
Abstract
Background:
The results of high-frequency repetitive transcranial magnetic stimulation (rTMS) over the dorsolateral prefrontal cortex for migraine have been inconsistent. However, high-frequency rTMS over the motor cortex is a treatment that may be effective in relieving symptoms of migraine with a low risk of side effects.
Methods:
A systematic review of high-frequency rTMS over the brain motor cortex areas in human participants was conducted to assess efficacy in treating migraine. Articles that were not looking at migraine patients, stimulation over the left motor cortex, or were not in English were excluded. Nine articles representing eight experiments using high-frequency rTMS over the motor cortex areas for migraine in human participants were extracted from the databases of PubMed, PsycINFO, MedLine, CINAHL, and BioMed Central.
Results:
Two-hundred and seven of 213 patients completed treatment throughout all the studies examined. High-frequency rTMS over the motor cortex areas for migraine improved migraine frequency in seven of eight studies. Two of the eight studies were randomized controlled trials at low risk for biases and found high-frequency rTMS over the motor cortex areas effective in improving migraine frequency and severity. Other details of treatment prescription and symptoms were also examined.
Conclusion:
High-frequency rTMS over the motor cortex areas for migraine demonstrated efficacy as a migraine treatment, had minimal side effects, and should be further investigated.
Introduction
Migraines are a public health problem, with stark economic implications. Direct and indirect health-care costs for migraines are approximately US$14 billion annually 1 and US$36 billion in total cost when including the estimated 113 million lost workdays annually due to migraines. 2 Migraine attacks influence the sufferer in copious ways, including an individual’s educational and employment decisions, social lives, and family relations, due to anxiety of an expected attack, or fearing commitment due to a fear of unpredictable attacks. 3 –7 Even between migraine episodes, migraine sufferers have demonstrated to have greater emotional distress, disturbed contentedness, and decreased vitality and sleep compared to healthy nonmigraine sufferers. 8 These episodes occur with an amalgamation of symptoms that include throbbing pain, light and sound sensitivity, nausea, vomiting, and sometimes auras. 9 –11 Migraines affect 15–20% of the population (38 million Americans) and are three times more prevalent in women (18%) than in men (6%) in the United States and Europe, 1,11,12 making advancement in treatment imperative.
Preventive and abortive/acute migraine pharmaceutical treatments may have modest to good efficacy in relieving attacks in some patients, but many of the most commonly prescribed preventive and acute treatments have adverse effects that are contraindicated for individuals with cardiovascular issues, 13 –15 kidney issues, 16 –19 pregnancy, 15,20 –22 or individuals at risk of overuse, addiction, and an episodic migraine becoming chronic. 21 –28 Additionally, adverse effects of prescribed pharmaceuticals for migraine may impair the patient from being able to work or engage in social activities 21,29,30 decreasing the overall quality of life. A possible novel treatment method that has less severe side effects than commonly prescribed drugs for migraine treatment is repetitive transcranial magnetic stimulation (rTMS). 31
rTMS has demonstrated efficacy in treating illnesses that have shared pathology and are often comorbid with migraine, including depression 11,32 –37 and epilepsy. 38 –40 Previous findings on rTMS as a therapy for migraine have been inconsistent partly due to no standard prescriptions regarding area of stimulation, Hz, amount of pulses, intensity, and sessions needed to achieve reliable outcomes. Low-frequency rTMS (1–5 Hz) 41 and high-frequency rTMS (10-20 Hz) 41 over the dorsolateral prefrontal cortex consistently have not demonstrated effective outcomes 42 and have not performed better than sham treatments. 42 –44 However, there have been promising results for direct current stimulation in the primary motor cortex for several pain conditions, 45,46 including migraine, 47 and researchers have suggested the motor cortex may be a more promising area of stimulation for migraine sufferers. 42 Therefore, this systematic review focused on rTMS over the motor cortex areas and was performed examining high-frequency rTMS over the motor cortex areas of the brain in individuals suffering from migraine, and whether it was an effective treatment for migraine prevention.
Methods
Search strategy
This systematic review of the literature examined the effectiveness of preventing migraine with high-frequency rTMS (10 Hz or higher) over the motor cortex areas in human participants who suffer from migraine. The primary measures being examined were treatment efficacy in improving migraine frequency and severity. No limits were set for when studies were completed since rTMS has only been recently used as a treatment for migraine in research. Studies examined were only those that were published. Search terms for the review included “repetitive transcranial magnetic stimulation” or “rTMS” combined with “migraine”. This review examined research in PubMed, PsycINFO, MedLine, CINAHL, BioMed Central, and reference lists of identified articles (see Figure 1 for study selection flow chart). Date of last searches for all databases was May 22, 2019.

Study selection details. Studies were identified using five separate database searches: PubMed, PsycINFO, Medline, CINAHL, and biomed central.
Exclusion criteria
Studies excluded from this review were any that are not specifically looking at migraine prevention using high-frequency rTMS over the motor cortex areas in patients that suffer from migraine, not in English, and/or primarily examining conditions comorbid with migraine.
Data extraction
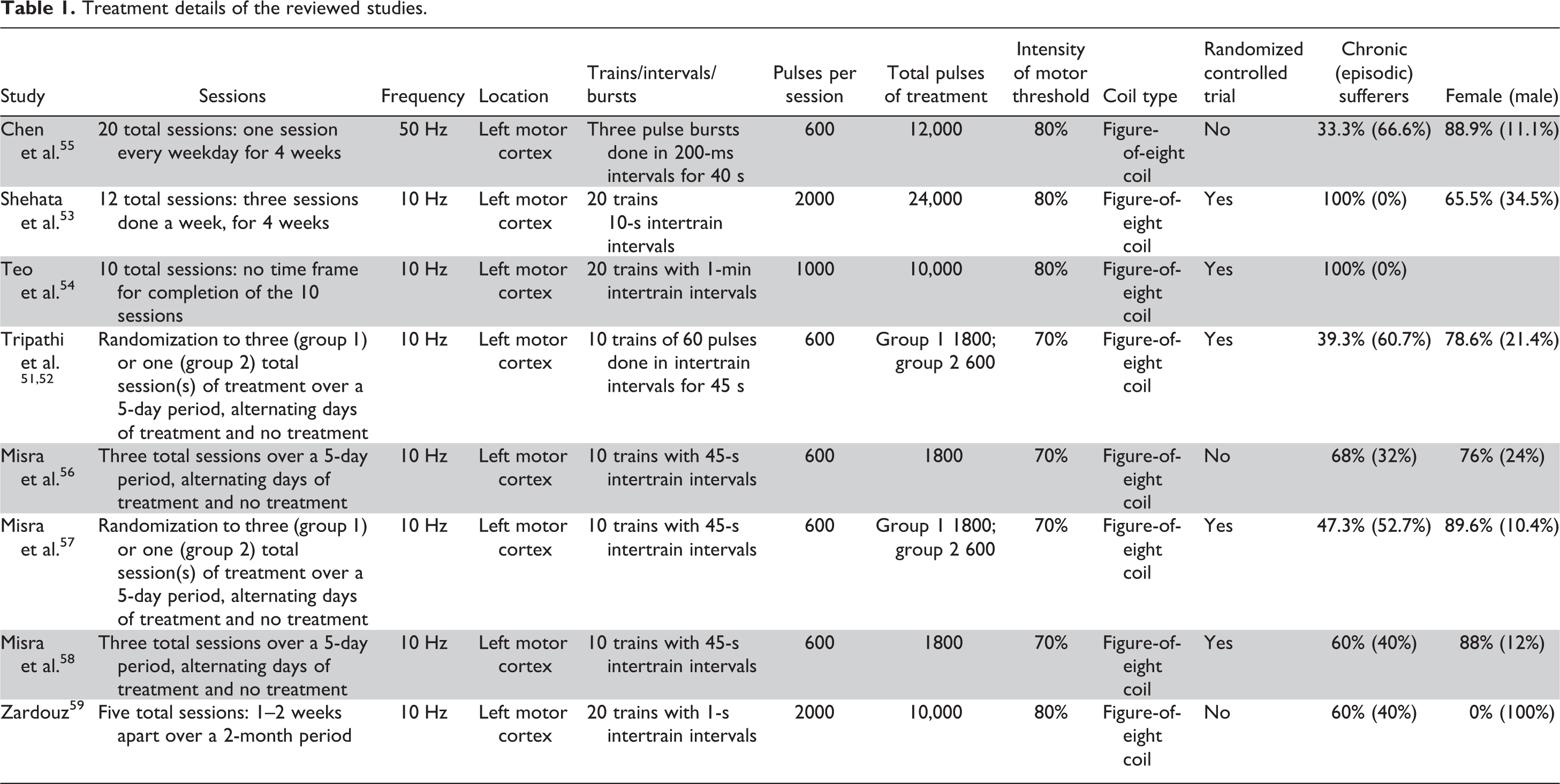
For each study, the following information was extracted: authors’ names; publication year; study design; number of participants; gender and age of participants; rTMS intensity, frequency, and duration of exposure; and measures of migraine frequency, pain intensity, and other measures (see Table 1).
Treatment details of the reviewed studies.
Quality assessment
Results of studies can be undermined by flaws in design, conduct, analyses, and reporting that cause biases; leading to systematic errors that could influence variability in findings and lead to underestimating or overestimating the true intervention effect. 48 To assess the risk of bias for the studies reviewed, this review used the Cochrane Collaboration’s tool for assessing risk of bias, which assigns risk as low risk, high risk, and unclear risk to six bias domains. 49 Higgins and colleagues 49 noted that this tool makes the process more accurate as a methodological quality evaluation tool by separating judgment about risks of bias from description of the support for that judgment using a series of items encompassing several domains of bias. The six bias domains include selection bias, performance bias, detection bias, attrition bias, reporting bias, and other biases. 50 Selection bias examined the similarities and differences of baseline characteristics among participants in a study. If randomization was accomplished successfully, it prevented selection bias in sequencing of participants to specific interventions. Concealing intervention assignment by eliminating the researchers’ knowledge of forthcoming allocation of participants was also examined in selection bias. 50 Performance bias examined the systematic differences between interventions or the exposure to factors other than the intervention’s intended treatment. 50 Studies were assessed on performance bias by assessing if the study was single-blind. How detection bias was assessed examined if the study was double-blind. 50 Attrition bias was the systematic difference between participant withdrawals between groups. For example, if one group had greater attrition than another, this could lead to biases in the resulted outcomes from the groups. Reporting bias was systematic differences between reported and unreported findings. Other biases were biases that did not fit into the categories of selection, performance, detection, attrition, or reporting bias, such as medication use of participants during studies that were not a part of the experimental treatment. 50
Results
Results from all searches yielded 7958 articles, 9 of which were identified for final review and were relevant to the aim of examining the effectiveness of rTMS over the motor cortex areas in individuals suffering from migraine (see Figure 1). Two of the nine studies, Tripathi et al., 51,52 were combined in the analysis as one study, because they shared the same sample but were separate publications that reported on different biomarker outcomes. Of the eight studies, five were randomized controlled trials. The studies were described based on treatment demographics, treatment prescriptions, treatment tolerance, treatment effectiveness, study quality, and other treatment findings.
Treatment demographics
In general, most of the studies had female-dominated samples of individuals who suffered from four or more migraines a month. Most studies looked at episodic and chronic sufferers and generally had a very small sample of migraine sufferers that experienced aura. Two studies looked at chronic migraine sufferers only. 53,54 Six of the eight studies examined episodic and chronic sufferers. 51,52,55 –59 One study looked at males only. 59 Even though reports of migraine with aura were included in several studies, the number of experiencers was few, with very small sample sizes, and was not examined exclusively in any studies. Additionally, the settings for stimulation used in the studies varied.
Area of stimulation, frequency, intensity, and coil types
All eight of the studies stimulated the left motor cortex. Seven of the eight studies stimulated the left motor cortex at a 10 Hz in repetitive trains and one of the eight looked at the stimulation of the left motor cortex at 50 Hz in bursts. All studies used 70% or 80% of motor threshold for intensity with a figure-of-eight coil (see Table 1). Stimulation settings did not vary much overall, but sessions and amount of pulses did.
Number of sessions and pulses
Number of sessions of rTMS varied greatly in the studies, with the lowest being 1 session 51,52,57 to the highest being 12 sessions. 53 Pulses per session varied greatly as well, with many studies looking at the lowest amount of 600 per session 51,52,55 –58 and a couple studies using the highest amount reviewed at 2000 per session. 53,59 Total number of pulses over the entire treatment regimen ranged from 600 51,52,57 at the lowest to 24,000 53 at the highest (see Table 1). The amount of sessions and pulses did not seem to influence treatment tolerance, but the stimulation intensity and demographics of the migraine sufferer may have.
Treatment tolerance
Overall high-frequency rTMS over the left motor cortex was well tolerated with 207 of 213 total participants completing the treatment regimen in all the studies. The two studies that examined chronic sufferers exclusively were also the only two studies that were rated high risk in attrition bias. Shehata and colleagues reported a 14.29% attrition rate (n = 2) due to side effects of headaches worsening in their treatment group, 53 and Teo and colleagues reported a 50% attrition rate (n = 3) due to increased headaches of discomfort in their treatment group. 54 Both studies used 80% of resting motor threshold intensity. The majority of studies that used a 70% resting motor threshold intensity with chronic sufferers had a zero attrition rate and included a study by Tripathi et al. 51,52 and two studies by Misra and colleagues. 56,57 Additionally, Misra et al. 58 used a 70% resting motor threshold intensity and had just a 2% attrition rate (n = 1) due to side effects, with no other side effects reported from the other 47 participants completing treatment. 58 However, Chen and colleagues and Zardouz et al. used 80% motor threshold and had zero attrition rates, and both included chronic migraine sufferers in their samples. 55,59 Overall, it appeared that intensity of 80% of resting motor threshold was well tolerated by episodic migraine sufferers but may have been difficult for some chronic migraine sufferers to tolerate. However, an intensity of 70% of resting motor threshold seemed to be well tolerated by chronic and episodic sufferers.
Treatment effectiveness
Seven of the eight studies found high-frequency rTMS to reduce migraine frequency 51 –53,55 –59 and six of eight found a reduction in migraine severity/intensity 51 –53,56 –59 in a 1-month follow-up after treatment. Only one of the eight studies examined high-frequency rTMS effectiveness beyond 1 month after treatment 53 and found that 12 sessions of 2000 pulses at 10 Hz of rTMS over the left motor cortex at 80% of motor threshold intensity, 3 days a week for 4 weeks had treatment effects that existed up to 8 weeks after treatment and then began to wane at the 10- and 12-week follow-up evaluations.
Overall, rTMS appeared to be effective in reducing migraine frequency after just one treatment of 600 pulses at 70% of motor threshold intensity. 51,52,57 No conclusions regarding optimal number of sessions and pulses could be made from reviewing the results, but it appeared that at least three sessions of treatment consisting of 600 pulses at 70% of motor threshold intensity over the left motor cortex in a 5-day span had a greater effect on improving migraine frequency and intensity 1 month after treatment when compared to just one session at the same settings. 51,57 In regard to sustained effects, 12 sessions of 2000 pulses at 10 Hz of rTMS over the left motor cortex at an 80% of motor threshold intensity, 3 days a week for 4 weeks reduced migraine frequency and severity, and improved quality of life that lasted over 2 months in duration. 53 Chen and colleagues’s 55 study was the only study that examined rTMS using 50 Hz administered in three pulse bursts rather than a 10 Hz frequency in trains. The 50 Hz three pulse bursts of 600 pulses per session for 5 days a week for 4 weeks yielded significant reductions in migraine frequency, abortive medication use, and depression, warranting further instigation of not only the more popular 10 Hz over the left motor cortex in repeated trains method but methods with different frequency levels and burst methods of stimulation. Only one study of the eight did not find improvements in migraine symptoms following rTMS, 54 but the study had high attrition (50% in the treatment group), and, as mentioned earlier, only examined a small treatment sample (n = 6) that were all chronic migraine sufferers treated at an intensity of 80% of resting motor threshold. To further interpret these findings, each study’s risk of bias was evaluated.
Low risk of bias studies
Two of the eight studies were of lower risk than the rest. Misra and colleagues study was considered the low risk of bias with having unclear risk in selection and other biases; low risk in performance, attrition, and reporting biases; and only having high risk in detection bias. 57 The other low-risk study was Misra et al., which had low risk for all bias domains 58 (see Figure 2). Both trials had promising results for rTMS as an effective treatment for migraine sufferers, warranting further investigation into the treatment. In addition to improvements in migraine frequency and severity, a variety of other measures were observed to improve in migraine sufferers after high-frequency rTMS treatment over the left motor cortex.

Other findings
Some studies examined measures outside the scope of migraine frequency and severity. Visual analog scale was one of the few variables with mix results, with improved scores in patients who received rTMS in Tripathi et al.’s study. 51,52 Visual analog scale scores were not improved in Misra and colleagues’ two studies. 56,57 Other variables that were found to improve after high-frequency rTMS included migraine duration, 56,58,59 migraine index, 51,52 functional impairment/disability, 56 –58 headache disability, 53 rescue medication use, 55,56,58 quality of life, 53 depression, 55 plasma beta-endorphins levels in chronic sufferers, 56 plasma beta-endorphins level in episodic and chronic sufferers, 57 µ opioid receptors, 57 glutamate and NR2B receptors, 51 glutathione, and total antioxidant activity. 52 Teo and colleagues’ study was the only study to find no difference in the measures of migraine duration, headache index, and analgesics used after rTMS treatment. 54 Anxiety measured in Chen and colleagues’ study was not improved post-rTMS treatment. 55 Biomarkers that were not improved after rTMS included beta-endorphins levels in episodic sufferers in Mirsa and colleagues’ study, 56 δ opioid receptor, 57 and mGluR3 receptors. 51 Other interesting findings were high-frequency rTMS being directly compared to prophylactic medication. Shehata and colleagues compared high-frequency rTMS over the left motor cortex to botulinum toxin-A. The two treatments did not significantly differ from each other in improving migraine frequency and headache severity after 2 months; but at week 10, follow-up evaluation rTMS treatment started to wane in effectiveness, and botulinum toxin-A continued to be consistent in effectiveness. 53 Tripathi et al. compared rTMS over the left motor cortex to the prophylactic antidepressant drug Amitriptyline. Patients who received three sessions of rTMS saw greater improvement in migraine frequency, intensity, and migraine index scores than those taking Amitriptyline 1 month after treatment. 51,52 Many of the reviewed studies used the same response rate standards that are also used in pharmaceutical trials for prophylactic medication (50% reduction in migraine frequency), 21 as displayed in Table 2.
Reported response rates of at least a 50% reduction in migraine symptoms unless otherwise noted.a

a rTMS: repetitive transcranial magnetic stimulation. A “—” indicates the condition that did not exist in the study, or the study did not record or report a measure of a 50% or greater reduction for a migraine symptom.
In regards to comparing treatment effectiveness for episodic and chronic sufferers, no distinction in improvements was noted except in two studies. Mirsa et al. 58 noted that a greater percentage of chronic migraine sufferers reported improvement in migraine frequency (90.2%) and severity (85.2%) compared to episodic sufferers (60% and 65.5%, respectively) 1 month after treatment. The Mirsa and colleagues’ (2013) study demonstrated chronic migraine sufferers had a significant increase in beta-endorphin levels from baseline measures after treatment, while the same effect was not found in episodic sufferers. The evidence for repetitive high-frequency rTMS over the motor cortex having greater improvement in chronic migraine sufferers compared to episodic is sparse but should be further investigated with the limited support found in the aforementioned studies.
Discussion
The findings of this systematic review supported the use of high-frequency rTMS as an effective treatment for individuals suffering from episodic and chronic migraines and demonstrated that it was well tolerated; with seven of eight studies finding improvements in migraine frequency after treatment 51 –53,55 –59 and six of eight finding improvement in migraine severity. 51 –53,56 –59
High-frequency rTMS over the left motor cortex could be a promising area of stimulation, with evidence of treatment conditions performing better than sham conditions in headache frequency or severity in three of the four studies reviewed that contained sham conditions. 51,52,57,58 Teo and colleagues’ study was the only study with a sham condition that did not report a difference between treatment and sham conditions, but no descriptive statistics for the study were reported, and each condition only had three participants that completed the study. 54 The results of high-frequency rTMS over the motor cortex compared to sham were more favorable than the findings previously reported in which patients treated with high-frequency rTMS over the left dorsolateral prefrontal cortex experienced notable difficulties in responding to treatment and performed the same or worse than sham conditions (e.g. the studies by Conforto et al. 42 and Granato et al. 43 ).
The literature reviewed provided substantial evidence of the potential of high-frequency rTMS over the left motor cortex to reduce the number and severity of migraine attacks. The findings were upheld even under conditions of greater methodological rigor and generalized to other relevant outcomes. The two randomized controlled studies in this review with the lowest risk of bias found evidence for high-frequency rTMS over the motor cortex as an effective treatment in episodic and chronic migraine sufferers. 57,58 The findings held not only for improvements in subjective measures of migraine symptomatology (depression, quality of life, severity, etc.) but also for objective biomarkers. 51,52,56,57 This coincided with past research showing that high-frequency rTMS over the motor cortex induced neurological changes in the short-term 60,61 and had the potential to encourage long-term changes in the brain as mentioned by other researchers. 62 –64
In terms of the prescription required to induce the changes, it appeared that as little as three sessions of treatment in a 5-day span were effective in producing a significant improvement in migraine frequency, severity, migraine index, migraine duration, functional impairment, beta-endorphin levels, glutamate and NR2B receptors, glutathione, and total antioxidant levels 1 month after treatment 51,52,56,57 (see Table 1). Also, three sessions of treatment were demonstrated to be superior to one session for some migraine outcomes, such as migraine frequency, migraine intensity, and migraine index. 51,57 Unfortunately, only two studies examined outcomes beyond 4 weeks (see Table 3). Shehata and colleagues found improvements in headache frequency, headache severity, and quality of life at 8 weeks compared to baseline; however, the effects started to wane by 12 weeks after treatment. 53 Teo and colleagues found no improvement in migraine frequency or duration between true treatment and sham at 4 or 8 weeks after treatment, though sample sizes of each group were small (n = 3 in both groups). 54 Future research should include longitudinal research designs to determine the optimal prescriptions of high-frequency rTMS treatment over the left motor cortex in migraine sufferers to induce longer term changes in neuroplasticity and improvements in outcomes.
Studies details.

rTMS: repetitive transcranial magnetic stimulation.
While there appeared to be minimal adverse effects associated with high-frequency rTMS over the motor cortex, chronic migraine sufferers seemed to have a difficult time handling treatment at an intensity of 80% of motor threshold potential, as high dropout rates from discomfort (14.29%; 50%) were seen in chronic sufferers in the Shehata and colleagues’ and Teo and colleagues’ studies, though the sample of patients that dropped out were small (n = 2; n = 3). 53,54 The theta burst form of high-frequency rTMS done in Chen and colleagues’ study (see Table 1) also warrants further investigation, because their promising results were achieved at an 80% motor threshold intensity in chronic or episodic sufferers, but there was no attrition. 55 Therefore, future research should replicate these findings to determine whether the theta bursts are better tolerated by chronic migraine sufferers. A high rate of participants treated with high-frequency rTMS over the left motor cortex tolerated the treatment (97.18%; 207 of 213 participants) in comparison to 67% (1647 of 2444 surveyed participants) of migraine sufferers delaying or avoiding taking pharmaceutical medication due to side effects. 29 Therefore, it seemed advantageous as a primary treatment.
As in all studies, limitations existed in the studies reviewed. The small number of studies of high-frequency rTMS over the motor cortex (eight total studies), and only five randomized controlled trials (see Table 1), meant that there were still many voids regarding the optimal prescription to be administered in episodic and chronic sufferers, including Hz, intensity, pulses, and pattern of how pulses are administered, and medication interaction with the treatment. In terms of methodological issues, one of the most prominent limitations in the literature was a lack of recording differences of individuals who were taking migraine prophylactic medication and individuals who were not during high-frequency rTMS treatment. This limitation existed in six of the eight studies, 51,52,54 –57,59 which may have affected treatment outcomes. This was the most common reason studies were rated as unclear risk in other biases. No studies that were reviewed examined if prophylactic migraine medication had a possible synergistic effect or prevented the effectiveness of high-frequency rTMS therapy over the motor cortex areas. In fact, very little research has been done on the possible effects of migraine prophylactic medication on any other migraine therapies, with most the focus of prophylactic treatment being on how it reduces the use of abortive medications such as in Yaldo and colleagues’ study. 65 A study conducted by Almaraz et al. found that prophylactic medications did not have an effect on the efficacy of low-frequency single-pulse transcranial magnetic stimulation (TMS) over the occipital lobe as an acute treatment for migraine sufferers with migraine aura. 66 However, it was difficult to extrapolate these results, because the technique of TMS (single pulse over the occipital lobe and low versus high frequency) and focus (for acute treatment) were different than the studies examined in this review. It also should be noted that some prophylactic migraine treatment has been found to reduce blood plasma glutamate levels in migraine sufferers, 67 which could indicate an influence of neurochemistry that could possibly influence rTMS treatment. Also, six of the eight studies did not make the distinction between chronic sufferers and sufferers that were chronic due to medication overuse, 51,52,55 –59 why two studies removed patients who were chronic sufferers due to medication overuse 53,54 which may have influenced the studies. Further, other prophylactic treatment such as beta-blockers 21 angiotensin-converting enzyme inhibitors, 68,69 or less-invasive nutraceuticals such as magnesium, 70,71 CoQ10, 72,73 and riboflavin 74 should be examined in the future research for possible synergistic effects with high-frequency rTMS over the motor cortex.
In regards to the context of biases for the randomized controlled trials, only two of the five described their randomization process of participants clearly and had low risk of selection bias. 53,58 All other randomized control trials were unclear or at high risk for selection bias for not describing the randomization process or had significant differences on pretest measures among groups. Reporting bias was only an issue for two of the eight studies, and both were randomized controlled trials. 51,52,54 Tripathi et al. failed to report statistical comparisons of measures between all groups in their study, which made it difficult to distinguish if one method of treatment was superior to another. 51,52 Teo and colleagues failed to report any descriptive statistics of any measures and reported no statistical tests. 54 Some studies reviewed had low sample sizes that received treatment, such as Shehata and colleagues (n = 14), Teo and colleagues (n = 6), Chen and colleagues (N = 9), and Zardouz and colleagues (N = 5), which may have influenced results (see Table 3). 53 –55,59
With only eight studies that fit the search criteria (Tripathi et al., two articles counting as one study) for this systematic review and only five of those consisting of randomized controlled studies, the research on high-frequency rTMS over the left motor cortex as a treatment for migraine is in its early stages and has been mostly exploratory to this point. Future directions of research should consider examining effects longer than 1 month after treatment; examining effects of rTMS on more biomarkers associated with migraines such as serotonin 21,75 and inflammatory markers 76 –80 and comparing rTMS prescriptions to find the most appropriate for chronic and episodic sufferers and those with and without auras.
Also, the present research lacks any data on whether high-frequency rTMS affects migraine sufferers with aura any differently than those without aura. This is a common theme in migraine therapy research with the overwhelming majority of studies looking at a mixed population of migraine sufferers with and without aura. 81 Outcome measurements regarding the migraine aura are commonly not taken, with the focus being generally on the migraine attacks with pain. 82 Research done by Conte and colleagues demonstrated that individuals who experience migraine aura may have a greater abnormality in being more sensitive with glutamate-dependent short-term primary motor cortex cortical potentiation patterns than migraine sufferers without aura. 83 This would influence the necessary intensity that may be prescribed for rTMS therapy, as intensity is set based on resting motor threshold potential.
Other neurostimulation techniques also may be viable treatment methods for migraine and should be further examined. Single-pulse TMS over the occipital cortex has demonstrated effectiveness as a noninvasive abortive treatment for migraine, 84,85 but recent research has found a decent response rate (46%) as a prophylactic treatment. 86 Transcranial direct stimulation over the primary motor cortex has been supported in improving migraine length and intensity, 47 while transcranial direct stimulation of the visual cortex has been supported to improve migraine attack frequency, migraine days, attack duration, and abortive medication intake in individuals suffering from migraine without aura. 87 Transcutaneous supraorbital nerve stimulation has been studied as a preventative treatment for migraine, with the treatment of 20 min a day for 3 months reducing mean number of migraine days. 88 It is hypothesized that transcutaneous electrical stimulation of supraorbital peripheral nerves is beneficial as a treatment of migraine via inhibition of nociceptive transmission in small pain transmitting fibers, since theses fibers modulate nociceptive activity in the trigeminal ganglion. 89 For a more invasive nerve stimulation treatment, implanted occipital nerve stimulators also have some demonstrated efficacy. It is thought that occipital nerve stimulation of large sensory afferents is likely to have a pain-reducing effect through inhibiting nociceptive activity in small c-fiber and a-delta fibers. 89 Studies have supported implanted occipital nerve stimulation improving headache days, disability, quality of life, and pain intensity. 90 –92 The research into neurostimualtion as a preventative treatment is promising with all techniques warranting further investigation and are plausible candidates for systematic reviews.
The explanation for efficacy of high-frequency rTMS over the motor cortex could be due to a few mechanisms. A review by Saavedra et al. suggests that the primary motor cortex is a major modulator of pain with baseline activity reflects strong feedback with pain associated neural areas. The primary motor cortex contains an array of connections to the sensory relay nuclei in the thalamus, in addition to efferent and afferent fibers in the spinal cord that controls the signals of painful stimuli and modulation of motor response to aversive contact. 93 More recent studies have found that baseline characteristics of the primary motor cortex are altered in patients suffering from fibromyalgia, and activity of the primary motor cortex in response to pain is significantly increased. 94 Direct current stimulation in the primary cortex demonstrated to induce changes in pain conditions such as fibromyalgia, 45 neuropathy, 46 and pain intensity and durations of a migraine. 47 Further, research from Fregni et al. demonstrated maladaptive plasticity of the primary motor cortex in chronic pain patients and that rTMS over the primary motor cortex in human participants does induce analgesic properties. 95 Several of the studies reviewed in this article demonstrated neurochemical changes in human participants from high-frequency rTMS over the motor cortex that included improvements in plasma beta-endorphin levels, 56,57 µ opioid receptors, 57 glutamate levels, 51 NR2B receptors, 51 glutathione levels, 52 and total antioxidant activity, 52 giving further insight into high-frequency rTMS over the motor cortex mechanisms of action.
Overall, the early results of high-frequency rTMS over the left motor cortex as a treatment for migraine sufferers are promising, and with further investigation, it may be considered a line of treatment with a lower side effect profile and higher tolerance than most current treatment methods.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.