anxiety disorder (HAD anxiety score ≥11) and four as possibly having depression (HAD depression score ≥11) both before and after intervention. Changes in classification for anxiety disorder were seen for two patients; one changed from no case to a probable case and the reversed for the other patient. The same was found for two other patients concerning depression.
Descriptive and statistical results from questionnaires before and after intervention, p-values are from paired Wilcoxon signed ranks tests.

Patients’ individual changes in median values from answered questionnaires before and after the migraine patient school (MPS) in (a) the Headache Impact Test (HIT-6), (b) Perceives Stress Scale (PSS-14), and (c) Psychological Inflexibility in Pain Scale Avoidance (PIPS-A).
Examples of some free comments from the participants on the evaluation forms: 1. More homogenous groups based on migraine severity and consequences of the disability. 2. More focus on how to live with severe migraine. 3. Discussions between group members most rewarding. 4. More practical training methods. 5. More mindfulness and discussions. 6. Training in group most rewarding.
Discussion
The MPS had the focus of initiating behavioral changes with the purpose of decreasing the burden of headache and increasing QoL. All participants had previously been diagnosed having chronic migraine and most of them also had regular drug intake of attack medications, thus many also fulfilled a diagnosis of medication overuse headache. Most of them fulfilled also the criteria for tension-type headache. This study showed that the multimodal educational and behavioral group intervention, MPS, was feasible for patients with severe (high-frequency or chronic) migraine to attend to, to take part in the group discussion at the sessions and to understand the various components. The participants found the home assignments possible to perform and reported that they could benefit from these combined techniques.
A previous study performed on episodic, low-frequency, migraine patients with the same written study material but using internet as a behavioral modification therapy tool reported reduction in drug intake by 22% and 27% fewer migraine days. 12,16 After our MPS, however, there was no reduction in number of migraines, possibly due to too few patients, too short observation period and probably due to low compliance of filling out the diaries. The content in MPS used the same text-based program as in the previous Internet study. The MPS had a greater focus on physical activity and body awareness. The open evaluation questions in the MPS study showed that the participants appreciated the physical encounter with people with the same type of migraine as themselves and that it was valuable to feel that you were not alone in suffering from such severe migraine. Meeting face-to-face was something that the participants in the previous Internet study requested and the opportunity to be able to chat via the Internet with each other. What also differs was that the Internet study had more participants and a longer intervention time, the total time for the intervention groups was 11 months and the control group 8 months, respectively. The Internet diary was designed in such a way that one could not skip dates, which probably contributed to better compliance.
Significant improvements were found in both HIT-6 and PIPS-A indicating a reduced impact of headache on life and a reduced tendency to withdraw from planned and valued activities and social participation because of pain after the MPS. We acknowledge, however, that without a control or reference group the results must be interpreted with caution.
The content of the MPS was found rewarding by most participants, but there is a need to elucidate which theoretical parts and home assignments that should be adjusted to further improve future programs. The overall ratings of experience, understanding and ability to perform home assignments indicated that the MPS was of importance for this patient category. It was obvious that the participants had different expectations attending the headache school, depending on individual expectations/prior rehabilitation experiences and life situation. This was seen for all different themes to various extent. However, the wide range in NRS ratings from evaluations of the MPS program as well as in scores from questionnaires between individuals also suggest different pre-MPS experiences and knowledge. Thus, a pre-screening before inclusion or an individualized selection of sessions for patients to participate in rather than the whole program might further improve the MPS. Our opinion after performing this study is that information on the willingness of the participants to work with change of behavior is of importance for the outcome. Small groups give all participants the possibility to take active part in the discussions. The possibility to receive the theoretical material and home assignment through post or email, probably reduced the number of dropouts. Despite this, we believe that the evaluation of our MPS program was defaulted by these dropouts. The frequency was however in the same magnitude as reported in the CHESS trials. 32,33 In the future, we speculate that a combination of in-real-life participation to be able to take part in the discussions is important. We see great opportunities to develop a more tailored program for patients with the severest migraine. With the Internet as a tool and a meeting place for conversations via video and chat, will probably be a complement to but not as a substitute for face-to-face meetings. Working in small groups, meeting fellow patients, and learning from each other was of great importance for the participants in MPS, which is also in line with the result from the CHESS trials. 32,33 We agree with McLean and co-workers 34 that future MPS must be even more patient centered and we will therefore focus on further analyzing the individually presented free comments from our MPS in a coming report reporting structured group interviews.
We found the MPS program to be feasible from the patient perspective regarding participation and beneficial effects by judging from their evaluations. It worked well to send out the study material by post/mail to patients who could not attend a meeting due to migraine attacks, so that they could catch up before the next session. However, some adjustments of the study material are needed to better fit participants’ needs and level of knowledge. The training sessions with BBAT and AR exercises were much appreciated and judged to be of great importance. A lesson learned is to minimize both the number of questionnaires and evaluation occasions to not tire out these severely affected patients.
Conclusions
Our patient school with a multimodal educational and behavioral group intervention program was feasible to perform among patients with severe migraine, where most of them reported positive effects from this combined theoretical and especially the behavioral group training program.
Article highlights
Our 13 weeks of multimodal group intervention (MPS) with theoretical education and training in body awareness (BBAT) and applied relaxation (AR) was feasible to perform and had positive effects among patients with severe migraine.
A significant reduced impact of headache on life was observed (Headache Impact Test, p = 0.004).
A significant reduced withdrawal from activities and social participation because of pain was observed (Psychological Inflexibility in Pain Scale Avoidance p = 0.040).
Supplemental material
Supplemental Material, sj-pdf-1-rep-10.1177_25158163211020447 - A pilot study of the feasibility of a Swedish multimodal group intervention for severe migraine—The migraine patient school
Supplemental Material, sj-pdf-1-rep-10.1177_25158163211020447 for A pilot study of the feasibility of a Swedish multimodal group intervention for severe migraine—The migraine patient school by Birgitta Helmerson, Anna Sundholm, Kerstin Hedborg, Elisabet Waldenlind, Marie Kierkegaard and A Ingela M Nilsson Remahl in Cephalalgia Reports
Footnotes
Authors’ note
STROBE checklist of items that should be included in reports of cohort (longitudinal, intervention) studies.
Acknowledgements
We want to thank the participating patients.The specialized headache nurses A Halmearo, M Berg and E Forsberg who together with E-C Jacobson and V Hybrink organized the different MPS sessions.
Author contributions
Birgitta Helmerson, Anna Sundholm and Kerstin Hedborg: Designing the study, acquisition of data, analysis and interpreting of data. Elisabet Waldenlind: Statistical analyses, Interpreting of data, critical revision of manuscript for intellectual content, manuscript writing. Marie Kierkegaard: Designing the study, analysis and interpreting of data, statistical analyses, critical revision of manuscript for intellectual content, manuscript writing. A Ingela M Nilsson Remahl: Designing the study, analysis and interpreting of data, critical revision of manuscript for intellectual content, manuscript writing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the ethical review board in Stockholm, registration number Dnr 2013/2025-31/1 and procedures were conducted in accordance with the Declaration of Helsinki.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received scholarship from Swedish Headache Society and Karolinska University Hospital.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.