
Abstract
Background:
The quality of life of migraine patients, particularly mental domains, is severely diminished despite the preventive therapies available. We aimed to evaluate whether citalopram plus nadolol is superior to nadolol alone in terms of quality of life (QOL) in migraine patients.
Methods:
Adult patients with episodic migraine (≥ 3 headache days per month) were allocated by simple randomization to nadolol 40 mg daily plus citalopram 10 mg daily or to nadolol alone. Baseline visit confirmed the entry criteria and patients filled out a generic QOL (SF-36) as well a migraine-specific questionnaire (MSQoL), a measure of migraine-related disability (MIDAS), a headache calendar and Beck inventory for depression and anxiety. This battery was again completed after 16 weeks of therapy.
Results:
A total of 92 patients from a general neurology clinic completed the study, 85% females with migraine without aura. Fourty-four (47.83%) patients were allocated to nadolol therapy, and 48 (52.17%) to the combination of nadolol plus citalopram. After therapy, both groups had a similar gain in quality of life (SF-36 and MSQOL), but combination therapy was not superior to nadolol. Despite this improvement, all SF-36 domains remained below the population norms in both groups.
Conclusion:
Adding systematically citalopram 10 mg daily to a conventional migraine preventive drug (nadolol) does not result in an additional improvement in the QOL of migraine patients.
Introduction
Migraine is a major health problem representing the second most common neurological condition causing disability after stroke. 1 Migraine affects approximately 12% of the population worldwide and is highly comorbid with depression. 2 A meta-analysis of 12 original studies in 2011 found prevalence estimates of depression ranging from 8.6% to 47.9% in individuals with migraine and from 3.4% to 24.4% in individuals without migraine. 3
Despite important advances in therapy in the last decades, the quality of life (QOL) of patients with migraine remains severely deteriorated. 4 In addition to reducing the attack rate significantly, an effective preventive therapy should result in a significant improvement in the QOL of migraine patients. This objective is not often evaluated or achieved.
In a previous study, we showed that conventional preventive therapy significantly improved the physical domains of the SF-36 QOL questionnaire, while mental domains remained unchanged. 5 Despite this improvement, all QOL domains remained below the population norms. Also, patients had a moderate baseline depressive state that did not change with therapy. The extent to which depression may contribute to QOL impairment has not been properly assessed, and it remains unclear whether treating comorbid depression would result in improvement of the QOL of migraine patients.
In this study, we sought to investigate whether adding an antidepressant drug systematically to conventional preventive therapy with a beta blocker agent would improve the QOL of migraine patients in a population unselected for depression.
Patients and methods
This was a single-blinded, prospective study in adult patients (
Study patients
Patients who met the criteria of the IHS for episodic migraine with or without aura and in whom the clinician felt there was a need for preventive therapy were invited to participate in this study. Patients were naive in terms of migraine prevention and had no preventive medication in the 6 months prior to the beginning of the study. Patients with analgesic overuse, as defined by the IHS criteria, were excluded, as were those patients who were not able to properly fill out the headache calendar properly. Those with a prior diagnosis of major depressive disorder were excluded as well. Patients were stratified according to their scoring in Beck depression scale for subsequent analysis.
Patients were referred from their primary physicians to our outpatient clinic of general neurology and, therefore, were unselected except for their migraine frequency and representative of a general sample of migraine patients. Patients were recruited consecutively in the Department of Neurology of our hospital, a publicly funded community hospital serving a population of 300,000.
Schedule of the study
During visit 1 (screening), patients were evaluated by one of the neurologists (JCGM) who verified that they met the criteria for episodic migraine (with or without aura), that they needed preventive therapy, and that they had no contraindication for the use of a beta blocker agent (i.e. asthma, prior hypersensitivity to beta blockers or any other condition that would preclude using these agents).
Patients were instructed about the appropriate abortive therapy, which consisted of nonsteroidal anti-inflammatory drugs or triptans. Patients were directed to take one of them and leave the other as rescue medication, according to the usual clinical practice. If patients were already on acute attack medication, pertinent modifications were introduced if needed.
A headache calendar was given for a period of 6 weeks on which patients recorded the frequency (attacks per month) and characteristics of migraine attacks. The study was explained to the patient, and informed consent was obtained. Any medication with possible migraine preventive effect was forbidden. Fertile women were required to practice an acceptable method of birth control before study entry. Prior diagnosis of depression requiring specific therapy was also an exclusion criterion.
During visit 2, scheduled 6 weeks later, the need for preventive therapy was confirmed with the calendar. At this point, patients filled out the questionnaires of QOL (SF-36 and migraine-specific QOL (MSQOL)) and of depression (Beck Depression Inventory (BDI)). Therapy with nadolol 40 mg/day titrated over 2 weeks was prescribed as clinically indicated. The optimal dose of nadolol is not well established, with a wide range in published studies. Our own experience with greater than 700 patients treated with this drug (unpublished results) indicates that a dose of 40 mg/day provides a good risk–benefit profile. A simple randomization scheme was employed to allocate the required sample of patients to also receive citalopram 10 mg daily in addition to nadolol. Citalopram was selected because it has not shown efficacy in migraine prevention 6 and has a good profile of tolerability and few interactions. The 10 mg dose was selected because it has a proven antidepressant effect, good antianxiety properties, and tolerability in a general population of migraineurs, keeping in mind that most of them would predictably have mild-to-moderate depressive or anxiety symptoms. Otherwise, they should be treated separately from this study and likely would require higher doses.
Nadolol is a beta adrenergic–receptor antagonist with a similar effectiveness to propranolol in migraine prevention but with the advantage of being administered only once daily.
Patients were kept on medication for 16 additional weeks, during which they kept a calendar and recorded the frequency (attacks per month) and characteristics of headaches as well as side effects.
At the end of the period, patients came back to the clinic for the final visit and again filled out the QOL questionnaires and the Beck’s questionnaires for anxiety and depression. The study was approved by our local Ethics Committee of the Institutional Review Board of our hospital.
Instruments of evaluation
We employed two questionnaires of QOL, one generic (SF-36) and one specific for migraine (MSQOL), as well as a scale to evaluate the degree of anxiety and depression (Beck).
SF-36
The SF-36 is a structured, self-report questionnaire that the patient can generally complete with little or no intervention from an interviewer. It includes 36 items measuring health across 8 domains of health status. The scoring system for the SF-36 is relatively complex and generates subscale scores for physical functioning (PF), role limitations due to physical problems (RP), bodily pain (BP), general health perceptions (GH), vitality (VT), social functioning (SF), role limitations due to emotional problems (RE), and mental health (MH). Two summary scores can also be derived from the SF-36: the physical component summary (PCS) and the mental component summary (MCS). Four scales (PF, RP, BP, and GH) contribute most to the scoring of the PCS measure. 7 The VT, SF, RE, and MH scales contribute most to the scoring of the MCS measure.
Summary scores allow a much simpler interpretation of results and are very useful when interpreting differences across scales in the SF-36 profile and for monitoring disease groups over time. The SF-36 scores range from 0 to 100, with a higher score indicating better health status. In addition, normalized values can be estimated so that it can provide a reference value from the general population. To do so, each SF-36 score was first standardized using the mean and standard deviations (SDs) obtained from the Spanish population, and then transformed to norm-based (mean = 50, SD = 10) scoring, as suggested by the authors of the questionnaire. 8 The SF-36 has been translated into Spanish and validated in Spanish populations, and the measurement properties have been published previously. 9 In addition, normalized values can be estimated so that it can provide a reference value from the general population. To do so, each SF-36 score was first standardized using the mean and SDs obtained from the Spanish population and then transformed to norm-based (mean = 50, SD = 10) scoring, as suggested by the authors of the questionnaire. 10
Migraine-specific QOL
The MSQOL questionnaire is a specific instrument that has been shown to be a valid and reliable measure in migraineurs. 11,12 Self-administered, it consists of 20 items, each of which is rated using a response scale with 4 categories (from 1 = very much to 4 = not at all). It has a multidimensional scale comprising 20 items grouped into 3 dimensions: avoidance (10 items), social relationships (6 items), and feelings (4 items). The scores were determined by adding the items for each domain. An overall score was also determined by adding the 20 items. The data were standardized to a range of values from 0 to 100, where 0 represents the worst health status and 100 the best health status. The original questionnaire has been translated and validated into Spanish. 11,13
Beck Depression Inventory
The BDI consists of 21 multiple-choice, self-reported questions and is one of the most widely used psychometric tests for measuring the severity of depression. Designed for individuals aged 13 and over, the BDI is composed of items relating to symptoms of depression such as hopelessness and irritability, cognitions such as guilt or feelings of being punished, and physical symptoms such as fatigue, weight loss, and lack of interest in sex. 14
BDI items are rated on a four-point scale ranging from 0 to 3 based on severity of each item. The maximum total score is 63. Scoring 0–13 indicates minimal depression, 14–19 mild depression, 20–28 moderate depression, and 29–63 severe depression. BDI has been validated in Spanish.
Beck Anxiety Inventory
The Beck Anxiety Inventory (BAI) consists of 21 items with a Likert-type scale ranging from 0 to 3 and raw scores ranging from 0 to 63. The BAI scores are classified as minimal anxiety (0–7), mild anxiety (8–15), moderate anxiety (16–25), and severe anxiety (30–63). It has been validated in Spanish.
Migraine Disability Assessment
This is a validated five-item questionnaire that is easy to use in practice and evaluates the impact and disability that migraine produces on the lives of patients. 15
Statistical analysis
The sample was divided in two subsamples according to the treatment given to the patients (nadolol vs. nadolol and citalopram). Descriptive statistics for the entire sample and for both subsamples were measured by mean and SDs for continuous variables, while frequencies and percentages were used for categorical data. Comparisons between groups of patients according to sociodemographic variables and headache history of the patients were evaluated using Student’s t-test (or nonparametric Wilcoxon test, when normality was rejected) for continuous variables, whereas χ 2 test (or Fisher’s exact test, when expected frequencies were lower than 5) was used for categorical variables.
QOL questionnaires such as SF-36, MSQOL, migraine disability assessment (MIDAS), and Beck for anxiety and depression were evaluated in two different times (before and after 16 weeks of therapy). At both points in time, differences between groups of patients were evaluated using Student’s t-test (or nonparametric Wilcoxon test, when normality was rejected), since all the questionnaires were measured by continuous scores. χ 2 test (or Fisher’s exact test, when expected frequencies were lower than 5) was used for anxiety and depression scales when they were measured as categorical variables. Also, in each group, differences between baseline visit and second visit were evaluated using the nonparametric Wilcoxon-signed rank test for related samples. The same procedure was repeated for patients with a moderate or severe depression in baseline, as measured by the BDI.
All effects were deemed significant at p < 0.05. All statistical analyses were performed using SAS 9.4 software (SAS Institute Inc., Cary, NC, USA).
Sample size calculation
Based on our previous results, 4 and considering an alpha of 0.05, a power of 0.8, a size effect of 4 points in therapeutic gains in the QOL (SF-36 or MSQOL) tests. A dropout of 10% was estimated, and using Student’s t-test to compare the mean between two groups, the required sample size was 45 patients on each group.
Results
One hundred patients were consecutively recruited, of whom 92 completed the study. Forty-four (47.83%) patients were allocated to nadolol therapy, and 48 (52.17%) to the combination of nadolol + citalopram. Most of the patients were women (84.78%) with a diagnosis of migraine without aura (Table 1). There were no significant differences between both groups according to sociodemographic and associated medical conditions or to the history of headache and migraine drugs utilization. Migraine severity was similar in both groups as indicated by the MIDAS scores (Table 2).
Descriptive analysis of the patients.
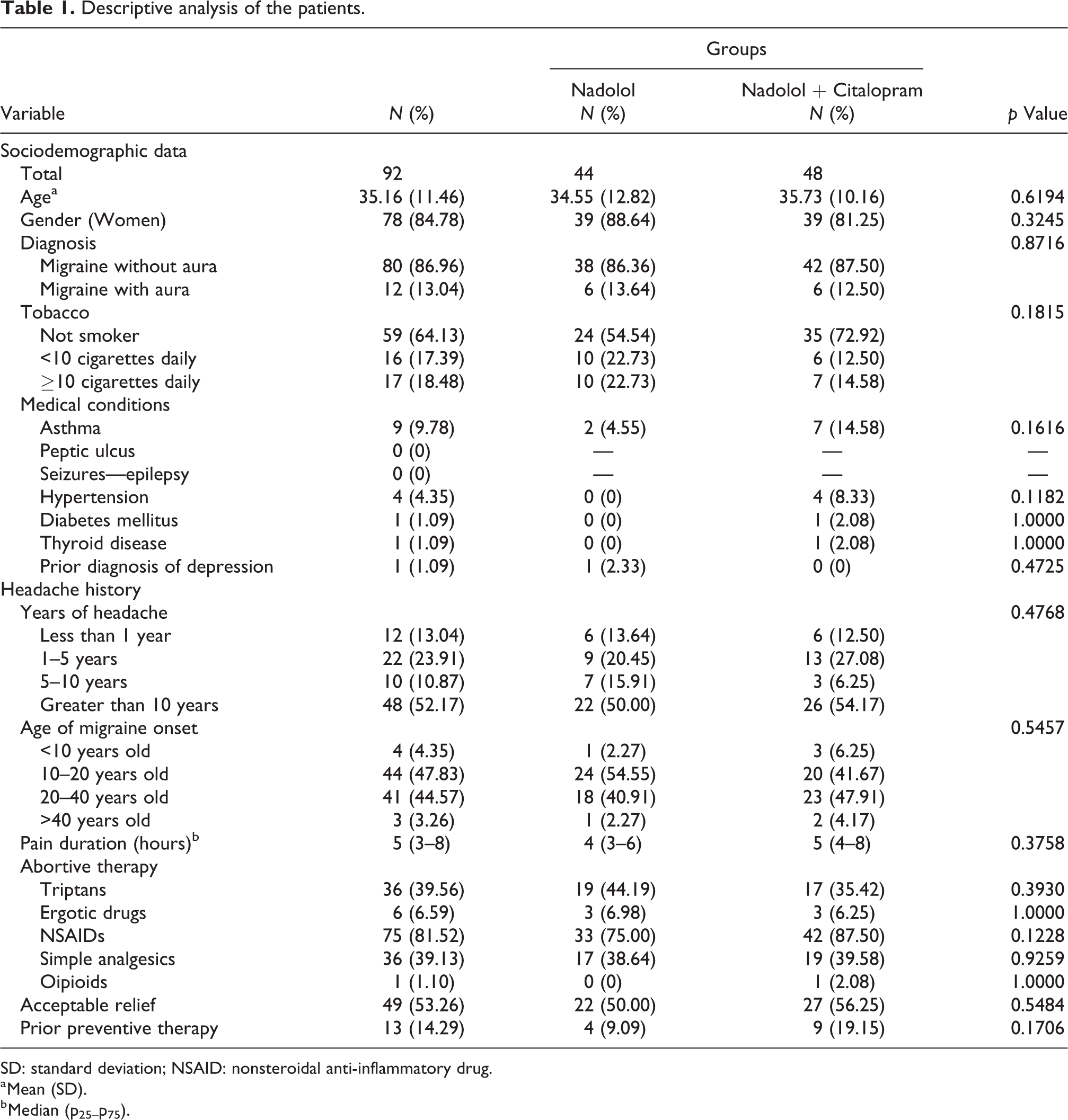
SD: standard deviation; NSAID: nonsteroidal anti-inflammatory drug.
a Mean (SD).
b Median (p25–p75).
QOL before and after therapy according to the two groups and differences between the two visits.a

PF: physical functioning; RP: physical role; BP: bodily pain; GH: general health perceptions; VT: vitality; SF: social functioning; RE: emotional role; MH: mental health; PCS: physical component summary; MCS: mental component summary; QOL: quality of life; MSQOL: migraine-specific QOL; MIDAS: migraine disability assessment; SD: standard deviation.
a Results are shown as mean (SD).
b Statistically significant differences are in change from visit 1 to visit 2.
At baseline (visit 1), no significant between-group differences were observed in the scoring of the QOL questionnaires or Beck inventories for depression or anxiety (Table 2).
At visit 2, both groups had a similar gain in QOL, but combination therapy was not superior to therapy with nadolol alone as reflected by the lack of statistical significance in the scoring change from visit 1 to visit 2.
It was interesting to note that all the SF-36 domains showed a statistically significant improvement in each group after completing 16 weeks of therapy. Along these lines, the mean score of MH subscale and mental component scales of the SF-36 questionnaire in patients with nadolol was higher than in patients with nadolol and citalopram, although the difference did not reach statistical significance (p = 0.0625 and p = 0.0593, respectively). Figure 1 depicts the norm-based SF-36 scores at visits 1 and 2 in both groups and shows that despite the improvement after therapy, patients remain below the general population in terms of QOL as measured by the SF-36.

Norm-based SF-36 scores at visits 1 and 2, according to therapy. General population score ≥50 on each item. PF: physical functioning; RP: physical role; BP: bodily pain; GH: general health perceptions; VT: vitality; SF: social functioning; RE: emotional role; MH: mental health.
The MSQOL also showed a clear improvement in both groups after therapy, although there were not significant between-group differences. The impact of migraine on patients was clearly favorable after 16 weeks of therapy as indicated by a reduction in the MIDAS scores.
According to Beck inventories, both groups showed less anxiety and depression from visit 1 to visit 2, after 16 weeks of therapy. At visit 2, the mean BDI score of the patients with nadolol treatment was 6.26 (SD 6.93), while for patients with nadolol and citalopram, the mean score was 9.08 (SD 7.10). However, this study was not powered to evaluate depression changes as a main outcome and, therefore, we cannot interpret this finding properly. Furthermore, the change in scores both for depression and anxiety did not reach statistical significance (Table 2). The improvement that both groups showed in depression and anxiety scores may have reflected indirectly their migraine improvement.
Patients were stratified according to their BDI scores, since most of the patients had mild or moderate depression scores. Results are presented in Table 3. Again, both groups showed an improvement in the different domains of the SF-36 and MSQOL and Beck inventories, but none of the groups was statistically superior. The benefit in terms of migraine impact as measured by the MIDAS scores was also present in both groups with no between-group differences.
QOL before and after therapy according to the two groups and differences between the two visits in patients with mild or moderate depression.a

PF: physical functioning; RP: physical role; BP: bodily pain; GH: general health perceptions; VT: vitality; SF: social functioning; RE: emotional role; MH: mental health; PCS: physical component summary; MCS: mental component summary; QOL: quality of life; MSQOL: migraine-specific QOL; MIDAS: migraine disability assessment; SD: standard deviation.
a Results are shown as mean (SD).
b Statistically significant differences are in change from visit 1 to visit 2.
Discussion
The main objective of this study was the evaluation of QOL after therapy with a conventional drug (nadolol) against a combination of nadolol and citalopram. Our results showed that the null hypothesis could be rejected, since addition of an antidepressant without preventive properties for migraine to a conventional preventive drug (nadolol, a beta blocker) did not result in a significant improvement in QOL measures, either with a generic questionnaire—SF-36—or with a specific one, the MSQOL.
Patients in both groups showed a benefit in terms of migraine prevention, that is, there was a significant reduction in the number of headache days after completing 16 weeks of therapy, as well as an improvement in MIDAS scores, reflecting less disability on the patients’ lives. However, the combination therapy was not superior to nadolol alone.
Along with these lines, the QOL of patients improved after therapy but again combination therapy was not superior. We evaluated the QOL by employing a widely used questionnaire, the SF-36, in which physical and emotional domains are considered. All these domains’ scores showed an improvement over time but without differences between groups. Despite improving on the different domains of the SF-36 questionnaire, migraine patients remained below the general population scores after therapy, thus indicating the need for more effective preventive therapies in terms of QOL.
A specific migraine questionnaire was also employed, the MSQOL, which also showed a clear improvement in both therapeutic groups without differences between them. The results were replicated when patients were stratified to their scores on the BDI and those with mild or moderate scores were analyzed.
The scores of both BDI and BAI reflected a decrease in depression and anxiety with therapy to a similar degree in both groups, perhaps reflecting an indirect indication of a better sense of well-being due to migraine improvement. However, this study was not powered to evaluate the change on these variables as a main outcome.
Antidepressants, both in monotherapy and in combination with other drugs, may benefit diverse pathologies other than mood disorders, including neuropathic pain, smoking cessation, or tension-type headaches, among others. Of the many options in this family of drugs, we selected one with a good safety profile, few interactions, a clear mechanism of action limited to serotonin uptake (since it was to be used in combination with a beta blocker), and known lack of properties in migraine prevention.
Previous studies have shown a correlation between depression using the BDI and pain intensity and found some degree of depression in up to 85% of the patients. 16 Our migraine patients showed mild-to-moderate depression and anxiety scores. However, we are not aware of previous experience evaluating the role of antidepressants as add-on medication on migraine prevention, despite the well-known bidirectional effect of migraine and these psychiatric comorbidities. Whether migraine patients with severe depression would particularly benefit from this combination therapy remains to be explored.
It should be stressed that our main goal was to evaluate the impact on QOL of these interventions, not only their impact on the classical pain frequency measures. It is widely appreciated that migraine severely deteriorates the QOL of the migraineur, and every effort should be devoted to ameliorate this situation. Currently, the therapeutic options for migraine prevention are rather limited due to tolerability issues, not too many drugs available, and contraindications to their use. New approaches are clearly needed, and in this regard, humanized antibodies against the calcitonin gene-related peptide or its receptor have been developed, although the right candidates need to be identified. 17
Combination therapy in migraine prevention has occasionally been evaluated but always combining two conventional preventive drugs such as topiramate and beta blockers and with limited results in terms of effectiveness.
In conclusion, adding citalopram to the conventional beta blocker for prevention of migraine does not result in an increased QOL in the general population of migraine patients.
Clinical implications
Despite the high comorbidity of migraine and depression, adding citalopram to the conventional preventive drug (nadolol) does not improve the QOL of patients. The QOL of migraine patients is severely deteriorated and remains below the general population after preventive therapy. Much work needs to be done to improve the QOL of migraine patients and bring them closer to the general population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.