
Abstract
Background:
The sphenopalatine ganglion (SPG) is a target for several headache syndromes. Most of the groups targeting the SPG do not localize it directly, and this might account for some therapeutic failures. As the SPG cannot be seen on computerized tomography (CT) scans, magnetic resonance image (MRI) must be used to visualize the ganglion. It would be advantageous to be able to predict the location of the SPG on CT scans for those using fluoroscopy or CT-guided injections and for those in whom MRI is not accessible or contraindicated.
Methods:
We localized the SPG in 21 Caucasian patients (21 right and 17 left ganglia; total 38) in 3 tesla MR images subsequently fused with CT scans. We measured the distance from the SPG to two bony landmarks identified on CT scans. We then applied the average distances to find an estimated position of the SPG. The first landmark was the center of the anterior opening of the vidian canal (VC). The second landmark was a point on the sphenoidal bone, defined in an axial plane at the level of the center of the VC (S-point). The predicted position of the SPG measured from the VC and the sphenoidal bone were referred to as, respectively, vcSPG and sSPG. Finally, the distances between the SPG, as seen on MRI, and predicted vcSPG/sSPG were calculated.
Results:
The average distance between SPG as seen on the MRI images and the estimated position based on CT images were 1.82 mm (SD 0.83, range 0.22–3.57 mm) for vcSPG and 2.09 mm (SD 0.99, range 0.71–4.79 mm) for sSPG.
Conclusions:
The localization of the SPG can be predicted on CT images using bony landmarks. Localization of the SPG may be important in achieving successful therapeutic outcomes for treatments that are directed toward the SPG.
Introduction
The sphenopalatine ganglion (SPG) is the target for the treatment of several headache conditions. 1 The SPG is situated in the sphenopalatine fossa, which is a complex anatomical region deep in the face behind the maxillary sinus. The SPG cannot be visualized on fluoroscopic or computerized tomography (CT) images due to its tissue properties and size. This makes it a challenge to target the SPG (Figure 1), and most of the techniques targeting this structure are performed without knowing its exact position (Table 1). 24 Some authors have used fluoroscopic guidance or CT-guided techniques, but the anatomical landmarks are not properly validated or standardized. Bratbak et al. have localized the SPG in magnetic resonance imaging (MRI) images in living humans for the first time 25 and used the exact localization of the SPG in a novel technique in two pilot studies. 2,3

Illustration showing the anatomical structures surrounding the SPG in an axial plane. SPG: sphenopalatine ganglion.
Technique used to localize the sphenopalatine ganglion in different studies that have targeted it.
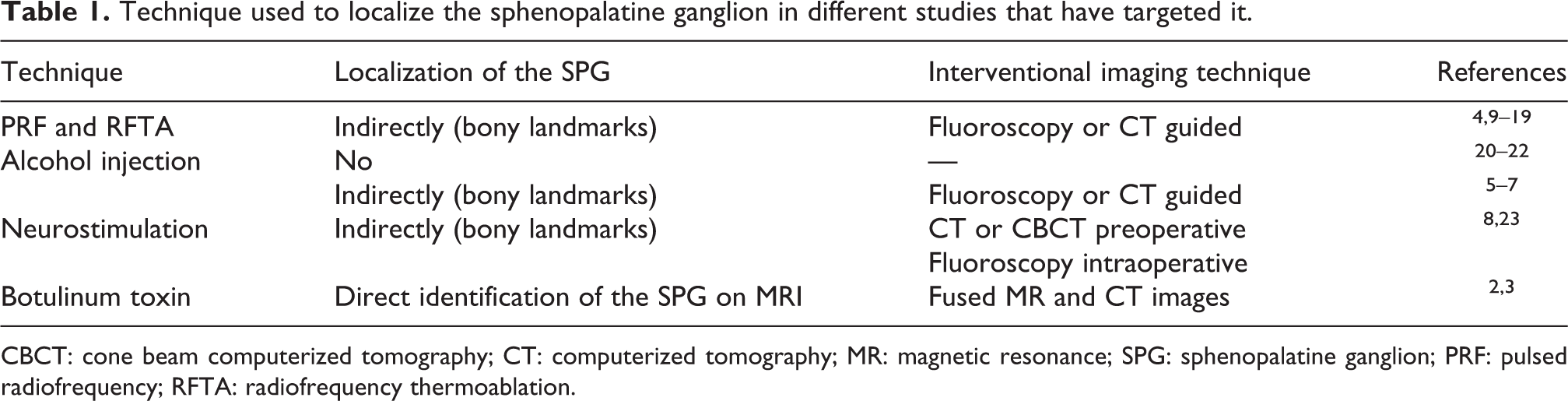
CBCT: cone beam computerized tomography; CT: computerized tomography; MR: magnetic resonance; SPG: sphenopalatine ganglion; PRF: pulsed radiofrequency; RFTA: radiofrequency thermoablation.
Access to MRI is limited in many countries, 26 and some patients cannot be examined with MRI due to metallic implants, 27 foreign bodies, 28 or claustrophobia. 29 Furthermore, CT scans are more accessible both in number and in cost than MRI. Thus, it would be highly valuable to be able to predict the localization of the SPG using CT scans.
In this study, we evaluate two different methods for predicting the position of SPG on CT scans by measuring the distance in three planes between the SPG and two different landmarks and calculating the distance between the known position as identified on MRI and the predicted position for the two methods.
Methods
Written informed consent was obtained from all patients. All patients were recruited from four clinical trials approved by the Central Norwegian Regional Ethical Committee (ref. 2012/164, 2014/962, 2015/1193, and 2015/2018) and registered at ClinicalTrial.gov (NCT02019017, NCT02259075, NCT02662972, and NCT02784262). None of the patients had previously had any invasive procedure toward the SPG.
All 27 patients included in clinical studies targeting the SPG at St Olavs University Hospital from 2013 to 2017 were screened. MRI and CT scans had been performed on all patients to enable the study treatment, MRI was performed according the protocol as described by Bratbak et al. 25 for identification of the SPG. The MRI scans were assessed independently by two observers. To avoid the introduction of errors, only sides where both observers were positively certain of the position of the SPG were included. All measurements were done by JCV and DB, and in case of discrepancies, average values were used.
We first localized the SPG on 3 tesla MRI scans in 38 sides. MRIs were fused with CT images using Brainlab iPlan 3.0 (Brainlab AG, Feldkirchen, Germany). Correct co-registration was controlled visually by two physicians (JCV and DB). MRIs and CT scans were obtained on the same day and in all cases prior to intervention. The coordinates of the center of the SPG on an axial plan and two bony landmarks were calculated using Brainlab iPlan 3.0. We used the coordinates to measure the distance in three planes from the center of the SPG to two different bony landmarks identified on CT scans for each participant. We then applied the average distances of the cohort to find an estimated position of the SPG for each participant. The coordinates of the estimated and the real position of the SPG were used to calculate the absolute distance between the two positions using a free online 3-D Calculator Resource. 30 The chosen landmarks were the vidian canal (VC) and the sphenoidal bone. The VC was defined as the center of the anterior opening of the canal using both axial and sagittal CT images through the VC (Figure 2), and the predicted position of the SPG according to this method was referred to as vcSPG. The second landmark was a point on the sphenoidal bone (the S-point), which was defined in an axial plane at the level of the center of the VC as depicted in Figure 3. First, a line parallel to the sagittal plane was drawn (pink line in Figure 3), second, a line with an angle of 45° to the sagittal plane positioned as a tangent on the curvature of the sphenoidal bone laterally to the VC was drawn (cyan line in Figure 3), and the point of contact with the cortex of the sphenoidal bone was registered as the S-point (red point in Figure 3). Bratbak et al. have described the average distance from the center of the SPG to the nearest point of the posterior limitation of the sphenopalatine fossa in the same data set to be 1.6 mm. 25 Based on our measurements in this study, the SPG was depicted 1.0 mm inferior to the axial plane of the opening of the VC. According to these findings, the predicted position of the SPG according to this method was referred to as sSPG (green point in Figure 3) situated 1.6 mm from the S-point on the discontinuous yellow line (perpendicular to the cyan line) and 1.0 mm inferior to the S-point.

(a) Axial CT scan through the opening of the VC(red star); the blue star shows the localization of the SPG previously localized in fused MRIs. The distance between the opening of the VC and the SPG was measured using Brainlab iPlan 3.0 (represented with a yellow discontinued line). (b) Illustration showing an enlarged detail of the image on the left. (c) Parasagittal CT scan through the opening of the VC (green star). SPG: sphenopalatine ganglion; VC: vidian canal; CT: computed tomography.

Axial CT scan through the opening of the VC (enlarged detail on the right). A line parallel to the sagittal plane is drawn (pink line). Then a line with an angle of 45° to the sagittal plane is positioned as a tangent on the curvature of the sphenoidal bone laterally to the VC (cyan line), and the point of contact with the cortex of the sphenoidal bone is registered as the S-point (red point). The predicted position of the SPG (green point, referred in this article as sSPG) was 1.6 mm from the S-point on the discontinuous yellow line (perpendicular to the cyan line) and 1.0 mm inferior to the S-point. SPG: sphenopalatine ganglion; VC: vidian canal; CT: computerized tomography.
MR scans were performed on a 3-tesla scanner (Siemens’ Magnetom Skyra, Germany). Technical parameters were as follows: sagittal T2 weighted: repetition time (TR) range 3780, echo time (TE) 111, slice thickness 2 mm, matrix 0.4 × 0.4 × 2.0 mm3, field of view (FOV) 210, number of acquisitions 3; sagittal T1 weighted: TR range 710, TE 10, slice thickness 2 mm, matrix 0.4 × 0.4 × 2.0 mm3, FOV 210, number of acquisitions 2; axial T2 weighted: TR range 4160, TE 110, slice thickness 2 mm, matrix 0.4 × 0.4 × 2.0 mm3, FOV 220, number of acquisitions 2; and axial T1 weighted: TR range 710, TE 7.9, slice thickness 2 mm, matrix 0.4 × 0.4 × 2.0 mm3, FOV 210, number of acquisitions 2. All CT scans were performed using a helical CT scanner (Siemens’ Somatom sensation 64, Germany) set at effective mAs 63, 120 kV, slice thickness 1 mm, reconstruction increment 0.7 mm, collimation 12 × 0.6 mm2, Kernel U 70, window width 1750.0 HU and window level 450.0 HU.
Statistical analysis
SPSS version 24.0 (SPSS Inc., Chicago, Illinois, USA) was used in the data analyses. Data distributions are expressed as means and standard deviations (SDs). Results are given as mean ± SD if not otherwise stated.
Results
The demographics of the sample are described in Table 2. Both investigators were positively certain of the position of the SPG on MRI in a total of 38 sides (21 right and 17 left SPG) in 21 patients (Figure 4). A total of 16 sides were rejected due to uncertainty of position among both investigators. The average distances from bony landmarks to the SPG are depicted in Table 3. The average distance between the SPG, as located in MRI images, and the estimated position based on measurements from the VC (vcSPG) and the sphenoidal bone (sSPG) was, respectively, 1.82 mm (SD 0.83; range 0.22–3.57 mm) and 2.09 mm (SD 0.99; range 0.71–4.79 mm).
Demographics and clinical characteristics of the sample.
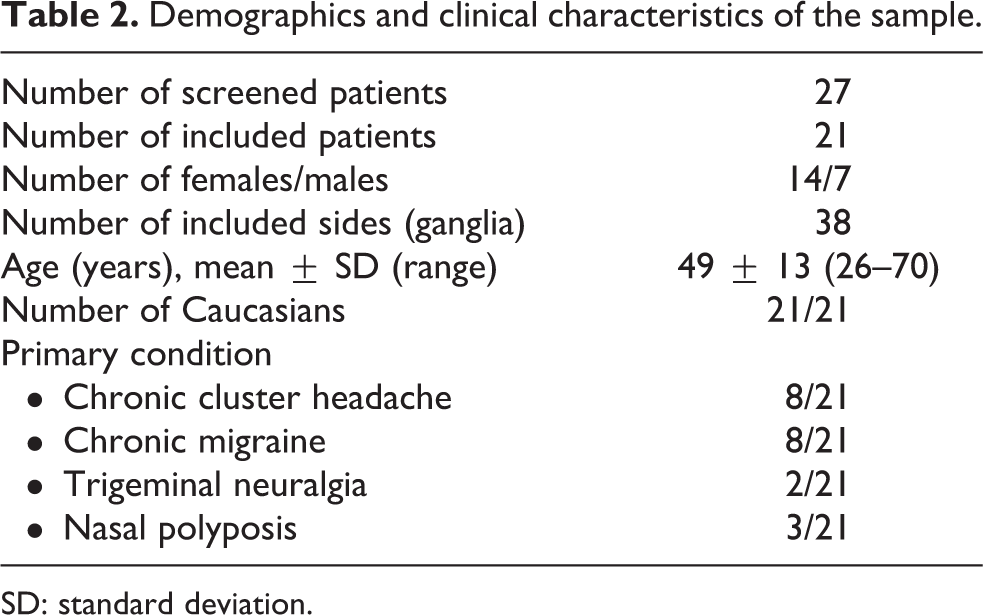
SD: standard deviation.

Patients included in the study. SPG: sphenopalatine ganglion.
Average distances ± SD from bony landmarks to the pterygopalatine ganglion (SPG) in all three planes.

VC: vidian canal. X: lateromedial; Y: craniocaudal; Z: anterioposterior; SPG: sphenopalatine ganglion.
No statistically significant differences were observed between genders or side regarding the average distance between the SPG and the estimated SPG (an independent-samples Mann–Whitney U Test was used for this purpose).
Discussion
In this study, we show that the localization of the SPG can be predicted on CT images using bony landmarks. The center of the anterior opening of the VC and the point on the cortical aspect of the sphenoidal bone (described as S-point in this article; red point in Figure 3) appear to be reliable anatomical landmarks to predict the position of the SPG. In this study, we find that the VC is more accurate than the S-point when one tries to predict the localization of the SPG with a more favorable mean distance (1.82 mm vs. 2.09 mm, respectively) and a narrower range (0.22–3.57 mm vs. 0.71–4.79 mm). This might be because the opening of the VC is a more constant anatomical landmark.
Even though the SPG has been the target for treating headache for more than a century, 31 it has regained interest in the last decade with the development of several novel interventions. Most of these interventions do not localize the SPG and only recently has the SPG been identified in living humans on MRI 25 and exploited with the aim of increasing accuracy when targeting the SPG. 2,3 Most of the authors targeting the SPG rely on cadaveric descriptions where the SPG has been assumed to lie in the sphenopalatine fossa right under the sphenopalatine foramen. 31 However, these descriptions are vague and the location of the SPG in cadaveric studies might be different than its location in vivo as a result of postmortem desiccation. 24
The ability to accurately predict the location of the SPG on CT scans, based on validated anatomical landmarks in vivo, would be highly advantageous for those using CT-guided techniques. This should optimize the accurate delivery of the treatment and optimize patient outcomes. Fewer side effects may also be expected if correction(s) of the position of the needle during the procedure is avoided. Even though the SPG cannot be identified on CT scans, our results show that the localization of the ganglion can be accurately predicted. Being able to use CT images instead of MRI would make it easier to target the SPG in locations with limited access to MRI 26 or in patients who have contraindications to MRI. 27 –29
Depending on the therapeutic strategy, different levels of precision might be acceptable when predicting the localization of the SPG. For instance, using the methods described in this article, an error of 1.82 mm (SD 0.83, range 0.22–3.57 mm) or 2.09 mm (SD 0.99, 0.71–4.79 mm) might be acceptable for most injected drugs, because these distances will probably be overcome by the diffusion of the drug.
All studies using pulsed radiofrequency (PRF) and radiofrequency thermal ablation (RFTA), as depicted in Table 1, have used either fluoroscopy or CT-guided punctures to place the tip of the needle toward the SPG. It has been described that the correct placement of the needle can be achieved by stimulation, as the stimulation of the SPG produces paresthesia in the root of the nose. 4 This does not need to be due to the correct placement of the needle at the SPG, because stimulation anywhere along the posterior lateral nasal nerves on its course from the SPG to the sphenopalatine foramen would elicit paresthesia in the same region. In addition, the technique depends on the patient’s subjective sensory perception and has never been validated. One can speculate that treatments using PRF or RFTA would be optimized using navigation toward the SPG with validated anatomical landmarks, achieving better results and reducing the risk for complications.
Other groups have injected various substances such as alcohol toward the SPG using CT-guided techniques. 5 –7 The anatomical landmarks used by these groups have not been validated. Whether CT-guided interventions toward the SPG are more effective and safer than other techniques should be evaluated in a randomized controlled trial.
In a publication describing a technique to implant a stimulator targeting the SPG, 8 the authors claim that the putative location of the SPG is “typically located posterior to the middle nasal turbinate, between the VC and the foramen rotundum.” This assumed topography has not been validated in vivo. Whether the use of the proposed anatomical landmarks in this study would increase the precision when inserting such stimulators toward the SPG may deserve further investigations.
Limitations of the study
All 21 patients in this study are White Caucasians, and this may constitute a limitation when extrapolating to other populations. On the other hand, it favors the homogeneity of the sample for internal analysis. Thirty percent of the sides were rejected, and 22% of the patients could not be assessed because of inability to come to consensus on the location/visualization of the SPG.
Another limitation of the study is the female predominance of the sample (14 females vs. 7 males), although no statistically significant differences were observed between genders regarding the average distance between the SPG and the estimated SPG.
The method of identification of the SPG on MRI has only been studied by our group 25 and has not been validated by others.
CT scans have a clear disadvantage compared to MRIs, that is, radiation of the patient. Nonetheless, the use of navigation-based approaches allows for repeated interventions without the need for fluoroscopy under each treatment. Moreover, a baseline CT scan can be used for consecutive treatments, thus reducing considerably the total amount of radiation.
In some patients, the SPG does not appear as a single macroscopic structure, 32 and this might be a limitation when using the methodology to localize the SPG described in this study or when using any other method that does not localize directly the SPG.
Conclusion
The localization of the SPG can be predicted on CT images using bony landmarks. The center of the anterior opening of the VC and the S-point (red point in Figure 3) appear to be reliable anatomical landmarks to predict the position of the SPG. Targeting the SPG has become more common and several randomized controlled trials utilizing a variety of treatment modalities are ongoing. To accurately predict the location of the SPG on CT scans will be important both in clinical trials and in clinical practice for those who choose CT-guided techniques. Being able to localize the SPG without the use of MRI will be valuable for those investigators and patients with limited access to MRI, for those patients with contraindications for an MRI and in those where repeated injections are needed. Further studies to validate this method in larger groups of patients are warranted.
Footnotes
Author contributions
JC, DB, and ET had the original idea for the manuscript. JC and DB analyzed the data. JC reviewed the literature for the introduction and discussion and drafted the manuscript. DB, DD, MM, KJ, and ET provided assistance for drafting the manuscript and revision of the text. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The results of this study may affect opinions on the feasibility of interventional treatments targeting the SPG. An intervention device for image-guided injections of pharmacological substances towards the SPG is developed at NTNU and St. Olavs Hospital, Trondheim University Hospital. These institutions may benefit financially of a commercialization of the device through future possible intellectual properties, this may include financial benefits to authors of this article. Dr Bratbak is co-inventor of a proposed treatment targeting the SPG and the intervention device used to perform the treatment, both inventions patent pending, and may benefit financially of a commercialization of the proposed treatment through future possible intellectual properties. Dr Tronvik may benefit financially of a commercialization of a proposed treatment targeting the SPG and the intervention device used to perform the treatment through future possible intellectual properties. Within the last 12 months, Dr Dodick reports personal fees from Amgen, Alder, Allergan, Autonomic Technologies, Biohaven, Eli Lilly, eNeura, Foresight Capital, Neurolief, Zosano, WL Gore, Vedanta Associates, Promius Pharma, Nocira, Novartis, Electrocore, Teva, Ipsen, Impel, Satsuma, Theranica. Compensation for activities related to data safety monitoring committee from Axsome. Compensation related to CME content development: Healthlogix, Medicom Worldwide, Medlogix Communications, MedNet, Miller Medical Communications, PeerView Operation Services America, Web MD/Medscape, American Academy of Neurology, American Headache Society, PeerView Institute for Medical Education, Chameleon Communications, Academy for Continued Healthcare Learning, Universal Meeting Management, Haymarket Medical Education, Global Scientific Communications, UpToDate, Meeting LogiX. Royalties from editorial or book publishing: Oxford University Press, Cambridge University Press, Wiley Blackwell, Sage, Wolters Kluwer Health. Consulting use agreement through employer: NeuroAssessment Systems, Myndshft. Equity (stock options): Aural Analytics, Healint, Theranica, Second Opinion/Mobile Health, Epien, Ontologics. Board of Directors position: King-Devick Technologies, Epien, Ontologics. Dr Crespi, Dr Jamtøy and Dr Matharu have no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant given by Norwegian University of Science and Technology (NTNU) and “The Liaison Committee for Education, Research and Innovation in Central Norway” (Samarbeidsorganet; grant number 46056923).